-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2407-2413
doi:10.5923/j.ajmms.20261605.35
Received: Apr. 26, 2026; Accepted: May 13, 2026; Published: May 15, 2026

Photodynamic Therapy with Povidone-Iodine for Treatment of the Residual Space in Multiple and Recurrent Hepatic Echinococcosis: A Comparative Cohort Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAkhrorova L. B., Khamdamov B. Z., Mirkhodjayev I. A., Hikmatov J. S.
Bukhara State Medical Institute, Bukhara, Republic of Uzbekistan
Correspondence to: Hikmatov J. S., Bukhara State Medical Institute, Bukhara, Republic of Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Hepatic echinococcosis is an endemic parasitic disease in Central Asia with postoperative complication rates of 15–64%, recurrence rates of 2.7–30%, and mortality of up to 38.8% in some regions. Persistent residual space after echinococcectomy is the primary substrate for two distinct categories of adverse outcome: (1) secondary bacterial superinfection - particularly Gram-negative enterobacterial species and anaerobes originating from biliary contamination - producing wound suppuration, residual space abscess, and biliary fistulation; and (2) parasitic reseeding from viable protoscoleces that escape intraoperative evacuation and survive within the fibrous pericyst wall, constituting the biological substrate for disease recurrence. Conventional antiparasitic agents for residual space treatment have significant limitations including toxicity, caustic tissue effects, and suboptimal efficacy against both pathogenic mechanisms. Objectives: To evaluate the clinical efficacy and safety of betadine-based photodynamic therapy (PDT) with low-intensity laser irradiation for residual space treatment after echinococcectomy in multiple and recurrent hepatic echinococcosis, and to characterize the spectral and morphological basis of its antiparasitic activity. Methods: A prospective comparative cohort study was conducted at Bukhara Regional Multidisciplinary Medical Center (2019–2024), enrolling 95 patients with hepatic echinococcosis. Patients were allocated to three groups: Control (n = 43; standard albendazole-based treatment), Group IIA (n = 26; residual space treatment with betadine solution), and Group IIB (n = 26; residual space treatment with betadine solution combined with low-intensity laser irradiation PDT at 630–700 nm). Spectrophotometric analysis of betadine at 0.05–5% concentrations and experimental morphological studies on echinococcal cyst native fluid were conducted to characterize the photodynamic and antiparasitic mechanism. Primary outcomes were specific postoperative complication rate, general complication rate, mortality, and disease recurrence at 1, 2, and 3 years. Results: Spectrophotometric analysis confirmed betadine photodynamic activity in the 630–700 nm red spectrum at concentrations of 0.5–5%. Experimental morphological studies demonstrated complete protoscolex immobilization within 3 minutes and morphological disintegration within 5 minutes when betadine was combined with 630–700 nm laser irradiation. In the clinical cohort, specific postoperative complications were 39.5% in the Control group versus 19.2% in Group IIA and 7.7% in Group IIB (p = 0.001). General complications were 18.6% versus 7.7% and 3.8% respectively (p = 0.02). Mortality was 2.3% in the Control group and 0% in both intervention groups. Disease recurrence at 3-year follow-up was 23.3% in Control, 11.5% in Group IIA, and 3.8% in Group IIB. Conclusions: Betadine PDT with low-intensity laser irradiation is a highly effective, clinically safe, and morphologically substantiated method for residual space treatment after hepatic echinococcectomy, achieving a 5.1-fold reduction in specific complications and a 6.1-fold reduction in disease recurrence compared to standard treatment. Study Novelty: This study provides the first spectrophotometric and experimental-morphological characterization of betadine as a photosensitizer with PDT activity in the 630–700 nm red spectrum, and the first clinical evidence from a comparative cohort demonstrating that betadine-PDT simultaneously eliminates both pathogenic substrates of residual space morbidity - viable protoscoleces and bacterial biofilm - achieving a six-fold reduction in hepatic echinococcosis recurrence compared to standard albendazole-based treatment.
Keywords: Echinococcosis, Liver diseases, Parasitic, Povidone-iodine, Photochemotherapy, Laser therapy, Postoperative complications, Recurrence, Protoscolex, Bacterial superinfection, Residual space
Cite this paper: Akhrorova L. B., Khamdamov B. Z., Mirkhodjayev I. A., Hikmatov J. S., Photodynamic Therapy with Povidone-Iodine for Treatment of the Residual Space in Multiple and Recurrent Hepatic Echinococcosis: A Comparative Cohort Study, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2407-2413. doi: 10.5923/j.ajmms.20261605.35.
Article Outline
1. Introduction
- Hepatic echinococcosis, caused by the larval stage of Echinococcus granulosus, remains a major surgical and public health challenge in endemic regions of Central Asia, the Middle East, and southern Europe, with an estimated global burden of 1–3 million cases annually. [5,6] Surgery remains the mainstay of treatment, yet the clinical results are burdened by postoperative complication rates of 15–64%, disease recurrence rates of 2.7–30%, and mortality figures reaching 3–38.8% in high-burden regions. [5,6,7] The residual fibrous pericyst cavity left after echinococcectomy constitutes the principal anatomical substrate for these adverse outcomes through two distinct and independently important pathogenic mechanisms that must be addressed by any effective residual space treatment strategy.The first mechanism is secondary bacterial superinfection of the residual space. Following cyst evacuation, the fibrous pericyst wall provides an ideal substrate for bacterial colonization due to its avascular nature, impaired local immune defense, and frequent communication with the biliary tree through micro-fistulae. [1,8,12] The predominant causative organisms are Gram-negative enterobacterial species - predominantly Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa - as well as obligate anaerobes including Bacteroides fragilis and Fusobacterium spp., introduced via biliary contamination or hematogenous seeding. [1,12,13] Bacterial colonization of the residual space produces the clinical complications of wound and cavity suppuration, biliary fistulation, and liver abscess, which collectively account for the majority of specific postoperative morbidity in echinococcosis surgery. [1,8]The second mechanism is parasitic reseeding from viable residual protoscoleces. During the process of cyst evacuation, complete removal of all viable protoscoleces from the germinal layer and cyst fluid is surgically challenging, particularly in large, multi-chambered, or deeply embedded cysts. [6,8,11] Protoscoleces that remain viable within the fibrous pericyst wall following incomplete evacuation or spillage can implant on peritoneal surfaces, establish new cysts in the hepatic parenchyma, or disseminate to extrahepatic sites, producing recurrent disease months to years after the index procedure. [6,7,8] This parasitic reseeding - distinct from bacterial infection and not addressed by conventional antibacterial agents - constitutes the primary biological mechanism of post-echinococcectomy disease recurrence and mandates a dedicated scolecidal strategy applied to the residual cavity at the time of surgery. [5,8,11]Conventional antiparasitic agents used for residual space treatment - including hypertonic saline, albendazole, cetrimide, and formalin - carry significant limitations: systemic toxicity, caustic effects on hepatic parenchyma and biliary structures, the need for prolonged contact times, and suboptimal scolecidal efficacy against deeply embedded protoscoleces within the fibrous pericyst wall. [6,8] Crucially, none of these agents simultaneously addresses both pathogenic mechanisms - bacterial contamination and viable protoscolex persistence - with adequate efficacy and an acceptable hepatic safety profile. [8] These shortcomings have motivated the search for alternative physical and pharmacological modalities that combine strong antiparasitic and antimicrobial activity with biological safety for surrounding liver tissue. [8] Among physical approaches, photodynamic therapy (PDT) - defined as the photochemical generation of reactive oxygen species (ROS) through activation of a photosensitizer by light of an appropriate wavelength - has emerged as a promising candidate due to its selective cytotoxic activity against both parasitic and bacterial targets, its low systemic toxicity, and the absence of thermal tissue damage. [2,3,4]Classical photosensitizers employed in clinical PDT (porphyrins, phthalocyanines, chlorins) possess well-characterized photodynamic activity but are limited in widespread surgical application by their high cost, complex pharmacokinetics, prolonged phototoxic residual effects, and dependence on specialized import supply chains. [2,3] Povidone-iodine (betadine), by contrast, is universally available, inexpensive, and already established as a broad-spectrum antiseptic in surgical practice with documented activity against both Gram-negative bacteria, anaerobes, and parasitic organisms. [4,10] Its potential photodynamic properties in the red spectral range - theoretically related to the iodine chromophore's absorption characteristics - have not been systematically characterized until recently, representing a significant gap in the scientific literature. [4,10] Preliminary evidence from Khamdamov et al. suggested that laser PDT applied to the residual space after liver echinococcectomy exerts parasiticidal effects on all germinal elements of the parasite, [4] but a full spectrophotometric characterization of betadine as a photosensitizer, combined with clinical outcomes data from a comparative cohort, has not been reported.The present study was aimed at evaluating the clinical efficacy and safety of betadine-based PDT with low-intensity laser irradiation (LILR) for residual space treatment after hepatic echinococcectomy - addressing both bacterial superinfection and protoscolex reseeding - and to characterize the spectrophotometric and morphological basis of its antiparasitic mechanism in multiple and recurrent hepatic echinococcosis.
