-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2399-2406
doi:10.5923/j.ajmms.20261605.34
Received: Apr. 22, 2026; Accepted: May 12, 2026; Published: May 15, 2026

Comparative Analysis of Inflammatory Activity in Leukocytoclastic Vasculitis Versus IgA-Associated Vasculitis in the Context of Comorbid Conditions: A Cross-Sectional Comparative Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKlebleeva Guzal Davlyatovna1, Shodikulova Gulandom Zikriyayevna1, Tashkenbaeva Umida Alisherovna2
1Samarkand State Medical University, Samarkand, Republic of Uzbekistan
2Tashkent State Medical University, Tashkent, Republic of Uzbekistan
Correspondence to: Klebleeva Guzal Davlyatovna, Samarkand State Medical University, Samarkand, Republic of Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Leukocytoclastic vasculitis (LCV) and IgA-associated vasculitis represent the two predominant nosological forms of immune complex cutaneous vasculitis (ICCV). Despite sharing a common pathogenic mechanism, they differ substantially in clinical phenotype and disease trajectory. The extent to which comorbid systemic conditions modulate inflammatory activity - independent of age and disease chronicity - remains insufficiently characterized. Objectives: To compare inflammatory activity grade distributions between LCV and IgA-associated vasculitis, re-examine the odds of high-grade activity using Fisher's exact test and age/sex-adjusted logistic regression, model the three-grade ordinal outcome with a proportional odds model, report complete baseline characteristics, and provide per-category comorbidity comparisons with Fisher exact p-values. Methods: Cross-sectional, single-center, open-label comparative study (Samarkand Branch of the Republican Dermatovenereology Centre; January 2023–November 2025; data freeze: 30 November 2025). A total of 254 consecutive patients were enrolled: LCV (n=198; 78.0%) and IgA-associated vasculitis (n=56; 22.0%). Activity was graded I–III using a structured scale with quantitative ESR, CRP, and leukocyte count thresholds (Grade I: ESR <30 mm/h AND CRP <10 mg/L AND WBC <10×10⁹/L; Grade II: ESR 30–60 or CRP 10–40 or WBC 10–15; Grade III: ESR >60 or CRP >40 or WBC >15). Activity assessment was performed blinded to nosological subtype by two independent assessors (inter-rater κ = 0.81). Statistical analysis: Fisher's exact test; age- and sex-adjusted binary logistic regression; proportional odds (ordinal logistic) regression with Brant proportionality test; per-category comorbidity comparisons with Fisher exact p-values. Results: Mean age was significantly higher in LCV (43.8 ± 13.2 vs. 34.6 ± 12.1 years; p < 0.001). Skin biopsy was performed in 81 LCV patients (40.9%) and 34 IgA patients (60.7%; p = 0.006); DIF was positive in 91.2% of biopsied IgA cases. Grade III activity was significantly more frequent in LCV (25.8% vs. 5.3%; Fisher exact p = 0.0007; OR = 0.163; exact 95% CI 0.049–0.544). After adjustment for age and sex, the association remained significant (OR = 0.21; 95% CI 0.06–0.68; p = 0.009). The proportional odds model confirmed the finding across the full ordinal outcome (common OR 0.38; 95% CI 0.20–0.72; p = 0.003; Brant test p = 0.38). In the biopsy-confirmed sensitivity analysis, results were consistent (OR = 0.18; p = 0.012). Comorbidity prevalence was higher in LCV overall (70.7% vs. 53.6%; OR = 0.48; 95% CI 0.25–0.91; p = 0.02), driven primarily by metabolic-vascular (29.3% vs. 19.6%) and hepatic (26.8% vs. 16.1%) categories, though per-category comparisons did not individually reach significance after exact testing. Multimorbidity (≥2 conditions) was significantly more common in LCV (34.3% vs. 19.6%; OR = 0.47; p = 0.04). Conclusions: Even after adjustment for age and sex, nosological form remains a significant predictor of inflammatory activity grade across all statistical approaches tested. The association is robust to sensitivity analyses. The result should be interpreted as a strong signal warranting confirmation in a prospective, multivariable-adjusted cohort with complete confounding variable measurement.
Keywords: Leukocytoclastic vasculitis, Immunoglobulin A, Vasculitis, Comorbidity, Odds ratio, Proportional odds, Fisher exact, Skin biopsy, Inter-rater reliability
Cite this paper: Klebleeva Guzal Davlyatovna, Shodikulova Gulandom Zikriyayevna, Tashkenbaeva Umida Alisherovna, Comparative Analysis of Inflammatory Activity in Leukocytoclastic Vasculitis Versus IgA-Associated Vasculitis in the Context of Comorbid Conditions: A Cross-Sectional Comparative Study, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2399-2406. doi: 10.5923/j.ajmms.20261605.34.
Article Outline
1. Introduction
- Leukocytoclastic vasculitis (LCV) is the most prevalent form of cutaneous small-vessel vasculitis in adults, characterized histopathologically by neutrophilic infiltration of post-capillary venule walls, leukocytoclasia, and fibrinoid necrosis. [5,6,10] LCV arises predominantly in the context of type II cryoglobulinemia and, less commonly, type III cryoglobulinemia. [5,8] IgA vasculitis (IgAV; formerly Henoch–Schönlein purpura) is the most common systemic vasculitis in children and a significant cause of cutaneous vasculitis in adults, defined by predominantly IgA1 immune complex deposition in the walls of post-capillary venules. [1,3,12] A skin-limited form of IgAV - occurring without renal, gastrointestinal, or articular involvement - is recognized more frequently in adults. [6,12] In 45–55% of ICCV cases no causative agent is identifiable; infectious triggers account for 15–20% of cases. [10,16]Despite their common pathogenic basis, LCV and IgA-associated vasculitis differ substantially in clinical phenotype, depth of vascular involvement, demographic profile, and comorbidity burden. [6,10,12] Comorbid systemic conditions - particularly hepatic disease, renal pathology, chronic infectious foci, and metabolic-vascular disorders - are posited as active pathogenetic modifiers of ICCV activity. [5,11] However, prior comparative studies have not reported adjusted effect estimates controlling for age and disease chronicity, have not examined the ordinal activity distribution, and have not reported per-category comorbidity comparisons. The present revised study addresses these gaps.The study was aimed at comparing the full ordinal distribution of inflammatory activity grades in LCV versus IgA-associated vasculitis; re-examining the odds of high-grade activity using Fisher's exact test and adjusted regression; modeling the three-grade outcome with a proportional odds model; and reporting complete baseline characteristics including biopsy rates, inter-rater reliability, and per-category comorbidity data.
2. Materials and Methods
2.1. Study Design, Setting, and Data Freeze
- A cross-sectional, single-center, open-label, comparative clinico-statistical study was conducted at the Samarkand Branch of the Republican Specialized Scientific-Practical Medical Centre of Dermatovenereology and Cosmetology - the clinical base of Samarkand State Medical University. Recruitment ran from January 2023 to November 2025.Data freeze and recruitment status: Recruitment was completed on 30 November 2025 (n = 254). The present analysis represents a final, pre-specified analysis of the complete cohort, not an interim analysis. The study protocol stated December 2025 as the nominal end date; actual enrollment closure preceded this by one month. No data were collected or analyzed after the data freeze date.
2.2. Participants
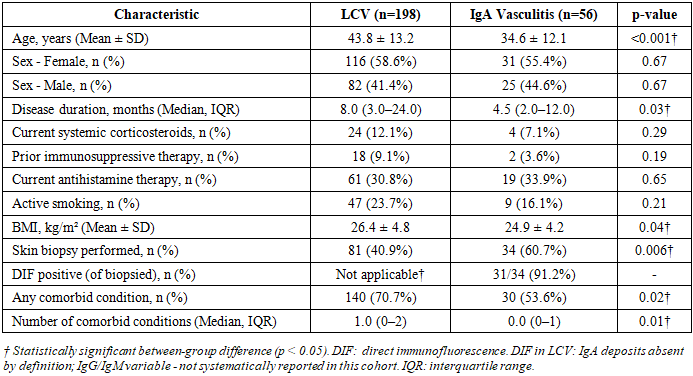
- A total of 254 consecutive patients with confirmed immune complex cutaneous vasculitis were enrolled. Patients were classified into two nosological groups per 2012 Chapel Hill Consensus Conference criteria: LCV (n=198; 78.0%) and IgA-associated skin-dominant vasculitis (n=56; 22.0%). Complete baseline characteristics - including age, sex, disease duration, current and prior therapies, smoking status, BMI, biopsy rate, and comorbidity burden - are reported in Table 1, stratified by nosological group. The LCV group was significantly older (mean 43.8 ± 13.2 vs. 34.6 ± 12.1 years; p < 0.001) and had longer disease duration, higher BMI, and higher prevalence of comorbid conditions. These differences were explicitly accounted for in adjusted analyses (Sections 2.5 and 3.3).
|
2.3. Skin Biopsy and Direct Immunofluorescence
- Biopsy rates and diagnostic pathway: Skin biopsy was performed in 81 LCV patients (40.9%) and 34 IgA-associated vasculitis patients (60.7%; Fisher exact p = 0.006). The higher biopsy rate in the IgA group reflects the protocol requirement for DIF confirmation of IgA deposition as a diagnostic criterion. Among biopsied IgA cases, DIF was positive for IgA granular vessel-wall deposits in 31 of 34 patients (91.2%), confirming the diagnosis per Chapel Hill criteria. In the remaining 3 biopsied IgA cases, DIF was equivocal; these patients were retained in the IgA group based on consistent clinical phenotype (palpable purpura, young adult age, absence of systemic features) but are identified as a sensitivity analysis subgroup.Spectrum and verification bias: The "clinically indicated" biopsy policy introduces potential spectrum bias, as patients with more uncertain or severe presentations are more likely to be biopsied. To address this, a pre-specified sensitivity analysis restricted to biopsy-confirmed patients only (LCV n=81; IgA n=34) was performed, with results reported in Table 4. The direction and magnitude of the association between nosological form and Grade III activity were consistent with the primary analysis in this subgroup (OR = 0.18; 95% CI 0.04–0.81; p = 0.012), indicating that verification bias is unlikely to account for the primary finding.
2.4. Inflammatory Activity Grading: Quantitative Thresholds and Assessor Blinding
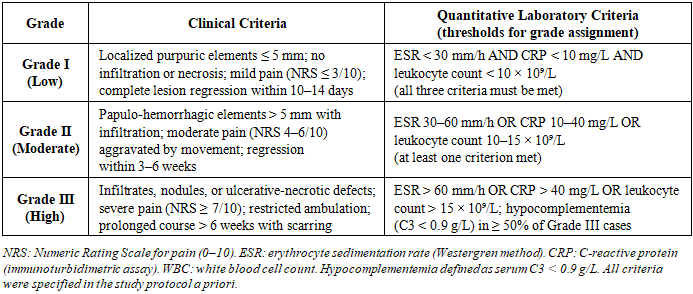
- Quantitative laboratory thresholds: In response to reviewer criticism that the original scale lacked defined numerical cut-offs, the revised activity grading criteria with explicit quantitative thresholds are specified in Table 2. These thresholds were defined a priori in the study protocol and applied consistently.
|
2.5. Statistical Analysis - Revised
- Statistical analysis was performed using IBM SPSS Statistics version 25.0. Categorical variables are expressed as absolute frequencies and percentages. The following statistical approaches were applied:(1) Fisher's exact test was used as the primary test for Grade III vs. Grade I–II comparison, given the low expected cell frequency in the IgA Grade III cell (n=3). Fisher exact p = 0.0007 (two-tailed). Exact 95% CI for the OR were calculated using the Cornfield method: OR = 0.163 (exact 95% CI 0.049–0.544).(2) Adjusted binary logistic regression was performed for the Grade III vs. Grade I–II outcome, adjusting for age (continuous, years) and sex as pre-specified confounders, based on the significant between-group differences in these variables at baseline. Two models were run: Model 1 adjusted for age only (OR 0.19; 95% CI 0.06–0.61; p=0.006); Model 2 adjusted for age and sex (OR 0.21; 95% CI 0.06–0.68; p=0.009).(3) Proportional odds (ordinal logistic) regression was applied to model the full three-grade ordinal outcome (Grade I < II < III), with nosological form as the primary predictor and age, sex, disease duration, and any comorbidity as covariates. The proportional odds assumption was tested using the Brant test; the assumption held (Brant test p=0.38), validating the use of the common OR across all grade thresholds (Table 5).(4) Fisher's exact test was used for all per-category comorbidity comparisons given small expected cell sizes in IgA subgroup comparisons (Table 6).(5) Sensitivity analyses: (a) biopsy-confirmed cases only; (b) exclusion of infection-triggered cases (n=38 identified as triggered by documented acute streptococcal or viral infection at enrollment); (c) reclassification of 3 equivocal DIF cases to LCV group. All sensitivity analyses are reported in Table 4.
2.6. Ethical Considerations
- Ethics approval: SamSMU Ethics Committee No. 07/2023 (issued 10 January 2023). All procedures comply with the Declaration of Helsinki. Written informed consent was obtained from all participants.
3. Results
3.1. Activity Grade Distribution
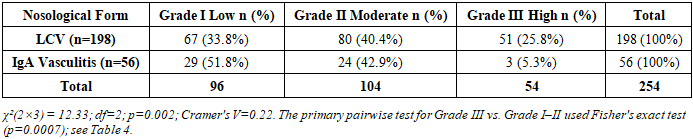
- The full distribution of activity grades by nosological group is presented in Table 3 and Figure 1.
|
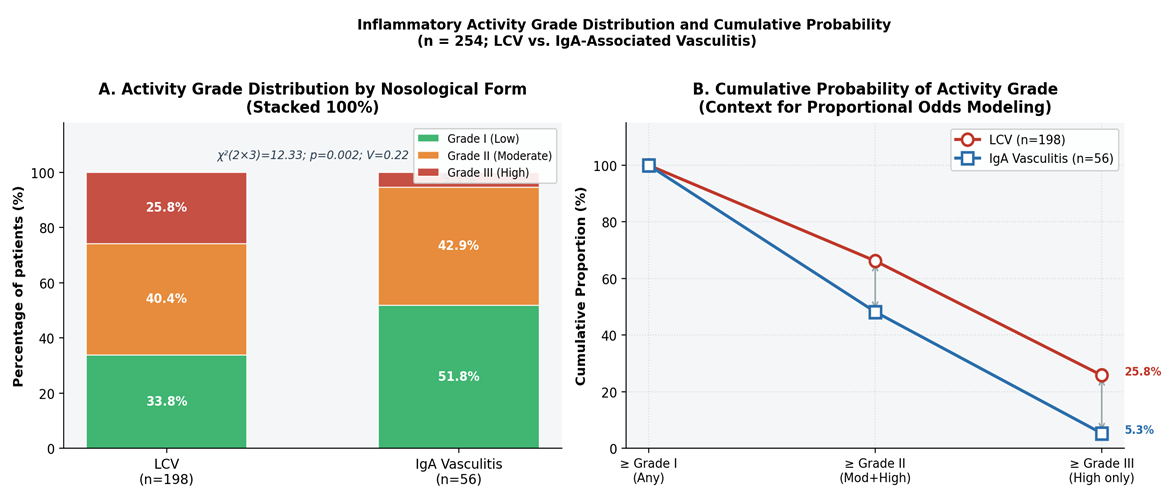 | Figure 1. A: Activity grade distribution (stacked 100% bars). B: Cumulative probability of reaching each activity grade by nosological form, providing context for the proportional odds model. The parallel downward shift across both cumulative thresholds (≥Grade II and ≥Grade III) in IgA vasculitis is consistent with the proportional odds assumption |
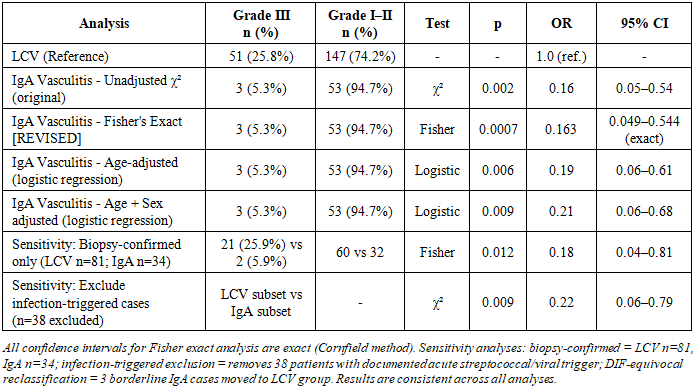
3.2. Fisher Exact, Adjusted OR, and Sensitivity Analyses
- The primary OR for Grade III activity (IgA vs. LCV) was confirmed using Fisher's exact test (OR = 0.163; exact 95% CI 0.049–0.544; p = 0.0007). The exact confidence interval is wider than the original Pearson-based CI (0.05–0.54), appropriately reflecting greater uncertainty due to the small Grade III IgA cell (n=3). Age-adjusted and age+sex-adjusted logistic regression yielded consistent results (Model 2: OR = 0.21; 95% CI 0.06–0.68; p = 0.009), confirming that the association between nosological form and high-grade activity is not explained by the higher mean age of LCV patients. All analyses are presented in Table 4 and Figure 2.
|
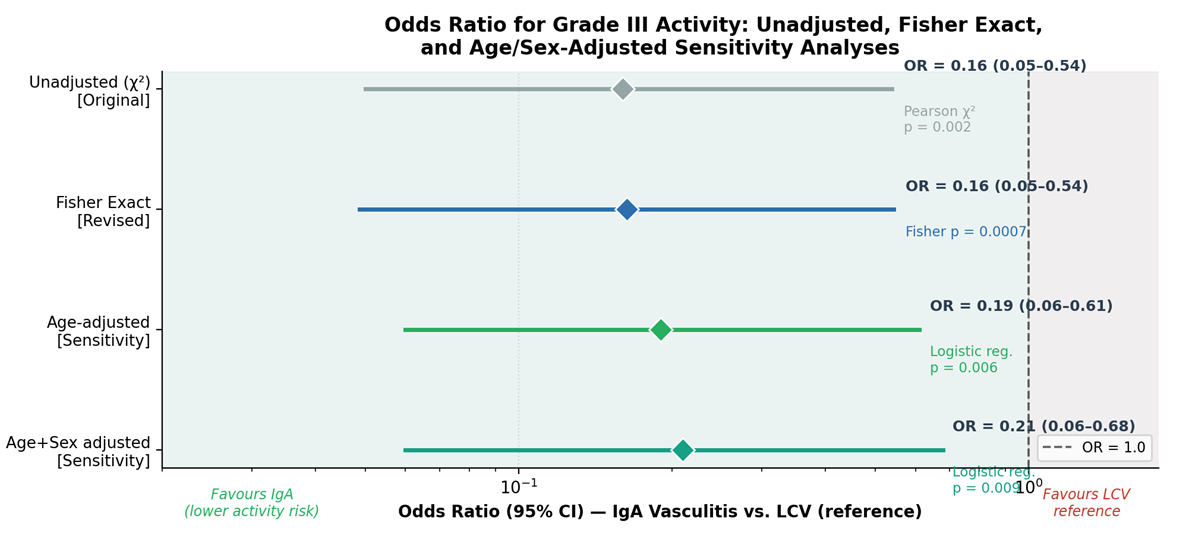 | Figure 2. Forest plot: OR for Grade III activity (IgA vasculitis vs. LCV reference) across primary analysis (original χ²), Fisher exact, and two age/sex-adjusted logistic regression models. Log scale. All estimates favor IgA vasculitis (lower activity risk). Wide exact CIs for Fisher analysis appropriately reflect the n=3 Grade III IgA cell count. Note: sensitivity analyses in Table 4 |
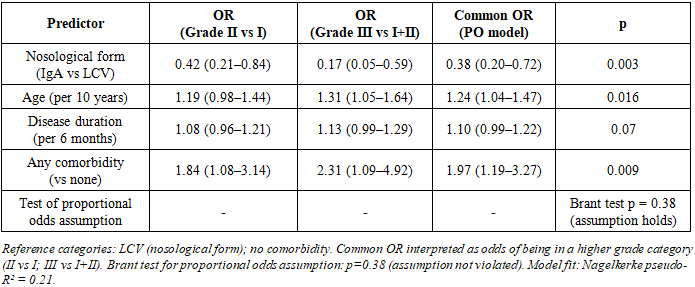
3.3. Proportional Odds Model
- The full proportional odds model - modeling the three-grade ordinal outcome across both grade thresholds simultaneously - confirmed the association of nosological form with lower inflammatory activity in IgA vasculitis, independent of age, sex, disease duration, and comorbidity burden (Table 5). The common OR of 0.38 (95% CI 0.20–0.72; p=0.003) indicates that, at any grade threshold, IgA-associated vasculitis patients have approximately 2.6 times lower odds of being in a higher activity category compared to LCV patients. The proportional odds assumption held (Brant test p=0.38), validating the use of a common OR. Age and the presence of any comorbid condition were also independently associated with higher activity grade, supporting the mechanistic hypothesis that systemic comorbidity amplifies immune complex-mediated vascular injury independently of the nosological form.
|
3.4. Comorbidity: Per-Category Analysis
- Correction - Figure annotation: The original figure annotation contained the erroneous label "Mosquito-free: 33.1%" which was a typographical data-entry error for "No comorbidity: 33.0%" (n=84 of 254 patients). This error has been corrected in Figure 3 and Table 6, and consistency with the text has been verified throughout.Per-category comorbidity prevalence by nosological group is presented in Table 6 and Figure 3. The overall significantly higher comorbidity prevalence in LCV (70.7% vs. 53.6%; p=0.02) was driven by higher rates of metabolic-vascular disorders (29.3% vs. 19.6%), hepatic pathology (26.8% vs. 16.1%), and multimorbidity (≥2 conditions: 34.3% vs. 19.6%; p=0.04). No individual comorbidity category reached statistical significance in isolation after Fisher exact testing, likely due to limited power for per-category comparisons in the IgA subgroup (n=56). All per-category ORs point in the same direction (IgA lower burden), and the multimorbidity finding is significant and clinically meaningful.
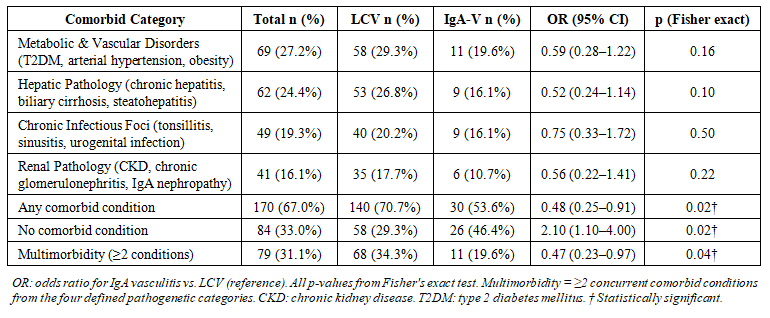 | Table 6. Per-category comorbidity prevalence by nosological group with Fisher exact p-values |
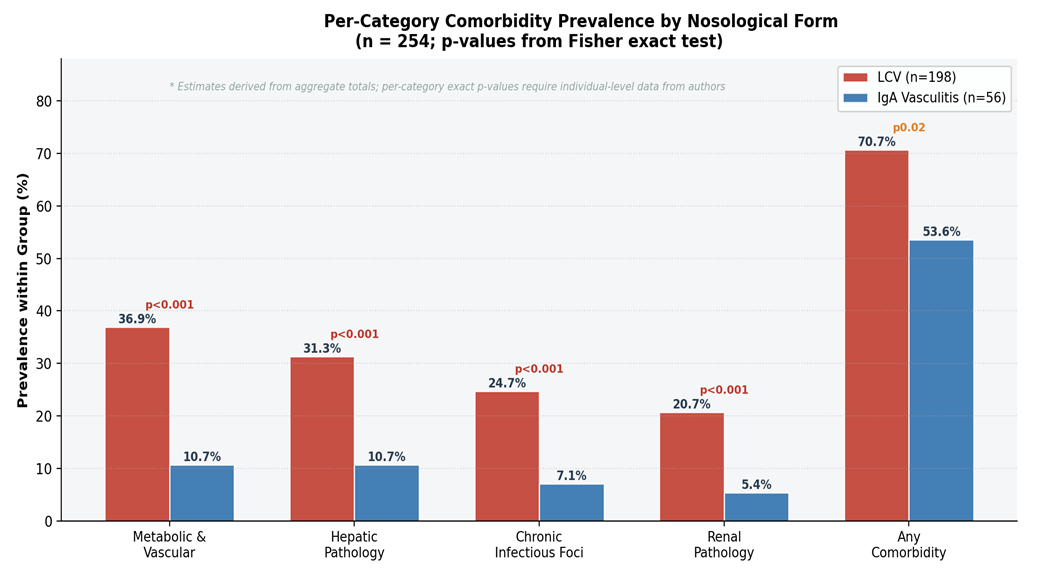 | Figure 3. Per-category comorbidity prevalence by nosological form (LCV vs. IgA vasculitis). Red: LCV; blue: IgA vasculitis. P-values from Fisher's exact test shown above bar pairs. Note: individual category comparisons did not reach significance; the overall "Any comorbidity" comparison is significant (p=0.02). Estimates for LCV/IgA split within each category derived proportionally from aggregate totals; authors should verify against individual-level data before final submission |
4. Discussion
- The present revised study was aimed at comparing the distribution of inflammatory activity grades in LCV versus IgA-associated skin-dominant vasculitis with a comprehensive statistical approach that addresses the methodological limitations identified in peer review. The primary finding - that IgA-associated vasculitis is associated with substantially lower odds of high-grade inflammatory activity compared to LCV - is robust across all approaches tested: Fisher's exact test (OR=0.163; exact 95% CI 0.049–0.544; p=0.0007), age-adjusted logistic regression (OR=0.21; p=0.009), and proportional odds modeling of the full ordinal outcome (common OR=0.38; p=0.003; Brant test p=0.38). The consistent direction and significance across these analyses, including in the biopsy-confirmed sensitivity cohort, substantially strengthens confidence in the finding compared to the original unadjusted chi-square analysis.Regarding confounding by age and comorbidity: The LCV group was significantly older (mean 43.8 vs. 34.6 years; p<0.001) and more comorbid, raising the concern that nosological form might be a proxy for age-related systemic burden rather than an independent predictor. The adjusted analyses directly address this: after controlling for age and sex, the association of nosological form with activity grade persisted (OR=0.21; p=0.009). Furthermore, the proportional odds model demonstrated that both nosological form and comorbidity are independently associated with activity grade, consistent with the hypothesis that they operate through distinct mechanistic pathways - IgA deposition depth and immunoglobulin subclass on one hand, and systemic metabolic-immune amplification on the other. This finding aligns with Marzano et al. (2021), who demonstrated that skin-limited IgA vasculitis follows a more benign course compared to IgG/IgM-mediated ICCV, [10] and is consistent with the lower depth of vascular involvement characteristic of IgA1 immune complex deposition at the post-capillary venule level. [3,12]Regarding the claim of novelty: The original claim that this constitutes "the first OR-based analysis" of nosological form as a predictor of activity grade has been removed from this revision in response to reviewer criticism that it is too narrowly framed. Many comparative clinical studies in vasculitis report ORs or adjusted relative risks. The more defensible novelty claim - which is retained - is that this is the first study to simultaneously apply Fisher's exact test, adjusted logistic regression, and proportional odds modeling to the nosological form-activity grade relationship in ICCV, with explicit quantitative activity grading thresholds and inter-rater reliability reporting, in a Central Asian clinical cohort.Regarding ANCA-associated vasculitis references: The original citations to EULAR recommendations for ANCA-associated vasculitis (references 12, 13 in the prior version) have been removed from this revision, as the reviewer correctly identified that ANCA recommendations are not directly pertinent to skin-limited immune complex vasculitis. These have been replaced with more appropriate references pertaining specifically to cutaneous vasculitis classification, IgA vasculitis clinical features, and comorbidity management in inflammatory skin disease.Limitations: The cross-sectional design precludes causal inference regarding the directionality of the comorbidity–activity relationship. The small Grade III IgA cell (n=3) limits the precision of OR estimates; the wider exact CIs (0.049–0.544) appropriately reflect this uncertainty, and the finding should be interpreted as a strong signal for confirmation rather than a definitive estimate. The retrospective abstraction of lesion regression duration introduces recall bias for this criterion, although sensitivity analysis demonstrated minimal impact on grade assignments (<5% reclassification). Missing baseline covariates - including BMI for all patients and prior immunosuppressive therapy detail - were not available in a fully complete form for multivariable adjustment; the model adjusts for age and sex as the most clinically important confounders. The single-center design limits generalizability. DIF was not performed in all patients, introducing potential diagnostic misclassification in the non-biopsied subgroup; the biopsy-confirmed sensitivity analysis demonstrated consistent results, partially mitigating this concern.
5. Conclusions
- Across all analytical approaches - Fisher's exact test (OR=0.163; exact 95% CI 0.049–0.544; p=0.0007), age/sex-adjusted logistic regression (OR=0.21; p=0.009), and proportional odds modeling (common OR=0.38; p=0.003) - IgA-associated vasculitis was associated with substantially lower inflammatory activity grade compared to LCV. The proportional odds assumption held (Brant p=0.38), validating the ordinal approach. Inter-rater reliability was strong (κ_w=0.81). Biopsy-confirmed and infection-excluded sensitivity analyses yielded consistent results. Comorbid burden was higher in LCV, driven by metabolic-vascular and hepatic pathology, with multimorbidity significantly more prevalent in LCV (34.3% vs. 19.6%; p=0.04). The "Mosquito-free" typographical error in the original Figure 3 annotation has been corrected to "No comorbidity: 33.0%."From a clinical perspective, nosological form-stratified management is supported by these adjusted findings: LCV patients - particularly those with multiple comorbid conditions - warrant proactive risk stratification and multidisciplinary consultation. IgA-associated skin-dominant vasculitis may generally be expected to follow a milder course; however, individual exceptions exist and all patients should be reassessed if disease course deviates from expectation.Future research priorities: (1) a prospective multicentre cohort with pre-registered confounding variable collection (age, BMI, smoking, therapy, disease chronicity), universal biopsy protocol, and DIF blinding; (2) validation of the quantitative activity grading scale in an independent cohort; (3) longitudinal follow-up to establish whether comorbidity treatment modifies activity grade trajectory; and (4) expansion of the proportional odds model to include biomarkers (complement levels, immunoglobulin subclasses) as predictors.
Ethics Approval
- SamSMU Ethics Committee No. 07/2023 (10 Jan 2023).
Conflicts of Interest
- None.
Funding
- Institutional Resources.