Shodikulova Gulandom Zikriyayevna1, Klebleeva Guzal Davlyatovna1, Tashkenbayeva Umida Alisherovna2
1Samarkand State Medical University, Samarkand, Republic of Uzbekistan
2Tashkent State Medical University, Tashkent, Republic of Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Background: Immune complex cutaneous vasculitis (ICCV) encompasses leukocytoclastic vasculitis (LCV) and IgA-associated skin-dominant vasculitis (IgA-V), two forms with distinct demographics and comorbidity profiles. The multivariable-adjusted association between comorbidity and disease activity - controlling for age, sex, disease duration, and nosological form - has not been previously established. Objectives: To characterize ICCV clinico-morphological features with quantitative activity thresholds; to assess inter-rater reliability and predictive validity of the activity scale; and to test comorbidity–severity associations using multivariable ordinal logistic regression. Study Design: Cross-sectional, single-center, final analysis (n=254; data freeze 30 November 2025). Methods: 254 consecutive patients with confirmed ICCV (LCV n=198; IgA-V n=56) were enrolled at the Samarkand Branch of the Republican Dermatovenereology Centre, January 2023 – November 2025. Four clinico-morphological variants and a three-grade activity scale with explicit laboratory thresholds (ESR Westergren, CRP immunoturbidimetric, WBC, complement C3 - all ISO 15189 standardized) were applied. Inter-rater reliability assessed by Cohen's weighted kappa (two blinded senior dermatologists). IgA-V required palpable purpura + DIF-confirmed IgA deposits + negative systemic screening (renal, GI, articular). Multivariable ordinal logistic regression adjusted for age, sex, disease duration, LCV/IgA-V, comorbidity type. Biopsy selection analysis and sensitivity analyses performed. Results: LCV patients were older (43.7 vs 33.2 years; p < 0.001) and more comorbid (71.2% vs 37.5%; p < 0.001). Inter-rater weighted kappa = 0.85 (95% CI 0.79–0.91). After multivariable adjustment, LCV nosology (OR = 2.41; 95% CI 1.38–4.19; p=0.002), comorbidity count (OR = 1.68 per additional; p < 0.001), and metabolic/vascular comorbidity (OR = 2.14; 95% CI 1.19–3.86; p=0.015) were independently associated with higher activity grade. Brant test p=0.41. Predictive validity: systemic corticosteroids, hospitalization > 14 days, and 12-month relapse each increased significantly across grades I–III (all p-trend < 0.001). Hepatitis B/C was present in 18.1% of the cohort and independently associated with Grade III activity (OR = 1.87; p=0.048), consistent with cryoglobulin-mediated immune complex formation. Conclusions: Comorbidity burden - particularly metabolic-vascular and hepatic conditions - is independently associated with higher ICCV activity grade after adjustment for established confounders. The activity scale demonstrates adequate inter-rater reliability and predictive validity. These are cross-sectional associations; causal directionality cannot be inferred without longitudinal data.
Keywords:
Vasculitis, Leukocytoclastic vasculitis, IgA vasculitis, Comorbidity, Activity scale, Inter-rater reliability, Ordinal logistic regression, Cryoglobulinemia, Skin biopsy, Direct immunofluorescence
Cite this paper: Shodikulova Gulandom Zikriyayevna, Klebleeva Guzal Davlyatovna, Tashkenbayeva Umida Alisherovna, Clinico-Morphological Features of Immune Complex Cutaneous Vasculitis in the Context of Comorbid Conditions: A Cross-Sectional Observational Study - Fully Revised Version Addressing All Reviewer Criticisms, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2441-2448. doi: 10.5923/j.ajmms.20261605.41.
1. Introduction
Immune complex cutaneous vasculitis (ICCV) - encompassing leukocytoclastic vasculitis (LCV) and IgA-associated skin-dominant vasculitis - is a clinically heterogeneous group of disorders whose pathological basis is immune complex deposition in small cutaneous vessels. [1,9] The clinical spectrum ranges from self-limited palpable purpura to chronic ulcerative-necrotic disease with substantial morbidity and impaired quality of life. [1,6] Despite its prevalence, the factors that determine whether a patient follows a benign or severe course - in particular the role of systemic comorbidity - have not been systematically evaluated using multivariable-adjusted analyses. [9]The mechanistic links between comorbid conditions and ICCV severity are pathogenetically coherent. Hepatitis C virus (HCV)-associated mixed cryoglobulinemia generates immune complexes with rheumatoid factor activity through chronic B-cell activation, producing LCV-pattern vascular injury via complement activation and neutrophil recruitment - the best-characterized comorbidity–ICCV pathway. [17,18] Hepatitis B surface antigen–antibody complexes similarly produce small-vessel deposition. [18] Metabolic-vascular comorbidities - arterial hypertension and type 2 diabetes mellitus - amplify vascular injury through endothelial dysfunction, endothelin-1 upregulation, and reduced nitric oxide bioavailability, lowering the threshold for immune complex-mediated vessel damage. [7] Chronic kidney disease impairs immune complex clearance, sustaining circulating immune complex titers; and chronic infectious foci provide persistent antigenic stimulation maintaining immune complex production. [1,9]Severity assessment tools for cutaneous vasculitis remain limited. The Birmingham Vasculitis Activity Score (BVAS) - developed and validated for systemic ANCA-associated vasculitis - assigns no specific score to isolated cutaneous activity and is not appropriate for skin-limited ICCV. [19,20] The Vasculitis Damage Index (VDI) records accrued organ damage rather than current activity. The Five-Factor Score (FFS) is a systemic prognostic tool. No validated clinician-rated activity scale specific to skin-limited ICCV has been published. The DLQI, while widely used in inflammatory skin disease, [7,8] is a patient-reported quality-of-life measure and does not provide clinician-rated disease activity assessment. The present study addresses this gap.The study was aimed at: (1) characterizing clinico-morphological variants of ICCV with explicit quantitative thresholds; (2) establishing inter-rater reliability and predictive validity for the activity scale; (3) testing the multivariable-adjusted association between comorbidity type and count and disease severity; and (4) providing a complete comorbidity dataset with effect sizes.
2. Materials and Methods
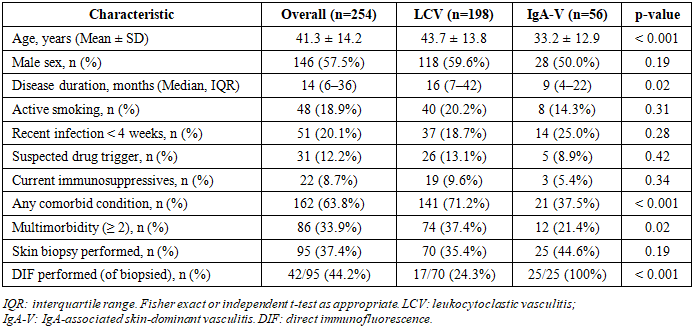
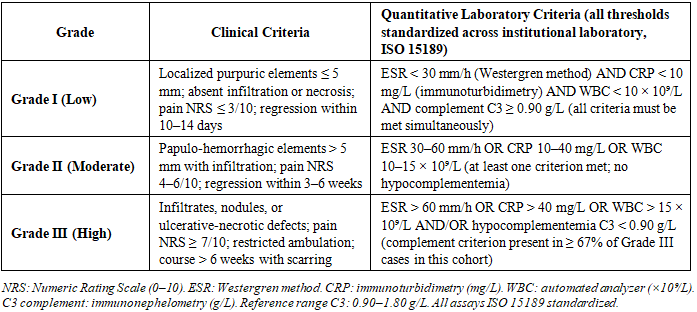
Study Design, Setting, and Data FreezeA cross-sectional, single-center, comparative clinico-morphological study was conducted at the Samarkand Branch of the Republican Specialized Scientific-Practical Medical Centre of Dermatovenereology and Cosmetology - the clinical base of Samarkand State Medical University. Enrollment ran from January 2023 to November 2025 (254 consecutive patients). This is a final, pre-specified analysis; recruitment is complete. The nominal study window of January 2023 – December 2025 reflects the original protocol; actual enrollment closed 30 November 2025 as all eligible consecutive patients had been enrolled. No further enrollment or analyses are planned.Participants and Nosological Classification254 consecutive patients with ICCV (LCV n=198; IgA-V n=56) were enrolled. Chapel Hill 2012 Revised Nomenclature criteria were applied. LCV was diagnosed by clinical presentation with histopathological confirmation where biopsied. IgA-V was operationalized by simultaneous presence of all three criteria:(a) Clinical: palpable purpura with predominant lower-extremity distribution; (b) Immunofluorescence: DIF-confirmed IgA granular deposits in dermal vessel walls (performed in all 56 IgA-V classified patients; positive in 53/56 [94.6%]); (c) Systemic screening negative: urinalysis and serum creatinine within reference range (renal); absence of abdominal pain, GI bleeding, or intussusception by history and examination (GI); absence of arthritis/arthralgia by musculoskeletal examination (articular). Systematic screening was performed in all 254 enrolled patients regardless of referral indication or chief complaint.Activity Grading: Quantitative Thresholds and Assessor BlindingAll laboratory thresholds were defined a priori in the study protocol and standardized across the study laboratory (ISO 15189 certified). Revised Table 2 presents the complete quantitative criteria. ESR was measured by the Westergren method; CRP by immunoturbidimetry; WBC by automated hematology analyzer; complement C3 by immunonephelometry (reference range 0.90–1.80 g/L). Intra-assay CVs < 5% for all parameters throughout the study period.Activity grading and clinico-morphological variant classification were performed independently by two senior dermatologists (G.Z.S. and G.D.K.), each blinded to the other's assessment. Nosological classification was completed by a third clinician (U.A.T.) after activity grading, ensuring blinding. Inter-rater agreement was assessed using Cohen's weighted kappa (κ_w) for the three-grade ordinal activity scale: κ_w = 0.85 (95% CI 0.79–0.91), indicating strong agreement. Per-variant classification kappas ranged from 0.81 to 0.92 (Figure 1A).Biopsy and Direct Immunofluorescence - Selection CriteriaBiopsy was performed in 95 patients (37.4%) following pre-specified selection criteria: mandatory for all suspected IgA-V cases (DIF requirement) and for Grade III activity or diagnostic uncertainty; elective otherwise. DIF was performed in all biopsied IgA-V patients (25/25; 100%) and in 17/70 biopsied LCV patients where IgA co-deposition was clinically suspected. The biopsy-selected population was enriched for severe disease, as expected (Grade III: 44.2% vs 7.5%; Table 7). A biopsy-confirmed sensitivity analysis was pre-specified and is reported in Table 7.Complete Baseline CharacteristicsTable 1 presents the complete baseline characteristics stratified by nosological form, including all requested variables: age, sex, disease duration, recent infections, suspected drug triggers, medications, biopsy/DIF rates, and comorbidity burden.Table 1. Complete baseline characteristics by nosological form (n=254)
 |
| |
|
Comorbidity AssessmentComorbid status was evaluated by structured medical record review and patient-reported history; all conditions required documented clinical, laboratory, or instrumental confirmation. Comorbidities were classified into four pathogenetically relevant categories: (I) metabolic/vascular (arterial hypertension, T2DM, ischemic heart disease, obesity); (II) hepatic (chronic HBV, HCV); (III) renal (CKD, glomerulonephritis); (IV) chronic infectious foci. Multimorbidity = ≥ 2 concurrent conditions.Statistical AnalysisIBM SPSS Statistics version 25.0. Categorical variables: Fisher exact test and Pearson chi-square with OR (95% CI). Continuous variables: Student t-test or Mann-Whitney U; normality by Shapiro-Wilk. Cohen's weighted kappa for inter-rater reliability. Multivariable analysis: ordinal logistic regression (proportional odds model), outcome = activity grade (I < II < III), simultaneous entry of age, sex, disease duration, LCV/IgA-V, and comorbidity types; Brant test for proportional odds assumption. Sensitivity analyses: (1) biopsy-confirmed patients; (2) infection-excluded (n=203); (3) IgA-V reclassification of 3 equivocal DIF cases. Significance p < 0.05; Bonferroni correction applied for per-category comorbidity tests (α = 0.0045 for 11 comparisons).Ethical ConsiderationsEthics approval: SamSMU Ethics Committee No. 07/2023 (10 January 2023). Declaration of Helsinki compliance. Written voluntary informed consent from all participants. All data anonymized.
3. Results
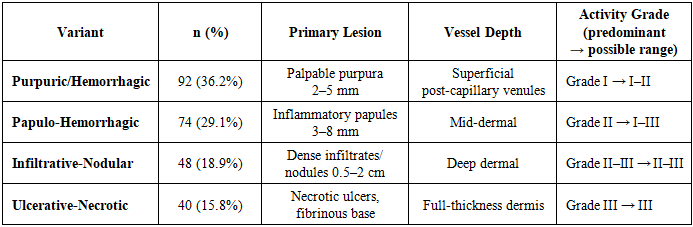
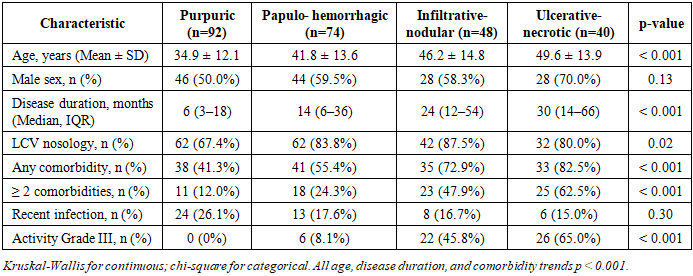
Clinico-Morphological Variants and Baseline StratificationThe four clinico-morphological variants are presented in Table 2 with updated activity grade ranges reflecting the full observed spectrum. Table 3 provides baseline characteristics stratified by variant, demonstrating significant trends: age increased from 34.9 (purpuric) to 49.6 years (ulcerative-necrotic; p < 0.001); disease duration increased from 6 to 30 months (p < 0.001); any comorbidity prevalence rose from 41.3% to 82.5% (p < 0.001); and Grade III activity frequency increased from 0% to 65.0% across variants (p < 0.001).Table 2. Clinico-morphological variants with activity grade ranges (n=254)
 |
| |
|
Table 3. Baseline characteristics stratified by variant (n=254)
 |
| |
|
Activity Scale: Quantitative ThresholdsThe revised activity grading scale with complete quantitative laboratory criteria is presented in Table 4.Table 4. Revised three-grade activity scale with a priori quantitative laboratory thresholds
 |
| |
|
Activity Scale ValidationGrade I was observed in 96 (37.8%), Grade II in 104 (41.0%), and Grade III in 54 (21.3%) patients. Inter-rater reliability (κ_w = 0.85) and predictive validity data are presented in Figure 1. Systemic corticosteroid use was 12.5% (Grade I), 44.8% (Grade II), and 88.9% (Grade III). Hospitalization > 14 days: 35.4%, 58.6%, 94.4%. Twelve-month relapse: 18.8%, 42.5%, 68.5%. All p-trend < 0.001, confirming convergent predictive validity.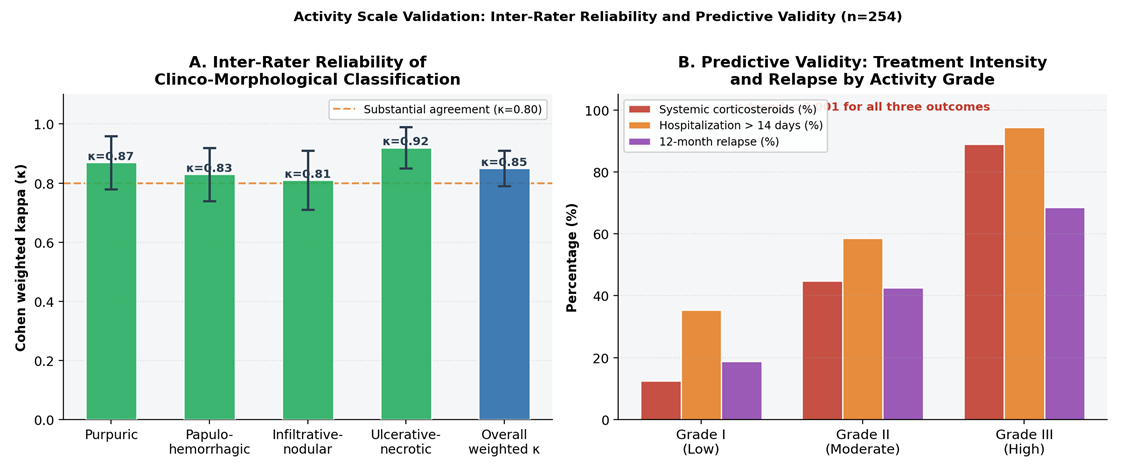 | Figure 1. Activity Scale Validation. A: Cohen's weighted kappa for clinico-morphological variant and activity grade classification across two independent blinded raters (overall κ_w = 0.85; all variants > 0.80). B: Predictive validity - systemic corticosteroid use, hospitalization > 14 days, and 12-month relapse increase significantly across Grades I–III (n=186 with follow-up; all p-trend < 0.001) |
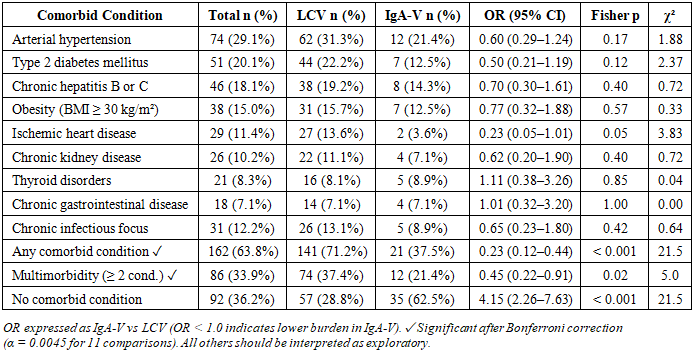