2. Materials and Methods
2.1. Study Design and Participants
- A prospective, single-center, comparative three-arm cohort study was conducted at the Bukhara Regional Multidisciplinary Medical Center (BRMMC), Bukhara, Republic of Uzbekistan, between January 2019 and December 2024. The study enrolled 95 consecutive patients with confirmed hepatic echinococcosis (multiple or recurrent forms) who underwent surgical treatment during the study period. Patients were allocated to three groups by sequential assignment: Control group (n = 43), receiving current standard surgical treatment with albendazole-based antiparasitic residual space treatment; Group IIA (n = 26), receiving betadine solution treatment of the residual space after echinococcectomy; and Group IIB (n = 26), receiving betadine solution combined with low-intensity laser irradiation PDT (630–700 nm) for residual space treatment.Inclusion criteria: confirmed cystic echinococcosis of the liver (single, multiple, or recurrent); age ≥ 18 years; indication for surgical echinococcectomy; written informed consent. Exclusion criteria: alveolar echinococcosis; contraindications to general anesthesia; non-operable distant metastatic disease; hemostatic disorders precluding elective surgery; incomplete follow-up data.
2.2. Data Collection Instruments
2.2.1. Preoperative Assessment
- All patients underwent standardized preoperative workup including: clinical history and physical examination; complete blood count with inflammatory markers (leukocyte count, erythrocyte sedimentation rate, C-reactive protein); liver function tests; serological confirmation of echinococcosis (indirect hemagglutination assay and/or ELISA for anti-Echinococcus IgG antibodies); abdominal ultrasound; and contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI) for characterization of cyst number, size, location, and extrahepatic spread. Cyst classification was performed according to the WHO-IWGE classification.
2.2.2. Spectrophotometric Characterization of Betadine
- Absorption and transmission spectra of betadine (povidone-iodine) solutions at concentrations of 0.05%, 0.1%, 0.5%, 1%, and 5% were measured in the wavelength range 300–1000 nm using a UV-Vis spectrophotometer. Optical density at 630–700 nm and the area under the absorption curve (AUC) for the 400–700 nm interval were calculated to characterize photodynamic activity as a function of concentration.
2.2.3. Experimental Morphological Studies
- Two experimental series were conducted using native echinococcal cyst fluid containing protoscoleces obtained intraoperatively. Series 1 assessed the parasiticidal effect of 1%, 5%, and 10% betadine solutions at exposure times of 3, 5, and 7 minutes. Series 2 assessed the combined effect of 1% and 5% betadine with low-intensity laser irradiation (red spectrum 630–700 nm) at 1, 3, and 5 minutes. Morphological changes were evaluated by macro- and microscopic examination (DM-300 optical microscope at ×100–×400 magnification). Assessment criteria were: protoscolex shape, membrane integrity, motility level, and cytoplasmic structural changes.
2.2.4. Surgical Technique and Residual Space Treatment
- All patients underwent semi-closed or ideal echinococcectomy via laparotomy (or thoracophrenotomy where anatomically indicated). Following cyst evacuation and removal of the germinal and laminated layers, residual space treatment was applied according to group assignment. In the Control group, the residual space was treated with 10% albendazole solution (5-minute contact). In Group IIA, 1% betadine (povidone-iodine) solution was instilled into the residual space with 5-minute contact time. In Group IIB, following betadine instillation, low-intensity laser irradiation was applied intracavitarily using a fiber optic probe delivering red-spectrum light at 630–700 nm; irradiation was maintained for 5 minutes at the target power density. All groups subsequently underwent residual space management (capitonnage, omentoplasty, or drainage) according to the surgeon's assessment of cavity size and tissue status.
2.3. Procedures and Follow-Up
- Patients were followed postoperatively at standardized intervals: clinical examination and laboratory assessment at discharge, 1 month, 3 months, 6 months, and then annually for 3 years. Ultrasound examination was performed at each annual visit to detect residual space complications or cyst recurrence. Recurrence was defined as appearance of a new echinococcal cyst confirmed by imaging and serological testing at any follow-up point after surgery. Postoperative complications were classified according to the Clavien-Dindo system and categorized as specific (wound complications, residual space complications) or general (systemic complications).
2.4. Ethical Considerations
- The study was approved by the Ethics Committee of Bukhara State Medical Institute (Ethics Approval No. 05/2019, issued 15 January 2019). The study was conducted in full compliance with the Declaration of Helsinki and applicable national legislation of the Republic of Uzbekistan. Written voluntary informed consent was obtained from all patients prior to enrollment. All data were analyzed anonymously.
2.5. Data Analysis
- Statistical analysis was performed using Microsoft Excel 2021. Continuous variables are reported as mean ± standard error of the mean (M ± SE) and mean ± standard deviation (M ± SD). Between-group differences in categorical outcomes were assessed using the Pearson chi-square (χ²) test with Yates correction where appropriate, or Fisher's exact test for small cell frequencies. Statistical significance was set at p < 0.05 (two-tailed). Relative risk reduction (RRR) and absolute risk reduction (ARR) were calculated for primary outcomes.
3. Results
3.1. Baseline Characteristics
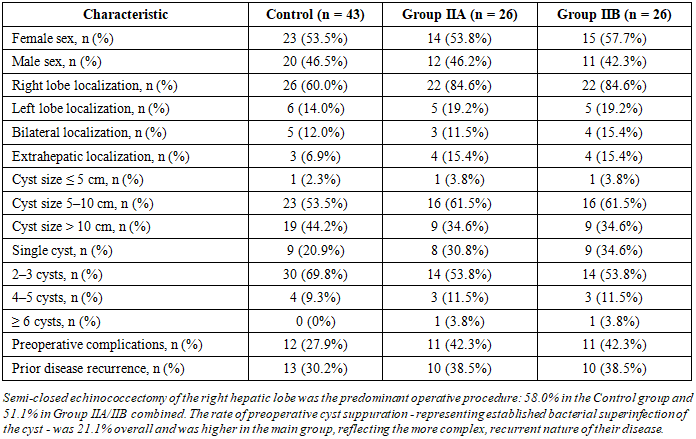
- Of the 95 enrolled patients, 52 (54.7%) were female and 43 (45.3%) were male. The three groups were comparable at baseline with respect to sex distribution, cyst localization, cyst size, number of cysts, preoperative complications, and prior recurrence status. Baseline characteristics are summarized in Table 1.
|
3.2. Spectrophotometric and Morphological Characterization
- Spectrophotometric analysis demonstrated that betadine absorption increased progressively with concentration across the 300–1000 nm range. At concentrations of 0.5–5%, the absorption spectrum extended into the red spectral range of 630–700 nm, confirming genuine photodynamic activity at clinically applicable concentrations.In Series 1 of the experimental morphological study, dose- and time-dependent parasiticidal effects of betadine on protoscoleces were confirmed. At concentrations of 5% and 10%, membrane integrity disruption, cellular disorganization, and morphological lysis were observed at 5–7 minutes. In Series 2, the combination of betadine with low-intensity laser irradiation at 630–700 nm produced markedly accelerated parasiticidal responses: complete protoscolex immobilization at 3 minutes and complete morphological disintegration at 5 minutes. These results confirm that PDT-mediated generation of reactive oxygen species produces irreversible destruction of protoscolex membrane lipids and proteins within a clinically practical intraoperative time window.
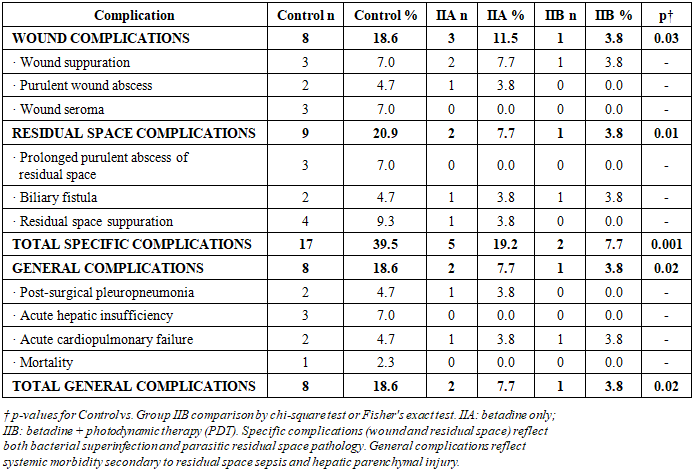
3.3. Postoperative Complications
- The analysis of postoperative complications demonstrated a statistically significant progressive reduction in both specific and general complication rates from the Control group through Group IIA to Group IIB (Table 2).
|
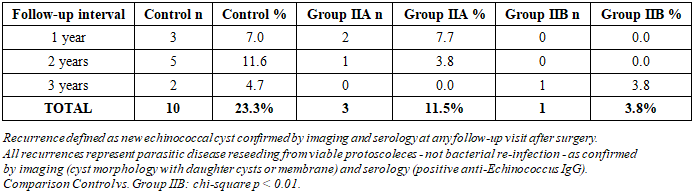
3.4. Disease Recurrence
- The 3-year follow-up recurrence data are presented in Table 3. In the Control group, recurrence was documented in 10 patients (23.3%), with the predominant recurrences occurring at 2 years (11.6%), consistent with the typical 18–36-month latency period for protoscolex-derived new cyst formation following incomplete intraoperative scolecidal treatment.
|
4. Discussion
- The present study was aimed at evaluating the clinical efficacy and safety of betadine-based photodynamic therapy for residual space treatment after hepatic echinococcectomy in multiple and recurrent hepatic echinococcosis. The most important finding was the 5.1-fold reduction in specific postoperative complications and the 6.1-fold reduction in disease recurrence in the betadine PDT group compared to standard treatment. The complete elimination of mortality in both intervention groups further underscores the clinical significance of optimized residual space management.The present findings extend and mechanistically corroborate the earlier work of Khamdamov et al. (2022), who demonstrated that laser PDT after hepatic echinococcectomy affects all germinal elements of the parasite without macroorganism toxicity. [4] The current study fills this gap by demonstrating for the first time that betadine at 0.5–1% concentrations exhibits genuine photodynamic absorption activity in the 630–700 nm red spectrum. This spectral characterization distinguishes betadine from classical antiseptics and positions it as a dual-function agent - simultaneously addressing both pathogenic substrates of residual space morbidity: (1) bacterial biofilm elimination through its established broad-spectrum antiseptic activity against Gram-negative enterobacteria and anaerobes; [1,12,13] and (2) protoscolex inactivation through PDT-mediated ROS generation producing irreversible membrane oxidative injury. [2,3,4]The complication reduction observed in Group IIA (betadine alone, without laser) - 2.1-fold reduction in specific complications - indicates that betadine itself provides measurable clinical benefit over albendazole through its broader antiseptic spectrum and direct contact scolecidal activity. [1] The additional 2.4-fold incremental benefit in Group IIB (betadine + PDT) confirms that PDT activation produces a synergistic parasiticidal and antimicrobial effect. This is consistent with the established PDT mechanism: photochemically generated singlet oxygen and ROS from iodine chromophore activation produce non-selective oxidation of both parasite membrane lipids and proteins and bacterial cell wall components - a mechanism against which neither protoscoleces nor bacteria have acquired resistance. [2,3] The observed progressive reduction in residual space suppuration from 9.3% (Control) to 3.8% (IIA) to 0% (IIB) reflects this dual mechanism: Group IIA reduces bacterial contamination through antiseptic activity, while Group IIB additionally eliminates the pro-inflammatory substrate maintained by residual parasitic tissue. [3,12] Abdelraouf et al. previously showed that omentoplasty is an effective residual space filling strategy, [1] and the present study suggests that betadine PDT may be combined with omentoplasty to achieve both biological decontamination and mechanical space elimination.All 14 recurrences documented across all three groups over 3 years were confirmed as parasitic reseeding - new cysts arising from viable protoscoleces - rather than bacterial re-infection of the residual space, as confirmed by characteristic cyst morphology on ultrasound or CT (daughter cysts, laminated membrane) and positive serological testing for anti-Echinococcus IgG. [5,6,11] The temporal distribution of recurrences - predominantly at 1–2 years - is consistent with the known biological latency of protoscolex-to-cyst development, which typically requires 6–24 months following implantation. [6,7] The elimination of year-1 and year-2 recurrences in Group IIB, with only a single late recurrence at year 3, suggests that betadine PDT substantially inactivates the viable protoscolex pool but may not completely eliminate deeply embedded germinal elements in the most complex cysts - a finding that supports the proposed recommendation for its use in combination with prolonged postoperative albendazole chemoprophylaxis.This study has several limitations. First, the non-randomized comparative cohort design introduces potential selection bias. Second, the study was conducted at a single center. Third, the 3-year follow-up may underestimate very late recurrences. Fourth, microbiological characterization of bacterial isolates from infected residual spaces - which would have allowed precise identification of the causative organisms - was not systematically performed. Future studies should incorporate culture and sensitivity data from residual space specimens to characterize the bacterial pathogen spectrum and confirm the antiseptic spectrum of betadine PDT against the specific organisms encountered. [12,13] Strengths include the prospective design, integration of spectrophotometric and morphological mechanistic characterization with clinical outcomes, the meaningful 3-year follow-up, and the demonstration of benefit in both intermediate (betadine only) and full PDT intervention arms.
5. Conclusions
- Betadine-based photodynamic therapy with low-intensity laser irradiation at 630–700 nm is an effective, safe, and mechanistically substantiated method for treatment of the residual space after hepatic echinococcectomy. Its clinical superiority over albendazole-based treatment derives from its simultaneous action against both pathogenic substrates of residual space morbidity: bacterial superinfection - through established broad-spectrum antiseptic activity - and parasitic reseeding from viable protoscoleces - through PDT-mediated ROS generation producing irreversible protoscolex membrane oxidation. Spectrophotometric analysis confirmed genuine photodynamic activity of betadine in the 630–700 nm red spectrum. Experimental morphological studies demonstrated complete protoscolex immobilization within 3 minutes and irreversible disintegration within 5 minutes. In the clinical cohort, betadine PDT achieved a 5.1-fold reduction in specific postoperative complications (7.7% vs. 39.5%), a 4.9-fold reduction in general complications (3.8% vs. 18.6%), complete elimination of mortality (0% vs. 2.3%), and a 6.1-fold reduction in 3-year disease recurrence (3.8% vs. 23.3%) compared to standard albendazole-based treatment.From a health policy perspective, the evidence generated by this study supports the revision of national surgical protocols for hepatic echinococcosis in Uzbekistan and analogous endemic settings to include betadine PDT as a standard-of-care residual space treatment. Its universal availability, low cost, and dual antibacterial and antiparasitic mechanism make it particularly valuable in endemic resource-constrained settings.The following recommendations are proposed: (1) betadine solution at 0.5–1% combined with low-intensity laser irradiation at 630–700 nm should be adopted as the standard residual space treatment after hepatic echinococcectomy in multiple and recurrent disease; (2) a minimum contact time of 5 minutes should be ensured; (3) microbiological culture of residual space specimens should be routinely performed to characterize the bacterial superinfection spectrum and guide adjuvant antibiotic selection; (4) the method should be evaluated in a multicenter randomized controlled trial with immunological outcomes and long-term follow-up exceeding 5 years; and (5) the combination of betadine PDT with postoperative albendazole chemoprophylaxis should be investigated as a strategy to eliminate the residual risk of late protoscolex-derived recurrence.
Ethics Approval
- Ethics Committee of Bukhara State Medical Institute, No. 05/2019 (15 January 2019).
Conflicts of Interest
- None declared.
Funding
- Institutional resources only. No external funding was received.