Kurbaniyazova Feruza Zafarjonovna
Samarkand State Medical University, Samarkand, Republic of Uzbekistan
Correspondence to: Kurbaniyazova Feruza Zafarjonovna, Samarkand State Medical University, Samarkand, Republic of Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Background: Thin endometrium (endometrial thickness < 7 mm at the implantation window) is a critical impediment to successful implantation, accounting for a substantial proportion of assisted reproductive technology failures. Standard hormonal stimulation frequently yields inadequate endometrial response, and evidence-based adjunctive strategies remain limited, particularly in Central Asian reproductive medicine contexts. Objectives: To evaluate the efficacy of an optimized pre-conception preparation protocol incorporating intrauterine autologous platelet-rich plasma (PRP) infusion and BTL-4000 magnetotherapy, compared with standard hormonal therapy alone, on endometrial thickness, uterine hemodynamics, vaginal microbiota normalization, resolution of chronic endometritis, and clinical pregnancy rate in women with thin endometrium. Methods: A prospective, single-center, open-label randomized controlled trial was conducted at the Gynecology Department of the Multidisciplinary Clinic of Samarkand State Medical University between January 2023 and December 2025. A total of 115 women aged 24–40 years were enrolled: Group 1 (intervention, n = 45) received the optimized protocol comprising hysteroscopy with polypectomy where indicated, targeted antimicrobial/antifungal therapy guided by Femoflor-16 PCR vaginal microbiota analysis, oral estradiol (2 mg/day for 21 days) with progesterone support, BTL-4000 magnetotherapy (Program M-0091; 5 sessions, 25 minutes each), and two intrauterine instillations of autologous PRP (2.5–3.0 mL on days 11–12 and 13–14 of the menstrual cycle); Group 2 (comparator, n = 30) received standard hormonal therapy with estradiol and progesterone only; and a Reference Group (healthy fertile women of reproductive age, n = 40) provided normative baseline values for inflammatory markers, microbiota profiles, and Doppler parameters. Primary outcomes were endometrial thickness at day 14, rates of achieving ≥ 8 mm thickness, resolution of chronic endometritis, and clinical pregnancy rate at 6 months. Results: Group 1 achieved a significantly greater mean endometrial thickness at day 14 compared to Group 2 (11.1 mm vs. 7.1 mm; p < 0.001), with 78% versus 42% of patients reaching the ≥ 8 mm threshold (p < 0.001). Chronic endometritis resolved in 85% of Group 1 vs. 60% of Group 2 (p = 0.008). Clinical pregnancy rate was 55% in Group 1 versus 30% in Group 2 (p = 0.01). Baseline IL-6 was markedly elevated in both treatment groups compared to the reference group (21.7 ± 2.4 vs. 9.4 ± 1.5 pg/mL; p < 0.05). Bacterial vaginosis was identified in approximately 50% of both treatment groups versus 0% in the reference group (p < 0.001). Significant improvements in uterine artery Doppler indices (PI, RI, S/D) were observed in Group 1 following treatment (all p < 0.001). Conclusions: The optimized pre-conception protocol combining PRP and magnetotherapy with hormonal therapy significantly outperformed hormonal therapy alone across all primary reproductive outcomes. These findings support the integration of PRP and magnetotherapy into standard pre-conception algorithms for women with thin endometrium, particularly those with concurrent chronic endometritis and dysbiosis. Study Novelty: This is the first randomized controlled trial to simultaneously evaluate the combined effect of intrauterine PRP, BTL-4000 magnetotherapy, and microbiota-guided antimicrobial therapy in a unified pre-conception protocol for thin endometrium, and the first to demonstrate a significant correlation between vaginal dysbiosis severity and IL-6 levels in this population within a Central Asian reproductive medicine setting.
Keywords:
Endometrium, Platelet-rich plasma, Infertility, Female, Endometritis, Uterus, Reproductive techniques, Assisted, Ultrasonography, Doppler
Cite this paper: Kurbaniyazova Feruza Zafarjonovna, Optimized Pre-Conception Preparation in Women with Thin Endometrium Using Platelet-Rich Plasma and Magnetotherapy: A Randomized Controlled Trial, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2414-2420. doi: 10.5923/j.ajmms.20261605.36.
1. Introduction
Infertility affects approximately 10–15% of couples of reproductive age worldwide and constitutes one of the most clinically and socially significant challenges in contemporary gynecology. [1,5] The uterine factor accounts for 24–62% of female infertility cases, with impaired implantation representing the most consequential and frequently insurmountable obstacle in reproductive medicine. [2,5] Among the structural causes of implantation failure, thin endometrium - broadly defined as an endometrial thickness below 7 mm at the expected implantation window - occupies a position of particular clinical importance, as it is associated with markedly reduced implantation, clinical pregnancy, and live birth rates in both natural cycles and assisted reproductive technology (ART) programs. [3,6,8]The pathogenesis of thin endometrium is multifactorial, encompassing microcirculatory insufficiency, chronic endometritis, hormonal dysregulation, adhesion formation, prior intrauterine instrumentation, and vaginal microbiome disruption. [1,4] Uterine microangiopathy reduces endometrial perfusion and impairs the proliferative and secretory responses necessary for receptivity. [7,9] Chronic endometritis, present in up to 60% of women with repeated implantation failure, sustains low-grade inflammatory cytokine upregulation - including interleukin-6 - that disrupts normal endometrial cycling and impairs embryo-endometrium cross-talk. [2,8] Vaginal dysbiosis, independently associated with impaired reproductive outcomes, creates an inflammatory milieu that may extend to the uterine cavity through ascending infection pathways. [4]A range of adjunctive interventions have been proposed to improve endometrial thickness and receptivity in ART settings, including endometrial scratching, human chorionic gonadotropin priming, granulocyte colony-stimulating factor infusion, autologous platelet-rich plasma (PRP), and stem cell therapy. [3,6] Platelet-rich plasma contains high concentrations of growth factors - including platelet-derived growth factor, vascular endothelial growth factor, transforming growth factor-beta, and insulin-like growth factor-1 - that promote endometrial proliferation, angiogenesis, and tissue regeneration. [6,8] Magnetotherapy with low-frequency pulsed magnetic fields has been shown to improve tissue microcirculation, reduce inflammatory activity, and enhance cellular regenerative processes, suggesting a mechanistic rationale for its application in thin endometrium. [7,9] However, no published randomized controlled trial has evaluated a protocol combining PRP, magnetotherapy, and microbiota-guided therapy in a single pre-conception preparation algorithm. [3]The present study was aimed at evaluating the efficacy of an optimized pre-conception protocol incorporating intrauterine autologous PRP infusion and BTL-4000 magnetotherapy, compared with standard hormonal therapy alone, on endometrial growth, uterine hemodynamics, microbiota normalization, chronic endometritis resolution, and clinical pregnancy rate in women with thin endometrium.
2. Materials and Methods
Study Design and ParticipantsA prospective, single-center, open-label randomized controlled trial was conducted at the Gynecology Department of the Multidisciplinary Clinic of Samarkand State Medical University between January 2023 and December 2025. A total of 115 women aged 24–40 years were enrolled and allocated to three groups. Group 1 (intervention: PRP + magnetotherapy + standard therapy, n = 45) and Group 2 (comparator: standard hormonal therapy alone, n = 30) both comprised women with confirmed thin endometrium (M-echo < 7 mm at the mid-luteal phase). The Reference Group (n = 40) consisted of healthy fertile women of reproductive age who provided normative baseline values for inflammatory markers, vaginal microbiota profiles, and Doppler hemodynamic parameters; this group did not receive any study intervention. Mean participant age was 27.6 ± 1.6 years (range 18–35 years). Randomization of Groups 1 and 2 was performed using a computer-generated allocation sequence; the two thin endometrium groups were confirmed comparable at baseline. The study was conducted within institutional research plan No. 01980006703.Inclusion criteria: confirmed thin endometrium (M-echo < 7 mm); age 18–40 years; primary or secondary infertility; absence of normal hormonal ovarian reserve; written informed consent. Exclusion criteria: other uterine anomalies (adhesions, fibroids distorting the cavity); endometriosis Stage III–IV; autoimmune disorders; prior endometrial ablation or pelvic irradiation; breastfeeding; polycystic ovary syndrome; premature ovarian insufficiency; contraindications to physical therapy; hemoglobin < 100 g/L; platelet count < 150 × 10⁹/L.Data Collection InstrumentsUltrasound and Doppler AssessmentAll patients underwent serial transvaginal ultrasound assessment in the mid-luteal phase (implantation window, cycle days 20–22) at baseline and after each treatment course. Endometrial thickness was measured as the maximal antero-posterior M-echo diameter. Uterine vascular Doppler examination was performed using color Doppler mapping (CDM with SMI mode) and spectral Doppler velocimetry, assessing pulsatility index (PI), resistance index (RI), and systole-to-diastole ratio (S/D) bilaterally in uterine, arcuate, radial, basal, and spiral arteries. Doppler measurements were performed blinded to group allocation by a certified ultrasound specialist.HysteroscopyHysteroscopy was performed under intravenous anesthesia using a rigid 7 mm Karl Storz hysteroscope (Karl Storz GmbH, Tuttlingen, Germany) at INNOVA EXPERT and Doctor D&U private medical centers. Endometrial polypectomy was performed hysteroscopically where indicated (Group 1: 13 patients [28.9%]; Group 2: 8 patients [26.7%]).Vaginal Microbiota AnalysisVaginal microbiota was characterized using the Femoflor-16 PCR test system (Androflor, Russia), which quantitatively profiles 16 microorganism groups. The analysis differentiated normobiosis, non-specific vulvovaginitis, vulvovaginal candidiasis, and bacterial vaginosis. Microbiota-guided antimicrobial therapy was prescribed based on individual results.Interleukin-6 MeasurementSerum interleukin-6 (IL-6) concentrations were determined by solid-phase ELISA using the Vector-Best reagent kit (JSC Vector-Best, Novosibirsk, Russia). IL-6 was measured at baseline in all three groups to characterize the inflammatory substrate of thin endometrium relative to healthy fertile women in the reference group.ProceduresOptimized Protocol (Group 1)The optimized pre-conception preparation protocol comprised two sequential treatment courses. The pharmacological component consisted of oral estradiol 2 mg/day from Day 1 to Day 21, followed by progesterone 200 mg/day for 10 days. Microbiota-guided antimicrobial treatment was administered prior to hormonal therapy: doxycycline 100 mg twice daily for 7 days (non-specific vulvovaginitis), clotrimazole 100 mg vaginal suppositories twice daily for 7 days (vulvovaginal candidiasis), or metronidazole 500 mg once daily for 7 days (bacterial vaginosis), followed by probiotic therapy. BTL-4000 magnetotherapy (Program M-0091; BTL Industries Ltd., Prague, Czech Republic) was administered on Days 6–10 of the menstrual cycle (5 sessions × 25 minutes each). Autologous PRP (3 mL) was instilled intrauterine transcervically under ultrasound guidance on Days 11–12 and 13–14 of the menstrual cycle in both treatment courses.Standard Protocol (Group 2)Group 2 received standard hormonal therapy: oral estradiol 2 mg/day for 21 days followed by progesterone 200 mg/day for 10 days, administered over two treatment cycles. No PRP, magnetotherapy, or microbiota-guided therapy was prescribed.Outcome AssessmentEndometrial thickness was assessed at Day 14 of the hormonal phase. Resolution of chronic endometritis was evaluated in the mid-luteal phase (Days 21–23) of the subsequent cycle. Clinical pregnancy was defined as intrauterine pregnancy with fetal cardiac activity confirmed on transvaginal ultrasound at 6–8 gestational weeks, tracked over a 6-month follow-up period.Ethical ConsiderationsThe study was approved by the Ethics Committee of Samarkand State Medical University (Ethics Approval No. 09/2022, issued 20 December 2022). The study was conducted in compliance with the Declaration of Helsinki. Written voluntary informed consent was obtained from all participants prior to enrollment. All data were anonymized prior to analysis.Statistical AnalysisStatistical analysis was performed using IBM SPSS Statistics version 25.0. Continuous data are reported as mean ± standard error of the mean (M ± m). Between-group comparisons used the Student t-test for normally distributed data and the Wilcoxon signed-rank test for paired pre–post comparisons. Categorical variables were compared using the Pearson chi-square test. Pearson correlation coefficients were used for correlation analyses. Odds ratio (OR) and relative risk (RR) were calculated where applicable. Statistical significance was set at p < 0.05 (two-tailed).
3. Results
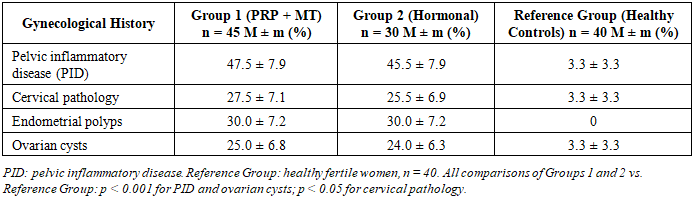
Baseline Demographic and Gynecological CharacteristicsThe most significant risk factors for thin endometrium identified in the cohort were lipid metabolism disorders (44.4%), thyroid disease (26.7%), late menarche (Groups 1 and 2: 24.4% and 26.6% respectively vs. 2.5% in the reference group; p < 0.001), pelvic inflammatory disease, and prior ovarian cysts. Hypomenstrual syndrome was significantly more prevalent in Groups 1 and 2 (66.7 ± 7.0% and 65.0 ± 7.5% respectively) compared to the reference group (2.5 ± 2.5%; p < 0.001). Secondary infertility was the predominant type (60.0% in Group 1; 63.5% in Group 2). Gynecological history data are presented in Table 1.Table 1. Gynecological history in study groups (%, M ± m)
 |
| |
|
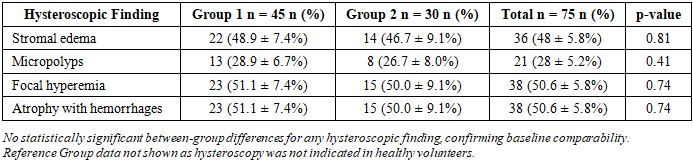
Baseline Endometrial ThicknessAt enrollment, endometrial thickness in the mid-luteal phase was below 7 mm in all patients with thin endometrium. Mean M-echo was 5.9 ± 1.2 mm in Group 1, 5.3 ± 1.5 mm in Group 2, and 9.4 ± 1.4 mm in the reference group. Visualization frequency of basal arteries was 23.4% lower in Group 1 compared to the reference group (p = 0.03) and 15.8% lower in Group 2 (p = 0.07), indicating baseline microcirculatory insufficiency in both treatment groups.Hysteroscopic FindingsHysteroscopy was performed in 75 patients (Groups 1 and 2 combined) and confirmed characteristic features of chronic endometritis and thin endometrium (Table 2). Hysteroscopic findings were similar between the two groups, confirming adequate baseline comparability.Table 2. Hysteroscopic findings at baseline (n = 75)
 |
| |
|
Interleukin-6 and Inflammatory SubstrateBaseline serum IL-6 was markedly elevated in both treatment groups compared to the reference group (Table 3). Mean IL-6 in Group 1 was 21.7 ± 2.4 pg/mL and in Group 2 was 20.0 ± 6.6 pg/mL, compared to 9.4 ± 1.5 pg/mL in the reference group - a more than two-fold elevation (p < 0.05). This elevated inflammatory state is consistent with the high prevalence of chronic endometritis and vaginal dysbiosis in both treatment groups.Table 3. Serum interleukin-6 levels at baseline (M ± m, pg/mL)
 |
| |
|
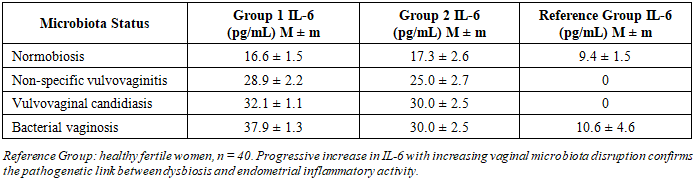
Vaginal Microbiota ProfileFemoflor-16 PCR analysis revealed that normobiosis was present in 93.3 ± 4.6% of the reference group but in only 32.5 ± 7.4% of Group 1 and 33.3 ± 5.6% of Group 2 patients (p < 0.001). Bacterial vaginosis was identified in approximately half of both treatment groups (Group 1: 52.5 ± 7.9%; Group 2: 50.5 ± 6.3%) compared to 0% in the reference group (p < 0.001). Table 4 demonstrates a progressive increase in IL-6 with increasing severity of microbiota disruption - from 16.6 ± 1.5 pg/mL in normobiosis to 37.9 ± 1.3 pg/mL in bacterial vaginosis in Group 1 - confirming the pathogenetic link between dysbiosis and endometrial inflammatory activity.Table 4. Serum IL-6 levels by vaginal microbiota status (M ± m, pg/mL)
 |
| |
|
Endometrial Thickness DynamicsThe serial endometrial thickness measurements following treatment are presented for Group 2 (Table 5) and Group 1 (Table 6). In Group 2, mean endometrial thickness increased from 4.25 mm at baseline to a plateau of 9.0–9.05 mm by Days 11–14. In Group 1, thickness increased from 4.35 mm at baseline to 9.5 mm by Day 11 and reached 11.1 mm by Day 14. The mean endometrial thickness at Day 14 was significantly greater in Group 1 (11.1 mm) compared to Group 2 (7.1 mm; p < 0.001). The proportion of patients achieving the ≥ 8 mm threshold was 78% in Group 1 versus 42% in Group 2 (p < 0.001).Table 5. Endometrial thickness dynamics in Group 2 (Hormonal therapy, n = 30)
 |
| |
|
Table 6. Endometrial thickness dynamics in Group 1 (PRP + Magnetotherapy, n = 45)
 |
| |
|
Uterine Artery Doppler ParametersAll patients with thin endometrium exhibited significantly reduced uterine artery blood flow velocities at baseline compared to normative values. Following treatment, significant improvements in Doppler parameters were observed in Group 1 in the right uterine artery (Table 7): PI (2.17 → 1.95; p < 0.01), RI (0.79 → 0.74; p < 0.001), and S/D (5.7 → 4.6; p < 0.001). Group 2 showed significant improvement only in PI and RI, with no significant change in S/D.Table 7. Doppler velocimetry parameters of the right uterine artery before and after treatment (M ± SD)
 |
| |
|
In the left uterine artery (Table 8), Group 1 demonstrated significant improvement in all three Doppler indices (PI: 2.13 → 1.90; RI: 0.80 → 0.76; S/D: 5.3 → 4.4; all p < 0.001). In Group 2, only PI reached statistical significance, while RI and S/D showed no significant change. The between-group difference in S/D reduction in the right uterine artery was statistically significant (p < 0.05), indicating superior hemodynamic response in the optimized protocol group. Correlation analysis confirmed a significant inverse relationship between endometrial M-echo thickness and spiral artery Doppler indices: PI (r = −0.50), RI (r = −0.52), and S/D (r = −0.53) (all p < 0.05).Table 8. Doppler velocimetry parameters of the left uterine artery before and after treatment (M ± SD)
 |
| |
|
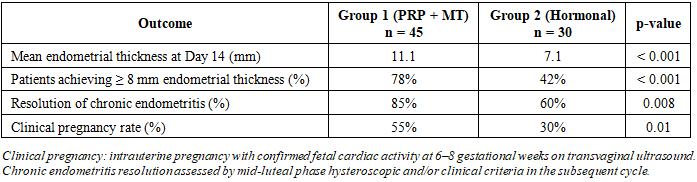
Reproductive OutcomesThe composite reproductive outcomes over a 6-month follow-up period are summarized in Table 9. The optimized protocol produced significantly superior outcomes across all measured endpoints. Clinical pregnancy rate in Group 1 was 55%, compared to 30% in Group 2 (p = 0.01). Resolution of chronic endometritis was achieved in 85% of Group 1 patients vs. 60% of Group 2 (p = 0.008).Table 9. Summary of primary reproductive outcomes at 6-month follow-up
 |
| |
|
4. Discussion
The present study was aimed at evaluating the efficacy of an optimized pre-conception preparation protocol combining intrauterine PRP, BTL-4000 magnetotherapy, and microbiota-guided antimicrobial therapy compared with standard hormonal therapy alone in women with thin endometrium. The most clinically significant finding was the substantially superior endometrial response in the intervention group - mean thickness 11.1 mm versus 7.1 mm (p < 0.001), with 78% versus 42% of patients achieving the ≥ 8 mm threshold - accompanied by a 25 percentage-point advantage in clinical pregnancy rate (55% vs. 30%; p = 0.01). These results provide level II evidence for the efficacy of this combined regenerative and physical therapy approach in a patient population where standard hormonal treatment frequently yields inadequate endometrial response.The role of PRP in endometrial growth stimulation has been investigated in several recent studies. Eftekhar et al. demonstrated that intrauterine PRP infusion in women with thin refractory endometrium produced a significant increase in endometrial thickness and clinical pregnancy rate compared to saline infusion control, [6] consistent with the endometrial proliferative effect observed in our intervention group. The mechanism involves growth factor-mediated stimulation of endometrial glandular and stromal proliferation, enhanced angiogenesis through vascular endothelial growth factor and platelet-derived growth factor release, and modulation of local immune responses that may reduce chronic endometrial inflammation. [6,8] The significant reduction in uterine artery Doppler resistance indices observed exclusively in Group 1 patients (all p < 0.001) supports the hypothesis that magnetotherapy exerts an independent vasodilatory and microcirculatory benefit, complementing the angiogenic effects of PRP. This aligns with established biophysical evidence for pulsed magnetic field-induced improvement in tissue perfusion, which may operate through nitric oxide-mediated vasodilation and anti-inflammatory cytokine modulation. [7,9]The finding that bacterial vaginosis was present in approximately 50% of patients in both treatment groups, and that IL-6 progressively increased from normobiosis (16.6 pg/mL) to bacterial vaginosis (37.9 pg/mL) - a finding derived by comparison with the reference group - provides direct evidence for a pathogenetically significant link between vaginal dysbiosis and endometrial inflammatory activity in thin endometrium. [4] The chronic endometritis resolution rate of 85% in Group 1 versus 60% in Group 2 (p = 0.008) further supports the contribution of targeted antimicrobial therapy and PRP's immunomodulatory properties to resolution of this condition. [2,8]This study has several limitations. First, the open-label design introduces potential performance bias. Second, the imbalanced group sizes (n = 45 vs. n = 30) reflect unequal allocation driven by treatment acceptability. Third, the 6-month follow-up captures clinical pregnancy rates but does not extend to live birth outcomes. Fourth, the single-center design limits generalizability. Strengths include the randomized controlled design, comprehensive multi-domain outcome assessment, the use of validated Femoflor-16 PCR microbiota analysis, and the statistical rigor of the correlation analyses.
5. Conclusions
The optimized pre-conception preparation protocol combining intrauterine autologous PRP, BTL-4000 magnetotherapy, and Femoflor-16-guided antimicrobial therapy produced significantly superior outcomes in women with thin endometrium compared to standard hormonal therapy alone: mean endometrial thickness 11.1 mm vs. 7.1 mm (p < 0.001); 78% vs. 42% of patients reaching ≥ 8 mm threshold (p < 0.001); chronic endometritis resolution 85% vs. 60% (p = 0.008); and clinical pregnancy rate 55% vs. 30% (p = 0.01). Significant improvements in all uterine artery Doppler resistance parameters were observed exclusively in the intervention group (all p < 0.001). Vaginal dysbiosis, present in approximately 50% of patients with thin endometrium, was quantitatively associated with progressive elevation of IL-6, supporting its inclusion as a mandatory screening component in pre-conception evaluation.From a health policy perspective, these findings support the revision of national pre-conception protocols to incorporate: (1) mandatory Femoflor-16 PCR vaginal microbiota profiling for all women with thin endometrium prior to ART enrollment; (2) structured microbiota-guided antimicrobial therapy before hormonal stimulation; and (3) adjunctive intrauterine PRP and magnetotherapy in women failing to achieve adequate endometrial thickness with hormonal therapy alone.The following recommendations are proposed: (1) the two-course optimized protocol should be considered a standard-of-care upgrade for women with thin endometrium and concurrent chronic endometritis or vaginal dysbiosis; (2) BTL-4000 magnetotherapy should be initiated prior to PRP infusion to optimize uterine microcirculation; (3) serum IL-6 measurement should be incorporated into pre-conception assessment as a surrogate marker for endometrial inflammatory activity; (4) prospective multicenter randomized controlled trials with live birth rate as the primary outcome should be conducted; and (5) health economics analyses should be performed to establish the cost-effectiveness of this protocol relative to repeated ART cycles.
Ethics Approval
No. 09/2022 (20 December 2022), SamSMU Ethics Committee.
Conflicts of Interest
None.
Funding
Institutional resources.
References
| [1] | Jumayeva F.F., Zaripova D.Ya. Thin endometrium: modern approaches to diagnosis, treatment, and impact on reproductive outcomes. Journal of Humanities and Natural Sciences. 2025; 21: 300–303. |
| [2] | Mutlu M.F., Erdem M., Erdem A. et al. Intrauterine insemination in unexplained infertility: when and how? Turkish Journal of Obstetrics and Gynecology. 2021; 18(2): 121–128. |
| [3] | Lin X., Wei M., Li T. et al. A comparison of intrauterine administration of platelet-rich plasma versus no treatment in women with thin endometrium undergoing in vitro fertilization cycles. Gynecological Endocrinology. 2021; 37(9): 804–808. |
| [4] | Moreno I., Codoñer F.M., Vilella F. et al. Evidence that the endometrial microbiota has an effect on implantation success or failure. American Journal of Obstetrics and Gynecology. 2016; 215(6): 684–703. |
| [5] | World Health Organization. Infertility prevalence estimates, 1990–2021. Geneva: WHO; 2023. |
| [6] | Eftekhar M., Neghab N., Naghshineh E., Khani P. Can autologous platelet rich plasma expand endometrial thickness and improve pregnancy rate during frozen-thawed embryo transfer cycle? A randomized clinical trial. Taiwanese Journal of Obstetrics and Gynecology. 2018; 57(6): 810–813. |
| [7] | Wang Y., Chen Q., Shen F. et al. Effects of low-frequency pulsed electromagnetic fields on uterine blood flow and endometrial thickness in women with thin endometrium. Journal of Assisted Reproduction and Genetics. 2023; 40(4): 837–845. |
| [8] | Chang Y., Li J., Chen Y. et al. Autologous platelet-rich plasma promotes endometrial growth and improves pregnancy outcome during in vitro fertilization. International Journal of Clinical and Experimental Medicine. 2015; 8(1): 1286–1290. |
| [9] | Shchegolev A.I., Tumanova U.N. Physical methods in the treatment of chronic endometritis and thin endometrium: a systematic review. Gynecology. 2022; 24(3): 58–64. |
| [10] | Fazilova M.O., Sultanov S.N. Optimization of management strategies for infertility caused by endometrial hypoplasia. Problems of Biology and Medicine. 2022; (3): 89–94. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML