-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2427-2432
doi:10.5923/j.ajmms.20261605.38
Received: Mar. 23, 2026; Accepted: Apr. 20, 2026; Published: May 18, 2026

Pathomorphological Changes in the Cardiovascular System in COVID-19 Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBostonov Sherzodbek Yakubjanovich, Mamajonov Ikboljon Maribjonovich
Andijan State Medical Institute, Uzbekistan
Correspondence to: Bostonov Sherzodbek Yakubjanovich, Andijan State Medical Institute, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study investigates pathomorphological changes in the cardiovascular system in patients with COVID-19 and post-COVID syndrome. The findings demonstrate significant structural and vascular alterations in the myocardium, largely resembling those observed in elderly patients with acute and chronic ischemic heart diseases. The most prominent changes include chronic cardiosclerosis, focal myocarditis, and endothelial dysfunction in the coronary vessels. In addition, pronounced atherosclerotic alterations were identified, characterized by plaque instability, structural destruction, and progression toward decompensation. These processes were frequently associated with enhanced thrombus formation, indicating a high thrombogenic potential in affected patients. The observed pathological changes suggest that SARS-CoV-2 infection contributes not only to acute myocardial injury but also to the progression of pre-existing cardiovascular conditions. Furthermore, the persistence of these alterations in the post-COVID period highlights the long-term impact of the disease on cardiac structure and function. Overall, the results emphasize the critical role of vascular and myocardial damage in the pathogenesis of COVID-19-related cardiovascular complications.
Keywords: COVID-19, SARS-CoV-2, ACE2 receptors, Myocardium, Coronary vessels, Cardiovascular system, Myocarditis, Post-COVID syndrome
Cite this paper: Bostonov Sherzodbek Yakubjanovich, Mamajonov Ikboljon Maribjonovich, Pathomorphological Changes in the Cardiovascular System in COVID-19 Disease, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2427-2432. doi: 10.5923/j.ajmms.20261605.38.
1. Introduction
- Coronavirus disease 2019 (COVID-19), caused by the SARS-CoV-2 virus, remains a major global health challenge due to its multisystem involvement and long-term consequences. Although primarily affecting the respiratory system, increasing evidence demonstrates significant involvement of the cardiovascular system, which substantially contributes to morbidity and mortality rates [1,2]. The virus gains entry into host cells via angiotensin-converting enzyme 2 (ACE2) receptors, which are highly expressed in cardiomyocytes and vascular endothelial cells, thereby facilitating direct myocardial and vascular injury [9,11].The pathogenesis of cardiovascular complications in COVID-19 is multifactorial and involves direct viral cytotoxic effects, endothelial dysfunction, dysregulation of the renin–angiotensin–aldosterone system, and an excessive inflammatory response known as a cytokine storm [3,4,12]. These mechanisms result in myocardial injury, ischemia, microvascular dysfunction, and activation of prothrombotic pathways, significantly increasing the risk of thromboembolic events [5,13].In addition, systemic hypoxia, metabolic imbalance, and increased sympathetic activity further aggravate myocardial damage and contribute to the development of cardiac arrhythmias and conduction disturbances [8]. Elevated levels of cardiac biomarkers, particularly troponins, are considered important indicators of myocardial injury and are associated with poor prognosis [2,14].Clinical and pathological studies indicate that COVID-19 patients frequently develop myocarditis, pericarditis, myocardial infarction, and pulmonary embolism, especially in severe forms of the disease [6,15]. Moreover, persistent cardiovascular complications have been observed in the post-COVID period, including left ventricular dysfunction, myocardial fibrosis, and chronic inflammatory changes, which may lead to long-term cardiac impairment [7,12].Thus, the study of pathomorphological changes in the cardiovascular system in COVID-19 remains highly relevant for understanding disease mechanisms, improving diagnostic accuracy, and optimizing therapeutic strategies.Purpose of the studyThe purpose of study the pathomorphological changes in the cardiovascular system during the periods of the COVID-19 disease and the post-covid syndrome.
2. Materials and Methods
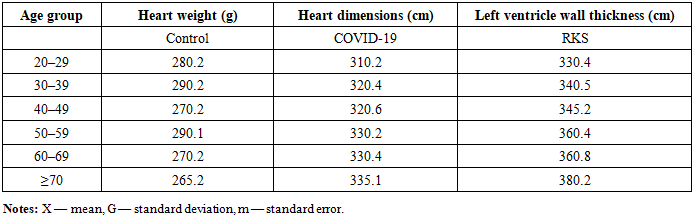
- This study included 60 patients who died from acute COVID-19 infection and post-COVID syndrome between 2020 and 2023, as well as 18 control subjects who died from non-COVID-related causes. The subjects were stratified by age into decade-based groups starting from 20 years. Autopsy data were obtained from the Department of Infectious Diseases of the Pathological Anatomy Center of the Ministry of Health of the Republic of Uzbekistan, as well as from hospitals in the Andijan region.During autopsy, the heart was examined macroscopically. Heart weight, anatomical structure, and morphometric parameters, including dimensions and left ventricular wall thickness, were measured. Particular attention was given to the assessment of atherosclerotic changes in the coronary arteries, as well as the presence of stenosis and thrombosis.For histological examination, myocardial tissue samples measuring approximately 1×1 cm were collected and fixed in 4% neutral buffered formalin. Tissue sections were obtained from the anterior and posterior walls of the left ventricle (2 cm above the apex), below the fibrous ring of the mitral valve, and from the interventricular septum. After dehydration in graded alcohol and chloroform, the samples were embedded in paraffin blocks.Paraffin sections with a thickness of 5–8 μm were prepared and stained with hematoxylin and eosin for microscopic evaluation.
3. Results
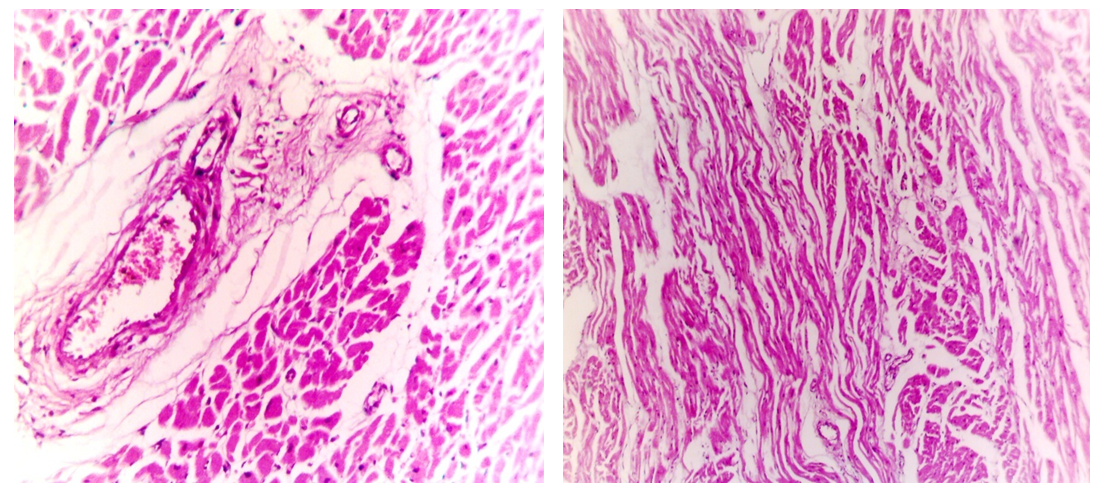
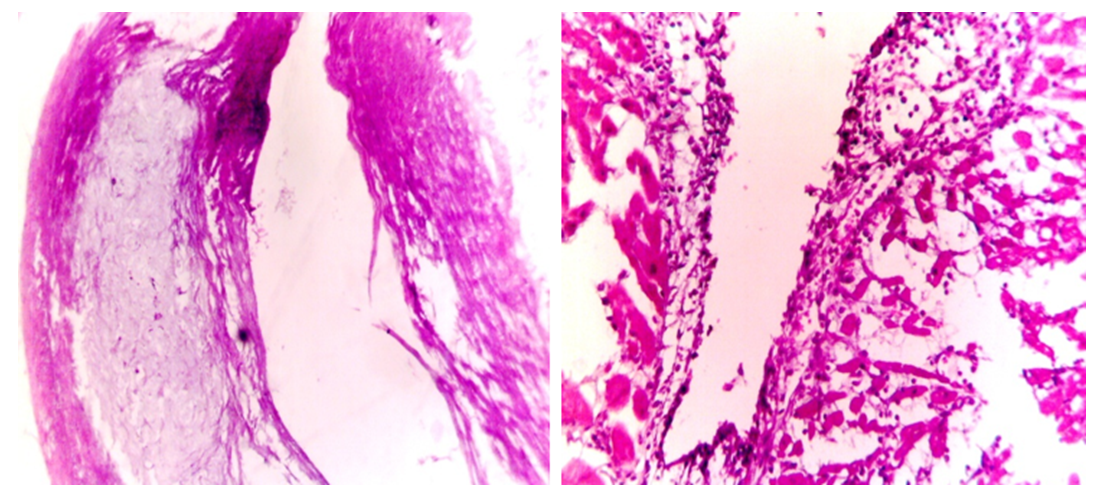
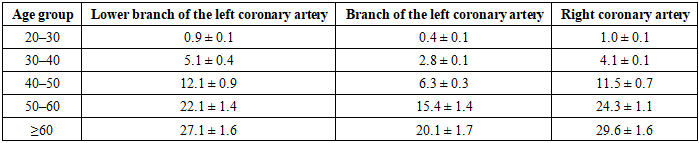
- Morphological examination of the myocardium in approximately one-third of autopsy cases of patients who died from COVID-19 revealed venous congestion and the presence of both small and large sclerotic foci. Microscopic analysis showed venous plethora, perivascular sclerosis, and signs of ischemia. Cardiomyocytes exhibited a hypercontractile state accompanied by structural alterations, including undulation, fuchsinophilia, and fragmentation (Fig. 1). Severe contracture injuries corresponding to grade III were predominantly observed in the ventricular myocardium. Notably, in all examined cases, blood within the cardiac cavities remained in a liquid state (Tables 1 and 2).
|
|
|
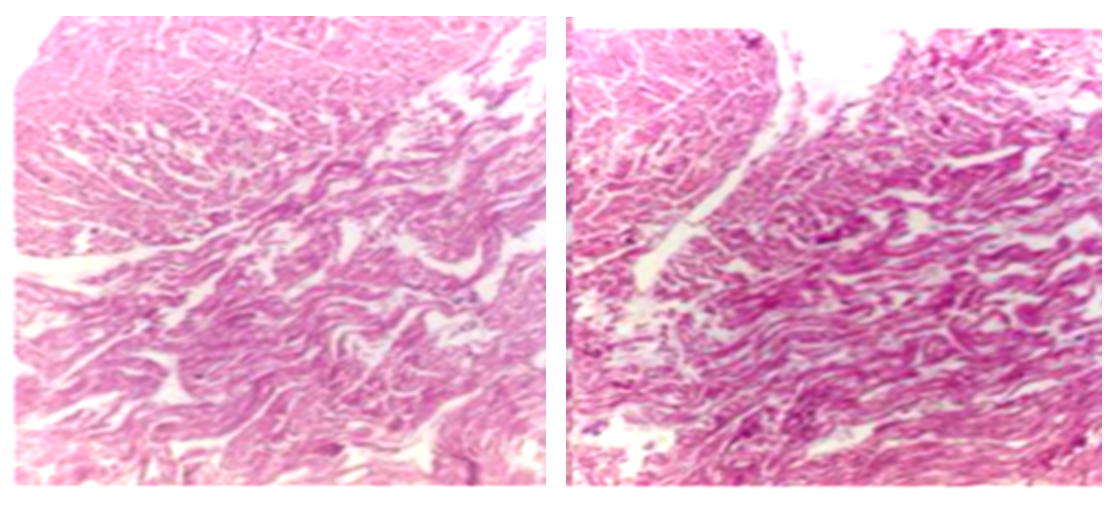 | Figure 1. Cardiomyositis contracture damage of the 2nd-3rd degree in the death of the COVID-19 disease. Stained by the hemm.-eosin method. 4x40 magnification |
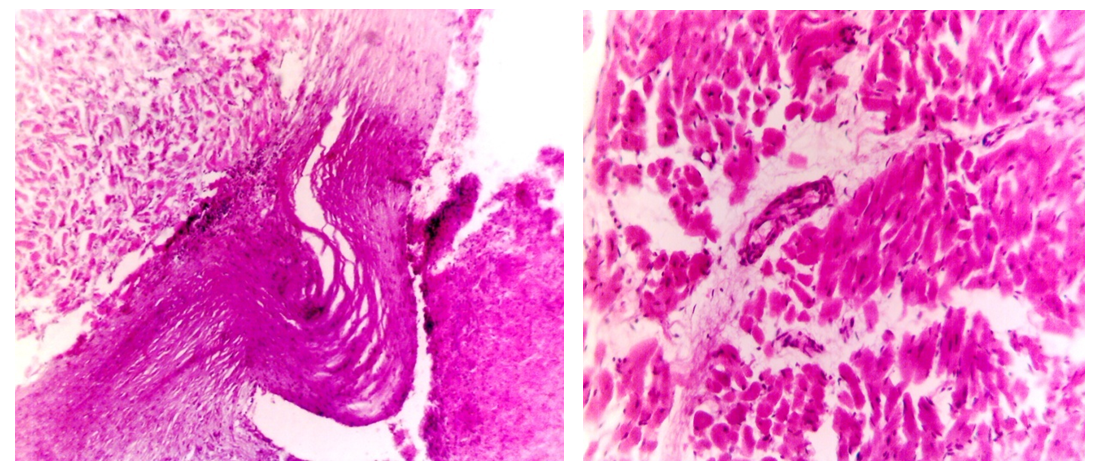
 | Figure 2. Patient F.F., born in 1995. 1-2. moderate fullness, perivascular sclerosis, swelling, interstitial tissue swelling, focal adipose tissue growth, small sclerosis, foci, undulating course of some groups of cardiomyositis, fragmentastia, a small amount of lymphoid infiltration in the interstitial tissue. Hemm.-eosin staining. Magnification 4*12.5 |
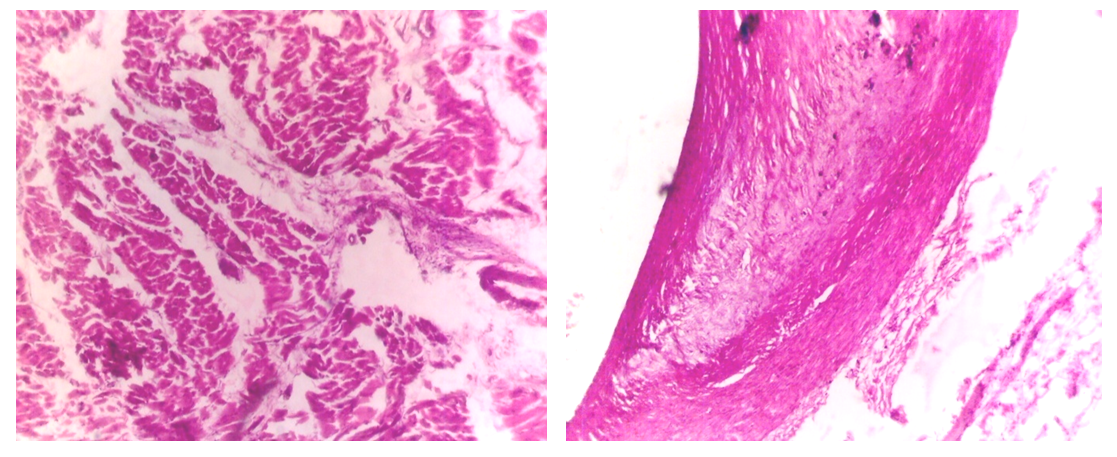
 | Figure 3. Patient I.X. 1988y.t. 1. Lipoidosis, liposclerosis, atheromatous changes in the intima and media layers of coronary vessels due to sharp narrowing and desquamation of the intima. 2. Patient B.I. 1990 moderate fullness, perivascular sclerosis, edema, small sclerosis foci in the myocardium, a small amount of lymphoid infiltration, the wave-like course of some groups of cardiomyocytes, fragmentation, and atrophic changes. Hemm.-eosin staining. Magnification 1. - 4*12.5. 2.10*12.5 |
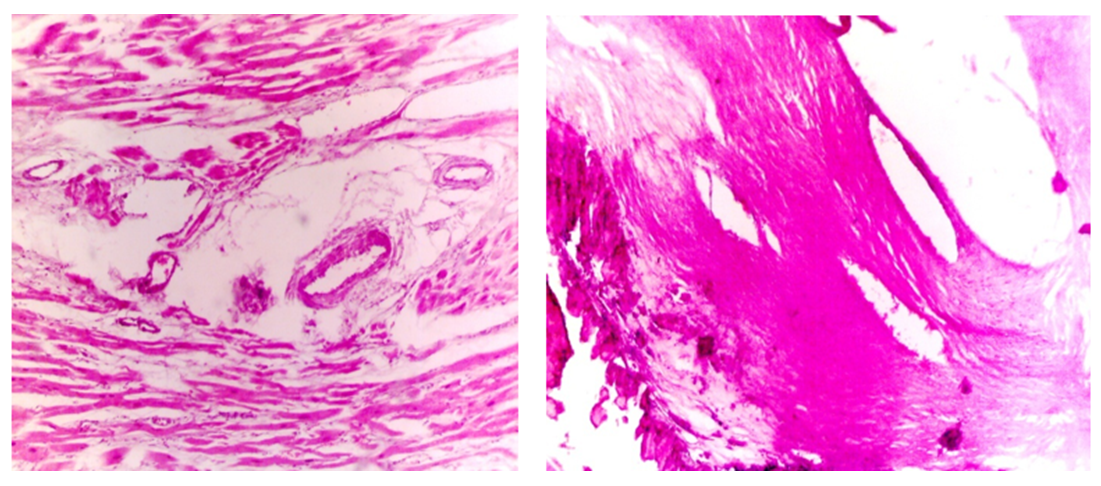
 | Figure 4. Patient U.S., born in 1982. 1. Perivascular sclerosis, edema of perivascular and interstitial tissue, small sclerosis foci, undulating course of certain groups of cardiomyocytes, fragmentation, necrobiotic changes, 2. lipidosis, lipo sclerosis, atheromatous in the intima and media layers of coronary vessels. Changes, wall thickening, and cavity narrowing to 1/3. Hemm.-eosin staining. Magnification 1. 4*12.5. 2.10*12.5 |
 | Figure 5. Patient G.K. 1969 1- moderate venous congestion, perivascular sclerosis, edema, interstitial tissue edema, small and large foci of sclerosis, undulating course of certain groups of cardiomyocytes, fragmentation, necrobiotic changes, foci growth of fatty tissue, desquamation of the intima of 2 coronary vessels, atheromatous changes in the intima and media, foci of calcification, destruction, a sharp narrowing of the cavity, decompensation, using the Hemm-eosin method live Magnification 4*12.5 |
 | Figure 6. Patient S.M. was born in 1960. 1. atheromatous changes in the coronary vessels, thickening of the intima and media layers, thickening of the wall, narrowing of the cavity to ½ part, destruction, 2. lymphoid infiltration in the intima, perivascular edema, sclerosis, edema in the surrounding myocardium, small sclerosis focus staining by Gemm.-eosin method—magnification 10*12.5 and 4*12.5 |
|
4. Conclusions
- Morphological and morphometric examination of the myocardium in patients with COVID-19 and post-COVID syndrome demonstrates that precise histopathological diagnosis can be challenging due to the heterogeneity of myocardial changes. The extent of myocardial damage varies depending on the patient’s age, disease severity, and duration of infection. Macroscopic and microscopic analyses consistently show an increase in morphometric parameters, including myocardial wall thickness, contractile dysfunction, and the presence of sclerosis foci. Concurrently, atherosclerotic changes in coronary vessels worsen progressively, with increased wall thickening, formation of fibrotic and lipid plaques, intimal and medial destruction, and thrombosis formation.The findings also highlight the importance of both cardiac and extracardiac triggering factors in the development of myocardial ischemia. Age-related progression is accompanied by an elevated incidence of acute coronary events, including myocardial infarction, accidental cardiac death, acute coronary syndrome, and post-infarction scarring. Focal and diffuse myocarditis, along with endothelial dysfunction in coronary vessels, contribute to impaired myocardial perfusion and contractile function. Decompensation of atherosclerotic lesions and increased thrombogenic activity further exacerbate cardiac injury.These observations underscore the multifactorial pathogenesis of COVID-19-related cardiac damage, in which viral effects, inflammatory responses, ischemic insults, and age-dependent structural changes interact to determine the severity and clinical outcomes of myocardial injury. Comprehensive morphometric assessment of both the myocardium and coronary vessels is therefore essential for understanding the cardiac complications associated with COVID-19 and for guiding post-infection clinical management.