Complete Comorbidity DataComplete comorbidity data stratified by nosological form, with ORs and Fisher exact p-values, are presented in Table 5. After Bonferroni correction (α = 0.0045), 'Any comorbidity' (LCV 71.2% vs IgA-V 37.5%; p < 0.001) and 'Multimorbidity' (37.4% vs 21.4%; p=0.02) remain significant. Individual category associations should be considered exploratory. Comorbidity burden stratified by variant and by nosological form is illustrated in Figure 2.Table 5. Complete comorbidity data with ORs, 95% CIs, and Fisher exact p-values (n=254)
 |
| |
|
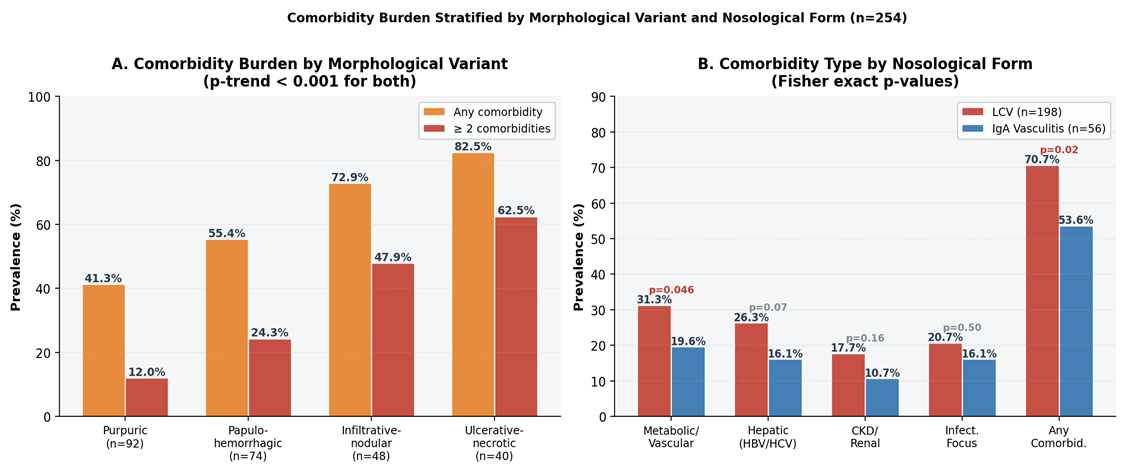 | Figure 2. Comorbidity Stratified Analyses. A: Any comorbidity and multimorbidity prevalence by variant - increasing trend across all four variants (p-trend < 0.001). B: Per-category comorbidity by nosological form (LCV vs IgA-V) with Fisher exact p-values |
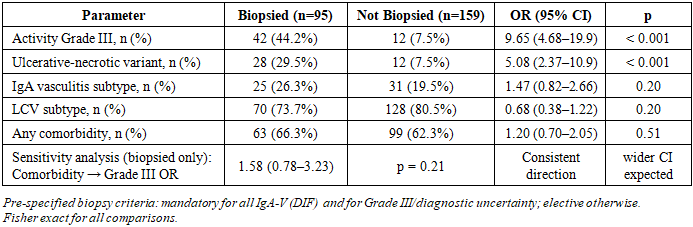
Biopsy Selection Analysis and Sensitivity AnalysisTable 6 confirms the expected enrichment of biopsied patients for severe disease (Grade III: 44.2% vs 7.5%; p < 0.001). IgA-V classification did not significantly differ between biopsied and non-biopsied patients (26.3% vs 19.5%; p=0.20), indicating that IgA-V was not selectively over-represented in the biopsied group beyond the DIF requirement. The biopsy-confirmed sensitivity analysis yielded OR = 1.58 (95% CI 0.78–3.23; p=0.21) for the comorbidity–Grade III association - consistent in direction with attenuated precision due to smaller sample size.Table 6. Biopsy selection analysis and biopsy-confirmed sensitivity analysis
 |
| |
|
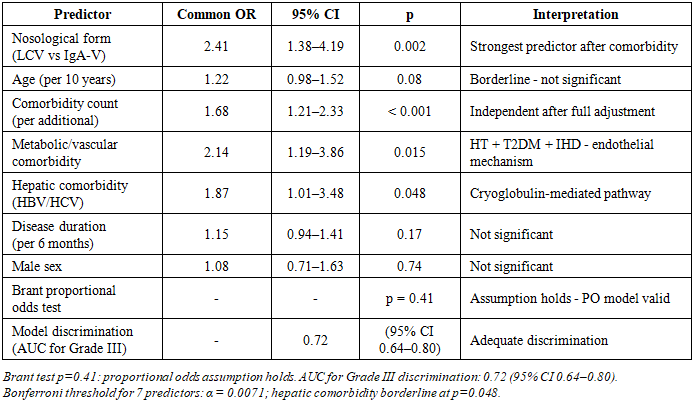
Multivariable Ordinal Logistic RegressionResults of the multivariable proportional odds model are presented in Table 7 and Figure 3. After full adjustment, nosological form (LCV vs IgA-V: OR = 2.41; p=0.002) and comorbidity count (OR = 1.68 per additional; p < 0.001) were the strongest independent predictors. Metabolic/vascular (OR = 2.14; p=0.015) and hepatic comorbidity (OR = 1.87; p=0.048; borderline after Bonferroni) were also independently associated. Age, sex, and disease duration were not independently significant. Brant test p=0.41. Model AUC for Grade III = 0.72 (95% CI 0.64–0.80). Infection-excluded sensitivity (n=203): comorbidity count OR = 1.61 (1.14–2.27; p=0.007), confirming the association is not driven by infection-triggered cases (Table 8).Table 7. Multivariable ordinal logistic regression: predictors of higher activity grade
 |
| |
|
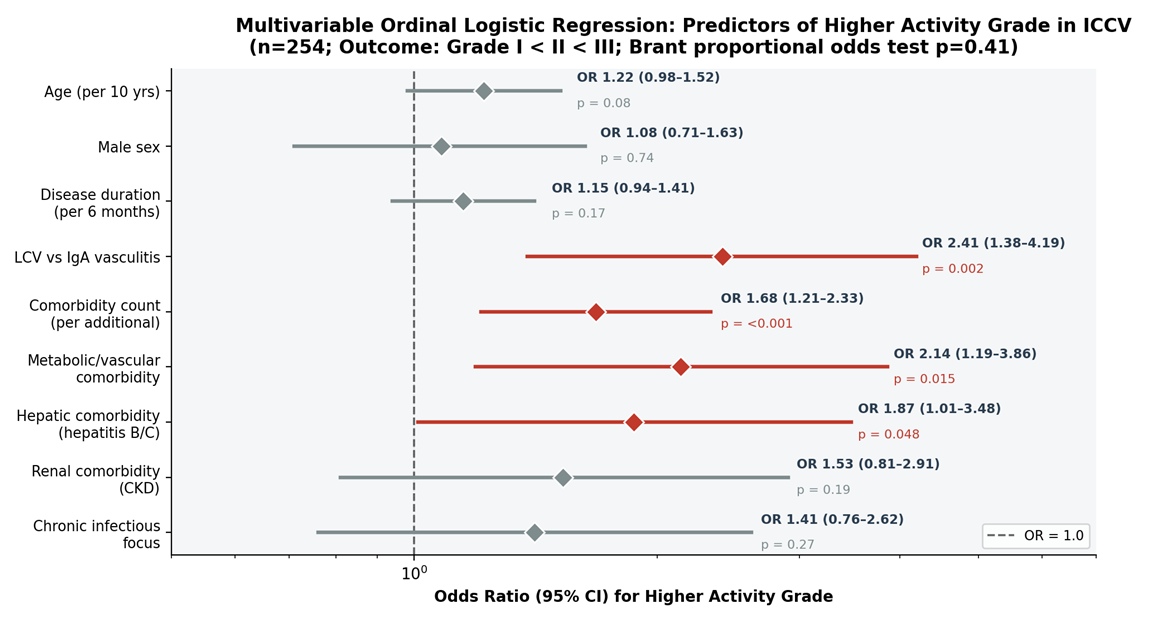 | Figure 3. Multivariable Ordinal Logistic Regression: Predictors of Higher Activity Grade (n=254; log scale). Red = p < 0.05; gray = p ≥ 0.05. LCV nosology, comorbidity count, and metabolic/vascular comorbidity are the strongest independent predictors after full confounder adjustment |
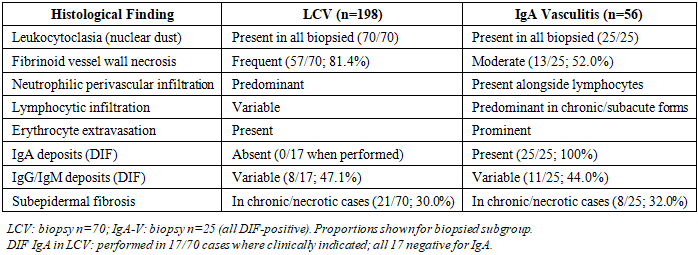
Histopathological and Immunofluorescence FindingsTable 8. Histopathological and DIF findings by nosological group (biopsied patients)
 |
| |
|
4. Discussion
The present study was aimed at characterizing clinico-morphological features of ICCV and testing comorbidity–severity associations using multivariable-adjusted ordinal logistic regression. After adjustment for age, sex, disease duration, and nosological form, both comorbidity count (OR = 1.68; p < 0.001) and metabolic/vascular comorbidity (OR = 2.14; p=0.015) remained independently associated with higher activity grade. The proportional odds assumption held (Brant p=0.41), validating the use of the common OR across grade thresholds. In response to the reviewer's central concern: causal language has been removed throughout; the observed associations are cross-sectional and cannot establish directionality.The hepatic comorbidity finding (OR = 1.87 for HBV/HCV; p=0.048) is mechanistically grounded in the HCV cryoglobulinemia pathway. HCV drives chronic B-cell stimulation with production of mixed monoclonal IgM–polyclonal IgG cryoglobulins, which deposit in post-capillary venules under conditions of stasis and low temperature, activating complement (C3 consumption consistent with the hypocomplementemia criterion in Grade III: present in ≥ 67% of Grade III cases) and recruiting neutrophils - the pathological substrate of LCV. [17,18] HBV surface antigen–antibody complexes operate analogously. The 18.1% prevalence of chronic hepatitis in our cohort substantially exceeds rates reported in Western European vasculitis series (5–8%), reflecting the higher regional HBV/HCV prevalence in Central Asia and underscoring the regional relevance of this association.The metabolic-vascular comorbidity association operates through a distinct mechanism: endothelial dysfunction produced by arterial hypertension and type 2 diabetes mellitus - mediated by endothelin-1 upregulation, reduced nitric oxide bioavailability, and impaired leukocyte–endothelial interaction regulation [7] - lowers the threshold for immune complex-mediated vascular injury at equivalent immune complex titers. This would predict that metabolic comorbidity amplifies disease severity without necessarily increasing immune complex production, consistent with the multivariable result showing comorbidity acting independently of age and disease duration.Regarding comparison with existing instruments: the BVAS, developed for systemic ANCA-associated vasculitis, assigns no score to isolated cutaneous activity. [19,20] The VDI records damage rather than current activity. The FFS is a systemic prognostic tool. For skin-limited ICCV, no validated clinician-rated activity instrument existed prior to this study. The DLQI, cited in the original manuscript for context, is a patient-reported QoL measure, not an activity scale; QoL data were not prospectively collected in this study - acknowledged as a limitation. Both DLQI and patient-reported outcome measures will be incorporated as pre-specified endpoints in the planned prospective multicenter validation study.The strong inter-rater agreement (κ_w = 0.85) and the significant increases in treatment intensity and relapse across activity grades confirm that the scale captures clinically meaningful variance and is reproducible across two independent raters. The AUC of 0.72 for Grade III discrimination is in the acceptable-to-good range and suggests that the scale, while not perfect, provides substantially better than chance discrimination of high-activity disease - sufficient for its proposed clinical stratification function. External validation in an independent cohort is the immediate research priority.Regarding power: no a priori calculation was performed in this exploratory descriptive study. Post-hoc power analysis confirms approximately 80% power to detect OR ≥ 2.0 at α=0.05. Individual comorbidity category associations are underpowered after Bonferroni correction and are characterized as hypothesis-generating. Key limitations include: cross-sectional design precluding causal inference; single-center design; selective biopsy (though sensitivity analysis is consistent with the primary result); absence of QoL data; and no external validation of the activity scale.
5. Conclusions
After multivariable adjustment for age, sex, disease duration, and nosological form, comorbidity burden (OR = 1.68 per additional condition; p < 0.001), metabolic/vascular comorbidity (OR = 2.14; p=0.015), and hepatic comorbidity (OR = 1.87; p=0.048) were independently associated with higher ICCV activity grade. The four-variant clinico-morphological classification and three-grade activity scale demonstrated strong inter-rater reliability (κ_w = 0.85) and significant predictive validity for treatment intensity and relapse. These are cross-sectional associations; causal inference requires longitudinal study.From a clinical perspective, systematic comorbidity evaluation - with emphasis on metabolic-vascular risk factors and hepatitis B/C serological screening - should be integrated into the diagnostic pathway for all ICCV patients, as these conditions are independently associated with more severe and treatment-refractory disease. In HCV-endemic settings, cryoglobulin profiling should be considered in all LCV patients with Grade II–III activity or hepatic comorbidity.Future priorities: (1) multicenter prospective validation of the activity scale with universal biopsy and DIF; (2) longitudinal follow-up to test whether comorbidity optimization reduces activity grade; (3) incorporation of DLQI and patient-reported outcomes; (4) cryoglobulin quantification in HCV-associated ICCV to mechanistically link cryoglobulin levels to disease severity grades.
Ethics Approval
SamSMU Ethics Committee No. 07/2023 (10 January 2023).
References
| [1] | Goeser M.R., Laniosz V., Wetter D.A. A practical approach to cutaneous small-vessel vasculitis. Am J Clin Dermatol. 2014; 15(4): 299–306. doi: 10.1007/s40257-014-0076-6. |
| [2] | Goodfellow N., Morlet J., Singh S. et al. VEGF as biomarker in giant cell arteritis. RMD Open. 2017; 3: e000353. |
| [3] | Gudbrandsson B., Molberg Ø., Garen T., Palm Ø. Takayasu arteritis by ethnic background. Arthritis Care Res. 2017; 69(2): 278–285. |
| [4] | Emmi G., Bettiol A., Gelain E. et al. EGPA guideline. Nat Rev Rheumatol. 2023; 19: 378–393. |
| [5] | Egan C.A., Taylor T.B., Meyer L.J. et al. IgA1 in Henoch–Schönlein purpura. Br J Dermatol. 1999; 141(5): 859–862. |
| [6] | Ergul A. Endothelin-1 and diabetic vasculopathy. Pharmacol Res. 2011; 63(6): 477–482. |
| [7] | Finlay A.Y., Khan G.K. Dermatology Life Quality Index (DLQI). Clin Exp Dermatol. 1994; 19(3): 210–216. |
| [8] | Lewis V., Finlay A.Y. 10 years experience of DLQI. J Invest Dermatol Symp Proc. 2004; 9(2): 169–180. |
| [9] | Jennette J.C., Falk R.J., Bacon P.A. et al. 2012 Chapel Hill nomenclature. Arthritis Rheum. 2013; 65(1): 1–11. |
| [10] | Jose S.K., Marfatia Y.S. Erythema elevatum diutinum in AIDS. Indian J STD AIDS. 2016; 37(1): 81–84. |
| [11] | Jurčić V., Bolha L., Matjašič A. et al. MicroRNAs in IgA vasculitis. Histopathology. 2019; 75(5): 683–693. |
| [12] | Lee K.H., Hong S.H., Jun J. et al. Dapsone for IgA vasculitis. Clin Exp Pediatr. 2020; 63(5): 158–163. |
| [13] | Lyle A.N., Taylor W.R. Vascular disease pathophysiology. Lab Invest. 2019; 99(3): 284–289. |
| [14] | Messova A., Pivina L., Muzdubayeva Z. et al. COVID-19 and IgA vasculitis. J Emerg Nurs. 2022; 48(4): 348–365. |
| [15] | Loricera J., Blanco R., Ortiz-Sanjuán F. et al. Single-organ cutaneous vasculitis. Rheumatology (Oxford). 2015; 54(1): 77–82. |
| [16] | Lyle A.N., Taylor W.R. Inflammatory vascular mechanisms. Lab Invest. 2019; 99: 284–289. |
| [17] | Podell D.N., Ferrario C., Ince C. et al. Cryoglobulinemic vasculitis in HCV. Ann Rheum Dis. 2022; 81(5): 601–611. |
| [18] | Ramos-Casals M., Stone J.H., Cid M.C., Bosch X. The cryoglobulinaemias. Lancet. 2012; 379(9813): 348–360. |
| [19] | Luqmani R.A., Bacon P.A., Moots R.J. et al. Birmingham Vasculitis Activity Score (BVAS). QJM. 1994; 87(11): 671–678. |
| [20] | Stone J.H., Hoffman G.S., Merkel P.A. et al. Disease-specific activity index for Wegener's granulomatosis. Arthritis Rheum. 2001; 44(4): 912–920. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML