-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2421-2426
doi:10.5923/j.ajmms.20261605.37
Received: Apr. 8, 2026; Accepted: May 5, 2026; Published: May 15, 2026

Pathogenetic Heterogeneity, Clinical Phenotypes, and Pharmacological Correction of Cerebral Microangiopathy: The Role of Inflammatory Mediators and Cognitive Profiles
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdambaev Z. I.1, Mirdjuraev E. M.2, Pazylova A. S.3
1Urgench State Medical Institute, Urgench, Uzbekistan
2Center for the Development of Professional Qualification of Medical Workers, Department of Neurorehabilitation, Tashkent, Uzbekistan
3International School of Medicine of the Educational-Scientific-Production Complex “International University of Kyrgyzstan”, Bishkek, Kyrgyzstan
Correspondence to: Adambaev Z. I., Urgench State Medical Institute, Urgench, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Relevance. Cerebral microangiopathy (CMA) is a heterogeneous group of diseases and a leading cause of vascular cognitive impairment. The relationship between etiology, inflammatory mediator profiles, specificity of cognitive deficits, and the efficacy of pharmacological correction remains insufficiently studied. Aim. To conduct a comprehensive comparative analysis of pro-inflammatory cytokines (IL-1β, TNF-α) and matrix metalloproteinase-9 (MMP-9) levels, the structure of cognitive impairments, and to evaluate the efficacy of the herbal preparation NeuroAiD II in various etiological forms of CMA. Materials and Methods. In the first part of the study (n=150), patients with hypertensive (n=30), amyloid (n=30), diabetic (n=30), inflammatory forms of CMA (n=30), and a control group (n=30) were examined. Laboratory assessment of mediators (ELISA, zymography) and neuropsychological testing (MoCA, MMSE, FAB) were performed. In the second part (n=65), the efficacy of NeuroAiD II in the correction of chronic cerebral ischemia was studied compared to basic therapy. Results. A specific “mediator portrait” of CMA forms was established: dominance of TNF-α in the hypertensive form, MMP-9 in cerebral amyloid angiopathy (CAA), IL-1β in diabetes, and pan-elevation of mediators in vasculitis. Unique cognitive phenotypes were identified: dysexecutive syndrome in hypertension, memory disorders in CAA, and diffuse decline in diabetes. The use of NeuroAiD II showed high efficiency in reducing anxiety, depression, asthenia, and improving cognitive functions (MMSE +2.4 points). Conclusion. A comprehensive assessment of biochemical markers and cognitive profiles allows for optimizing differential diagnosis and treatment strategies. The inclusion of neurometabolic and neuroprotective drugs (exemplified by NeuroAiD II) in the therapy regimen significantly improves clinical outcomes.
Keywords: Cerebral microangiopathy, Small vessel disease, IL-1β, TNF-α, MMP-9, Neuroinflammation, Cognitive impairment, Vascular dementia, NeuroAiD II, Chronic cerebral ischemia
Cite this paper: Adambaev Z. I., Mirdjuraev E. M., Pazylova A. S., Pathogenetic Heterogeneity, Clinical Phenotypes, and Pharmacological Correction of Cerebral Microangiopathy: The Role of Inflammatory Mediators and Cognitive Profiles, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2421-2426. doi: 10.5923/j.ajmms.20261605.37.
Article Outline
1. Introduction
- Cerebral microangiopathy (CMA), representing the morphological substrate of cerebral small vessel disease (CSVD), is today one of the most complex and urgent problems in modern neurology. According to epidemiological data, CMA serves as a leading cause of vascular cognitive impairment (VCI) and vascular dementia, ranking second in contribution to the global structure of dementias after Alzheimer's disease and placing a tremendous socioeconomic burden on healthcare systems worldwide [10,12]. Traditionally viewed as a single clinico-morphological entity, CMA is currently recognized as a heterogeneous group of diseases united by the common involvement of arterioles, capillaries, and venules in the deep regions of the brain, but differing in etiology, pathogenetic pathways, and, critically, therapeutic targets.The spectrum of etiological variants of CMA is broad and polymorphic. Key clinical forms include hypertensive angiopathy (arteriolosclerosis), cerebral amyloid angiopathy (CAA), diabetic microangiopathy, and primary/secondary inflammatory vasculitides [3,4,13,14]. Despite the final commonality of clinical outcome - progressive cognitive decline - each variant possesses a unique pathomorphological "portrait": from lipohyalinosis and fibrosis of the tunica media in hypertension to the deposition of β-amyloid in the membrane of muscle cells in CAA. This condition determines not only differences in neuroimaging patterns (localization of lacunar infarcts, nature of leukoaraiosis, type of microhemorrhages) but also forms fundamental differences in prognosis and patient management strategies.Modern scientific research has deeply penetrated the molecular mechanisms of CMA progression, convincingly demonstrating that pro-inflammatory cytokines (interleukin-1β [IL-1β], tumor necrosis factor-α [TNF-α]) and matrix metalloproteinases (MMP-9) play a key role in the damage cascade. These mediators are not merely markers but active drivers of the pathological process. IL-1β and TNF-α initiate and sustain chronic low-grade inflammation in the vessel wall and brain parenchyma, promoting endothelial dysfunction and apoptosis of glial cells. MMP-9, in turn, acts as a key effector of extracellular matrix destruction, leading to degradation of vascular basement membranes, disruption of blood-brain barrier (BBB) integrity, and remodeling of the vascular wall towards rigidity or ectasia [15,18]. The imbalance of this cytokine network explains the transition from compensated hemodynamic insufficiency to irreversible white matter degeneration.For a long time, clinical practice was dominated by a simplified view of cognitive deficit in microangiopathy as a unified phenomenon of "subcortical dementia," characterized by slowing of psychomotor processes (bradyphrenia) and executive function deficit with preserved memory. However, the accumulation of data from high-field MRI and refined neuropsychological verification has subjected this concept to revision. It has become evident that various etiological factors form specific clinical phenotypes: from "pure" dysexecutive syndrome in hypertensive encephalopathy to the dominance of mnestic disorders mimicking neurodegeneration in cerebral amyloid angiopathy, or diffuse reduction in neuroplasticity in diabetic encephalopathy [20]. This phenotypic variability dictates the necessity of abandoning averaged therapeutic approaches in favor of personalized medicine.Treatment of CMA, clinically manifesting as chronic cerebral ischemia (CCI), requires a comprehensive, multidisciplinary approach. Control of modifiable risk factors (arterial hypertension, hyperglycemia, dyslipidemia) is a necessary but insufficient condition for stabilizing the process. In light of the leading role of neuroinflammation and metabolic depression of neurons, pathogenetic neuroprotection becomes a strategic task. In recent years, scientific and clinical attention has shifted towards herbal preparations and complex dietary supplements with multimodal action. A key example is the preparation NeuroAiD II, which in a number of clinical studies has demonstrated not only symptomatic improvement but also potential for disease modification. Thanks to its unique composition, this preparation possesses synergistic neurotrophic, anti-apoptotic, and pro-angiogenic effects, stimulating neurogenesis and synaptogenesis, which makes it a promising tool in the correction of cognitive disorders and post-stroke rehabilitation [6,7,19]. Thus, the integration of modern concepts of the neuroimmunopathogenesis of CMA with the application of multimodal neurometabolic therapeutic strategies opens new horizons in the fight against vascular dementia.The aim of this comprehensive study was to perform a comparative evaluation of inflammatory mediator levels, analyze the structure of cognitive impairments in various etiological forms of CMA, and investigate the possibilities of pharmacological correction for the identified disorders.
2. Material and Research Methodology
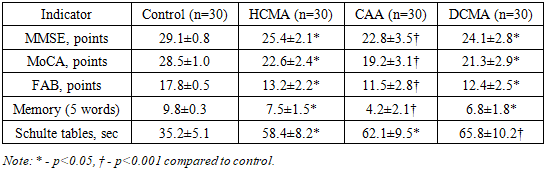
- The study design represents a comprehensive prospective project comprising two stages: a comparative cross-sectional clinical and laboratory study of etiological variants of cerebral microangiopathy (CMA) and an open comparative randomized clinical trial on the efficacy of pharmacological correction of chronic cerebral ischemia.The study was conducted in accordance with the standards of Good Clinical Practice (GCP) and the Declaration of Helsinki. The protocol was approved by the Local Ethics Committee. All participants signed informed consent for participation.Part I. Comparative Clinical and Laboratory Analysis of Etiological Forms of CMAThis part of the study included 151 patients. The main group consisted of 120 patients (58 men and 62 women, mean age 64.5±8.2 years) with a verified diagnosis of cerebral microangiopathy. The comparison group (control) consisted of 30 practically healthy volunteers, matched by sex and age, without signs of cerebral vascular pathology or cognitive complaints.Inclusion criteria for the main group:Presence of clinical and neuroimaging signs of cerebral small vessel damage according to modern criteria (STRIVE - Standards for Reporting Vascular Changes on Neuroimaging) [20].Patient age from 45 to 80 years.Verified etiology of CMA.Exclusion criteria:History of focal neurological deficit (stroke) with severe residual paresis (Rankin scale score >3).Signs of macrovascular pathology (hemodynamically significant stenosis of carotid arteries >50%).Diagnosed neurodegenerative dementia (Alzheimer's disease, Parkinson's disease, dementia with Lewy bodies).Severe depression or mental disorders preventing testing (Hamilton scale >17).History of oncological diseases, systemic infections in the acute phase.Formation of clinical groups (30 patients in each):Group HCMA (Hypertensive CMA): Patients with a long history of arterial hypertension (over 10 years). MRI criteria: presence of periventricular and deep leukoaraiosis (Fazekas scale ≥2), lacunar infarcts in subcortical nuclei and/or white matter, absence of lobar microhemorrhages [10,15,20].Group CAA (Cerebral Amyloid Angiopathy): Diagnosis was established based on modified Boston criteria. MRI criteria: presence of multiple lobar microhemorrhages (on SWI/T2* sequences), cortical superficial siderosis, possible atrophy of medial temporal lobes [5,14,20].Group DCMA (Diabetic CMA): Patients with type 1 or type 2 diabetes mellitus (history of at least 5 years). Criteria: presence of diabetic retinopathy and/or nephropathy, MRI data indicating diffuse white matter damage [3,20].Group ISVV (Inflammatory Small Vessel Vasculitis): Patients with systemic lupus erythematosus (SLE, meeting ACR/EULAR criteria) or primary CNS vasculitis, confirmed by MR angiography or CSF analysis [4].Methods of examination (Part I):Neuroimaging: All patients underwent brain MRI on a scanner with a magnetic field strength of at least 1.5 T. Protocols used: T1, T2, FLAIR, DWI, SWI/T2* (to assess hemorrhagic transformation) [17,20].Neuropsychological testing: Conducted by a qualified neuropsychologist in an isolated room. Scales used:MMSE (Mini-Mental State Examination) and MoCA (Montreal Cognitive Assessment) - for global assessment of cognitive functions [1,2,10].FAB (Frontal Assessment Battery) - for assessing executive functions (frontal lobes) [10,20].5-word test (Dubois) - for assessing episodic memory.Schulte tables - for assessing attention span and concentration, speed of psychomotor reactions [1,2].Laboratory assessment of biomarkers:Blood sampling was performed fasting from the cubital vein. Lumbar puncture for cerebrospinal fluid (CSF) collection was performed strictly according to indications when differential diagnosis was necessary (under local anesthesia).Levels of pro-inflammatory cytokines IL-1β and TNF-α were determined by solid-phase enzyme-linked immunosorbent assay (ELISA) using high-sensitivity test systems (sensitivity <0.1 pg/mL).The level of matrix metalloproteinase-9 (MMP-9) was determined by gelatin zymography followed by densitometry, which allowed assessing not only the concentration but also the enzymatic activity of the enzyme [17,18].Part II. Pharmacological Correction of Cognitive Impairments (Clinical Study)To evaluate therapeutic efficacy, 61 patients diagnosed with stage II–III chronic cerebral ischemia (CCI) (mean age 60.1±3.2 years) were examined [1,2,16].Design: An open comparative randomized study in two parallel groups. Randomization was performed using the envelope method (simple randomization).Group characteristics:Group 1 (Main, n=37): Received basic therapy and the preparation NeuroAiD II. Basic therapy included: antihypertensive drugs (ACE inhibitors/ARBs, calcium channel blockers if necessary), antiplatelet agents (acetylsalicylic acid 75–100 mg/day or clopidogrel), and for diabetes mellitus (DM) - glucose-lowering therapy. NeuroAiD II was prescribed at 400 mg (4 capsules) 3 times a day for a course of 60 days [6,7,19].Group 2 (Control, n=24): Received only basic therapy in a comparable volume [2,16].Efficacy assessment criteria:Assessment was conducted at the baseline visit (Visit 1), after 30 days (Visit 2), and after 60 days (Visit 3).Cognitive sphere: MMSE scale (Mini-Mental State Examination).Emotional sphere: Hospital Anxiety and Depression Scale HADS.Asthenic syndrome: Multidimensional Fatigue Inventory MFI-20.Statistical Data ProcessingStatistical analysis was performed using the IBM SPSS Statistics 26.0 package (USA).Testing for normal distribution of quantitative features was performed using the Shapiro-Wilk test.Data were described using the arithmetic mean (M) and standard deviation (SD) or median (Me) and interquartile range depending on the distribution type.Comparison of independent groups was performed using the Mann-Whitney test (for non-parametric data) or Student's t-test.To analyze the dynamics of indicators within groups, the Wilcoxon paired test or Student's t-test for dependent samples was used.Comparison of more than three groups was performed using analysis of variance (ANOVA) with Tukey's post-hoc test.To assess the relationship between laboratory parameters and cognitive scores, correlation analysis (Spearman's coefficient) was used.Differences were considered statistically significant at a significance level of p < 0.05.
3. Research Results
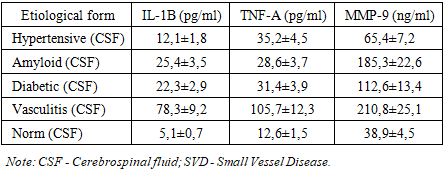
- The results of the conducted comprehensive study confirmed the fundamental hypothesis regarding the heterogeneity of cerebral microangiopathy (CMA). The obtained data demonstrate that, despite the similarity of the final clinical outcome in the form of cognitive deficit, various etiological variants of CMA possess unique biochemical profiles and neuropsychological phenotypes, which necessitates a differentiated approach to therapy [10,12].1. Pathogenetic aspects: the role of inflammatory mediators and proteolysisAnalysis of the concentrations of pro-inflammatory cytokines and matrix metalloproteinases in the cerebrospinal fluid (CSF) revealed clear differences between the groups, reflecting the specificity of the molecular mechanisms of brain damage (Table 1).In the hypertensive form (HCMA), the leading pathogenetic driver is chronic hemodynamic stress, leading to the activation of the renin-angiotensin-aldosterone system (RAAS) and endothelial dysfunction. In this group, a moderate increase in IL-1β (12.1±1.8 pg/mL) and a statistically significant increase in the level of TNF-α (35.2±4.5 pg/mL) compared to the norm were recorded. The high level of TNF-α confirms its central role in systemic inflammation: it induces the expression of adhesion molecules on endotheliocytes, promoting leukocyte infiltration of the vascular wall and disruption of microcirculation. A moderate increase in MMP-9 (65.4±7.2 ng/mL) is associated with vascular wall remodeling processes in response to elevated pressure, but does not reach critical values, explaining the relatively low risk of massive hemorrhages in this form [10,15].The mediator profile in cerebral amyloid angiopathy (CAA) is characterized by a unique specificity. A significant increase in IL-1β in the CSF (25.4±3.5 pg/mL) is observed, reflecting pronounced microglial activation in response to β-amyloid deposition in the vascular wall. The most indicative feature is a sharp jump in the level of MMP-9 to values of 185.3±22.6 ng/mL, which exceeds the norm by more than 4 times. It is known that β-amyloid has a direct inductive effect on MMP-9 expression in astrocytes and microglia. The high proteolytic activity of MMP-9 leads to the degradation of the basement membrane of vessels and white matter, which correlates with a high risk of lobar microhemorrhages and "amyloid flares" characteristic of this disease [5,14].In the diabetic form (DCMA), a significant increase in all studied mediators was revealed, but IL-1β dominates (22.3±2.9 pg/mL). The pathogenetic justification for this is the activation of receptors for advanced glycation end products (RAGE) under the influence of AGEs, which triggers a cascade of oxidative stress and the production of pro-inflammatory cytokines. Levels of TNF-α and MMP-9 are also significantly elevated (31.4±3.9 pg/mL and 112.6±13.4 ng/mL, respectively), indicating a combination of inflammatory and destructive processes in the vascular wall. The obtained data correlate with the severity of systemic vascular complications of diabetes (retinopathy, nephropathy), confirming the systemic nature of angiopathy [3].Inflammatory small vessel vasculitis (ISVV) is characterized by peak, extremely high values of all three markers: IL-1β (78.3±9.2 pg/mL), TNF-α (105.7±12.3 pg/mL), MMP-9 (210.8±25.1 ng/mL). These data reflect the intensity of the primary autoimmune process with destruction of the vascular wall, leukocyte infiltration, and the development of a “cytokine storm”. Such an aggressive mediator environment explains the severity of the clinical picture and the high risk of developing extensive infarctions and hemorrhages in this pathology [4].
|
|
4. Discussion
- The results of the conducted comprehensive study convincingly demonstrate the profound pathogenetic and clinical heterogeneity of cerebral microangiopathy (CMA), refuting outdated concepts of it as a monolithic clinical phenomenon reducible exclusively to "subcortical dementia." It has been established that various etiological factors form unique pathophysiological cascades requiring differentiated diagnostic and therapeutic approaches.Biomarker risk stratification. The identification of specific "mediator profiles" in cerebrospinal fluid and blood serum has high value for etiopathogenetic diagnosis [17,18]. The dominance of TNF-α in the hypertensive form confirms the leading role of systemic endothelial inflammation and RAAS activation. A pathognomonic marker of cerebral amyloid angiopathy (CAA) is an extreme increase in MMP-9, correlating with the risk of lobar microhemorrhages and hemorrhagic transformation, which is critically important for choosing an antithrombotic strategy [5,14]. The predominance of IL-1β in the diabetic form reflects protein glycation and metabolic stress, while pan-cytokinemia in vasculitis serves as an indicator of autoimmune process activity [4]. Thus, determining the spectrum of mediators allows not only to differentiate forms of CMA in complex diagnostic cases but also to stratify the risk of adverse cerebrovascular events.Clinical and neuropsychological endophenotypes. The study revealed clear cognitive endophenotypes linked to the topography of the lesion. The hypertensive form is characterized by the classic dysexecutive syndrome (disconnection syndrome) with preserved memory. CAA mimics a neurodegenerative process with a dominant memory deficit and rapid progression, requiring management tactics different from those for vascular dementia. The diabetic form manifests with a diffuse decline in neurodynamic indicators, while inflammatory vasculitides demonstrate polymorphism of deficit depending on the localization of foci. Recognizing these phenotypes is necessary for targeted neurorehabilitation [20].Therapeutic prospects. In the context of pharmacological correction of chronic cerebral ischemia, the high efficacy of the multimodal herbal preparation NeuroAiD II has been proven. Its inclusion in complex therapy ensures significant regression of cognitive disorders (increase in MMSE score), relief of anxiety-depressive disorders, and reduction of asthenia severity. The mechanism of action of the drug, combining neuroprotection, stimulation of neurogenesis, and angiogenesis, allows influencing key links in the pathogenesis of ischemia, compensating for the neuroplasticity deficit [1,2,6,7,19].
5. Conclusions
- In conclusion, it should be emphasized that the obtained data fundamentally change the paradigm of managing patients with CMA. The transition from averaged therapeutic schemes to a personalized approach, based on etiopathogenetic diagnosis with the assessment of mediator profiles and cognitive phenotypes, is a mandatory condition for improving the quality of medical care. Further studies should be aimed at integrating biochemical markers into routine clinical practice and developing combination treatment regimens including drugs with proven neuroplastic and anti-inflammatory potential [15,18].
ACKNOWLEDGEMENTS
- The authors express their sincere gratitude to the staff of the departments and clinical bases of the Center for Professional Development of Medical Workers under the Ministry of Health of the Republic of Uzbekistan (Tashkent), Urgench State Medical Institute (Urgench), and I.K. Akhunbaev Kyrgyz State Medical Academy (Bishkek) for their organizational support and for providing the clinical base for the study.Special appreciation is extended to the staff of the laboratory services and radiology departments for their high professionalism in performing enzyme immunoassays, zymography, and neuroimaging studies (MRI).The authors also thank all patients who participated in the study for their voluntary informed consent and cooperation.