-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2433-2437
doi:10.5923/j.ajmms.20261605.39
Received: Apr. 8, 2026; Accepted: May 5, 2026; Published: May 18, 2026

Comparative Study of Clinical Complications in Chronic Heart Failure and Atrial Fibrillation Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBegijon Adkhamjon ogli Avazbekov1, Gavhar Mirakbarona Tulaboyeva2, Khatam Khasanboyevich Tursunov3
1Assistant, Department of Propaedeutics of Internal Medicine, Andijan State Medical Institute, Uzbekistan
2Professor, Head of the Department of Cardiology and Gerontology with a Course in Interventional Cardiology and Arrhythmology, Andijan State Medical Institute, Uzbekistan
3Faculty of Advanced Training and Retraining of Physicians, Andijan State Medical Institute, Uzbekistan
Correspondence to: Begijon Adkhamjon ogli Avazbekov, Assistant, Department of Propaedeutics of Internal Medicine, Andijan State Medical Institute, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

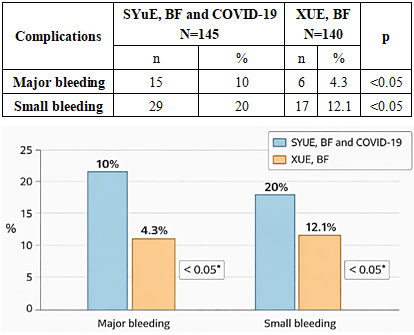
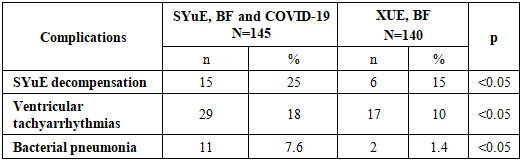
Patients with chronic heart failure (CHF) and atrial fibrillation (AF) represent a vulnerable population with high risks of cardiovascular and thromboembolic complications. This study aimed to comparatively analyze the frequency and characteristics of complications in CHF and AF patients with and without a history of COVID-19 infection. A total of 285 elderly patients (aged 60–74) were divided into two groups: Group 1 (n=145) included patients with CHF, AF, and previous COVID-19 infection, and Group 2 (n=140) included patients with CHF and AF without COVID-19. Retrospective data analysis was performed focusing on thromboembolic events, bleeding episodes, cardiac decompensation, arrhythmias, and infectious complications. The incidence of thromboembolic events such as pulmonary embolism (12.4% vs. 5%, p<0.01) and ischemic stroke (15% vs. 8%, p<0.05) was significantly higher in the COVID-19 group. Major and minor bleeding events were also more frequent in Group 1 (10% and 20% vs. 4.3% and 12.1%, respectively, p<0.05). Cardiac complications, including heart failure decompensation and ventricular tachyarrhythmias, occurred at higher rates in patients with prior COVID-19. Additionally, bacterial pneumonia incidence was elevated (7.6% vs. 1.4%, p<0.05). These findings underscore the exacerbating effect of COVID-19 on the severity and frequency of complications in CHF and AF patients, highlighting the need for tailored clinical management and anticoagulant dosing.
Keywords: Chronic heart failure, Atrial fibrillation, COVID-19, Thromboembolism, Bleeding, Cardiac decompensation, Arrhythmias, Pneumonia
Cite this paper: Begijon Adkhamjon ogli Avazbekov, Gavhar Mirakbarona Tulaboyeva, Khatam Khasanboyevich Tursunov, Comparative Study of Clinical Complications in Chronic Heart Failure and Atrial Fibrillation Patients, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2433-2437. doi: 10.5923/j.ajmms.20261605.39.
Article Outline
1. Introduction
- Chronic heart failure (CHF) and atrial fibrillation (AF) are two highly prevalent cardiovascular conditions that often coexist and contribute to significant morbidity and mortality worldwide. CHF results in impaired cardiac pumping function leading to inadequate systemic perfusion, while AF is characterized by irregular and often rapid heart rhythm causing an increased risk of thromboembolism. Both conditions independently and synergistically increase the risk of adverse events including stroke, hospitalization, and death [1,2].The emergence of COVID-19 has introduced new complexities to the management of cardiovascular diseases. Caused by SARS-CoV-2 virus, COVID-19 has a demonstrated impact on the cardiovascular system through direct viral injury, systemic inflammation, and endothelial dysfunction. Patients with pre-existing cardiovascular diseases, especially CHF and AF, face heightened vulnerability to severe COVID-19 complications. Recent evidence suggests that COVID-19 infection induces a hypercoagulable state, increasing the risk of thromboembolic events such as pulmonary embolism (PE) and ischemic stroke. Furthermore, COVID-19-related inflammation and hypoxia exacerbate cardiac dysfunction, leading to decompensation and arrhythmias [3,4,5].Despite these observations, there is limited comparative data quantifying the frequency and spectrum of complications in CHF and AF patients with and without COVID-19 infection. Understanding these differences is crucial to optimize clinical management and reduce morbidity and mortality in this vulnerable population. This study aims to analyze the incidence of thromboembolic, hemorrhagic, cardiac, and infectious complications in elderly patients with CHF and AF, comparing those with prior COVID-19 infection to those without, to inform future risk stratification and therapeutic strategies [6,7,8].
2. Materials and Methods
- This retrospective cohort study included 285 elderly patients aged 60 to 74 years diagnosed with chronic heart failure (CHF) and atrial fibrillation (AF) who were treated at the cardiology department of Andijan State Medical Institute, Uzbekistan. Patients were categorized into two groups based on their COVID-19 infection history: Group 1 (n=145) with documented prior COVID-19 infection and Group 2 (n=140) without such infection [9].Demographic data, clinical history, and laboratory findings were collected from medical records. The primary outcomes assessed included the frequency of thromboembolic events (pulmonary embolism and ischemic stroke), bleeding complications (major and minor), cardiac events (heart failure decompensation and ventricular tachyarrhythmias), and infectious complications (bacterial pneumonia) [10].Thromboembolic events were diagnosed based on clinical presentation supported by imaging studies such as Doppler ultrasonography, CT pulmonary angiography, and brain MRI. Bleeding events were classified according to standard criteria into major (requiring transfusion or intervention) and minor bleeding. Heart failure decompensation was diagnosed by worsening symptoms and signs requiring hospital admission or intensified therapy. Ventricular tachyarrhythmias were identified through ECG or telemetry monitoring. Bacterial pneumonia was confirmed by radiological findings and positive microbiological cultures [11,12].Statistical analysis was performed using SPSS software. Categorical variables were presented as frequencies and percentages. Comparisons between groups were made using chi-square tests or Fisher’s exact test as appropriate. A p-value of less than 0.05 was considered statistically significant. Confidence intervals were calculated for key complication frequencies to estimate the reliability of differences observed between groups.The study adhered to ethical standards and was approved by the institutional review board of Andijan State Medical Institute [13].The study included 285 elderly patients (aged 60 to 74 years) with CVE and BF. Of these, 138 (48.4%) were women and 147 (51.6%) were men. The study was conducted in the cardiology department of the Andijan State Medical Institute, Andijan region. Patients were divided into 2 groups according to the presence or absence of viral infection in their medical history: Group 1 (n=145): CVE, BF and COVID-19, Group 2 (n=140): CVE and BF, without COVID-19 infection. The study methods were as follows: retrospective analysis of data and medical history. Assessment of complications, i.e. analysis of thromboembolic events, bleeding, cardiac events and infectious complications [14].
3. Results and Discussion
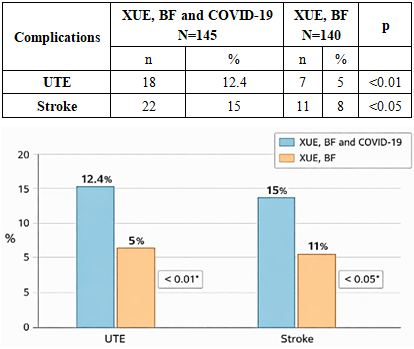
- The results showed that the incidence of thromboembolic events was significantly higher in patients with COVID-19. Pulmonary embolism (PE) was 12% in group 1 and 5% in group 2. At the same time, cerebral stroke was recorded in 15% of patients in group 1 and 8% in group 2.
|
|
|
4. Conclusions
- This study demonstrates that COVID-19 infection significantly increases the risk and severity of complications in patients with chronic heart failure and atrial fibrillation. Specifically, thromboembolic events such as pulmonary embolism and ischemic stroke occur at substantially higher rates in patients with prior COVID-19. These patients also face increased risks of both major and minor bleeding events, necessitating careful anticoagulant dose management.Moreover, cardiac complications including acute heart failure decompensation and ventricular tachyarrhythmias are more frequent in the COVID-19 group, reflecting the impact of systemic inflammation and hypoxia on cardiac function. The incidence of bacterial pneumonia is also elevated, likely due to COVID-19-induced immune suppression and lung damage.These findings highlight the need for personalized clinical strategies that balance thromboembolism prevention with bleeding risk mitigation, alongside proactive management of cardiac and infectious complications. Enhanced surveillance and tailored therapies will be crucial to improving prognosis in this high-risk group.
ACKNOWLEDGEMENTS
- The authors express their sincere gratitude to the staff of the Department of Cardiology and Gerontology of Andijan State Medical Institute for their continuous support and assistance in conducting this study. Special thanks are extended to the medical personnel of the cardiology department for their contribution to patient data collection and clinical monitoring.The authors also acknowledge the valuable assistance of the laboratory staff for their support in diagnostic procedures and data verification. Deep appreciation is given to colleagues who provided scientific guidance and constructive feedback throughout the research process.This study was supported by the internal research resources of Andijan State Medical Institute, and the authors are grateful for the institutional, technical, and infrastructural support provided.
Disclosure
- The authors declare that there are no conflicts of interest related to this study. This manuscript has not been previously published and is not currently under consideration for publication elsewhere. All authors have made substantial contributions to the conception, design, data collection, analysis, and interpretation of the study, and have approved the final version of the manuscript. No external funding was received specifically for this research. The study was conducted using the internal resources of Andijan State Medical Institute. No external editorial assistance, writing services, or paid review processes were utilized in the preparation of this manuscript. The findings presented in this study are based solely on the independent work of the authors.