-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2394-2398
doi:10.5923/j.ajmms.20261605.33
Received: Apr. 19, 2026; Accepted: May 2, 2026; Published: May 15, 2026

Characteristics of CD3 Marker Expression in Mesenteric Lymph Nodes in Necrotizing Enterocolitis in Infants
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLChartakov D. K.1, Don A. N.2, Mamatalieva M. A.1
1Andijan State Medical Institute, Uzbekistan
2Tashkent State Medical University, Uzbekistan
Correspondence to: Chartakov D. K., Andijan State Medical Institute, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study analyzed histomorphological and immunohistochemical alterations in mesenteric lymph nodes using 200 biopsy specimens obtained from infants diagnosed with necrotizing enterocolitis (NEC) between 2015 and 2026. In the early neonatal period (0-7 days), mesenteric lymph nodes demonstrated structural immaturity and incomplete morphogenesis. A pronounced T-cell deficiency was identified, characterized by a significant reduction in CD3+ T lymphocytes, with low expression observed in 65.71% of cases. A compensatory activation of the B-cell compartment was noted in response to T-cell insufficiency. During age-related progression, by the late neonatal period (8-28 days), a marked maturation of functional zones within mesenteric lymph nodes was observed. CD3 expression increased approximately 3.33-fold compared with the early neonatal period, indicating partial restoration of T-cell-mediated immune activity. In NEC cases presenting as part of a systemic inflammatory response syndrome (SIRS), migration of activated lymphocytes toward inflammatory foci was observed. This process contributed to lymphoid depletion, structural collapse of lymphoid tissue, and the development of secondary immunodeficiency in mesenteric lymph nodes.
Keywords: Neonates, Early and late neonatal period, Necrotizing enterocolitis, Mesenteric lymph nodes, Immunohistochemistry, CD3+ T lymphocytes, B lymphocytes, Systemic inflammatory response, Secondary immunodeficiency
Cite this paper: Chartakov D. K., Don A. N., Mamatalieva M. A., Characteristics of CD3 Marker Expression in Mesenteric Lymph Nodes in Necrotizing Enterocolitis in Infants, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2394-2398. doi: 10.5923/j.ajmms.20261605.33.
1. Introduction
- Necrotizing enterocolitis (NEC) is a severe inflammatory gastrointestinal disease that primarily affects premature and very low birth weight neonates and remains a major cause of neonatal morbidity and mortality worldwide [1,2]. Despite advances in neonatal intensive care, the clinical outcomes of NEC remain poor due to its rapid progression and multifactorial pathogenesis [1].The development of NEC is associated with intestinal immaturity, ischemia-reperfusion injury, microbial dysbiosis, and dysregulated innate and adaptive immune responses [2,3]. These mechanisms collectively lead to epithelial barrier breakdown and excessive intestinal inflammation [3,4]. Recent studies indicate that immune dysregulation plays a central role in NEC pathogenesis, particularly involving Toll-like receptor 4 (TLR4)-mediated activation of the immature intestinal epithelium, which triggers inflammatory cascades and immune cell recruitment. This process results in exaggerated mucosal inflammation and tissue injury. Mesenteric lymph nodes (MLNs) are a critical component of intestinal immunity, functioning as the primary site for antigen presentation and lymphocyte activation in response to gut-derived microbial and inflammatory stimuli. In NEC, MLNs are actively involved in immune regulation and disease progression due to continuous antigenic stimulation [5,6,7].Experimental and clinical studies have demonstrated that NEC is characterized by an imbalance in T-cell populations, including reduced regulatory T-cell activity and altered CD3+ T lymphocyte responses, contributing to impaired immune homeostasis [6,7]. This immune dysfunction is particularly pronounced in premature neonates due to incomplete maturation of adaptive immunity. During early neonatal life, mesenteric lymph nodes are structurally immature, with underdeveloped cortical and paracortical zones responsible for T-cell activation and immune coordination. This immaturity results in reduced CD3+ T-cell activity and weakened adaptive immune responses [7,8].In response to T-cell deficiency, compensatory activation of B-cell compartments and germinal center formation may occur; however, this response is often insufficient to control inflammation in NEC [7,9]. In severe cases associated with systemic inflammatory response syndrome (SIRS), activated lymphocytes migrate toward inflamed intestinal tissue, leading to lymphoid depletion and secondary immunodeficiency [5,6].Age-dependent maturation of mesenteric lymph nodes has been observed during the late neonatal period, characterized by improved structural organization and increased CD3 expression, indicating partial restoration of T-cell–mediated immunity [8,12].Purpose of the studyTo investigate the pathomorphological and immunohistochemical changes associated with immune organ disintegration in necrotizing enterocolitis in infants under one year of age.
2. Materials and Methods
- The study was based on archival materials obtained between 2015 and 2026 from the Andijan City Children’s Multidisciplinary Clinical Hospital and the Fergana regional Pathoanatomical bureau. A total of 200 archival biopsy samples were analyzed.In these biopsy specimens, immunohistochemical expression of the CD3 marker, a protein associated with the surface co-receptor of T-lymphocytes, was evaluated in mesenteric lymph nodes.
3. Results and Discussion
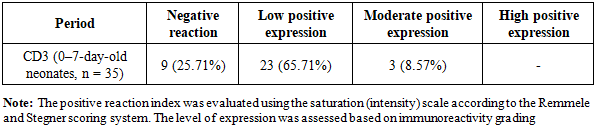
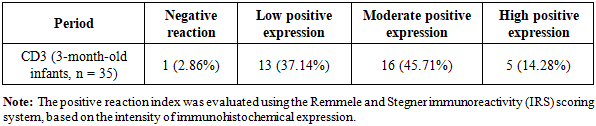
- The pathomorphological features of mesenteric lymph nodes in necrotizing enterocolitis (NEC) in neonates demonstrated a distinct pattern of development during the neonatal period, with clear differences between the early neonatal period (0–7 days) and the late neonatal period (8–28 days). These changes were closely associated with gestational maturity, including both term and preterm birth, and reflected the predominance of systemic vascular inflammatory responses in NEC.During the early neonatal period, morphologically immature mesenteric lymph nodes exhibited structural underdevelopment, which was accompanied by functional insufficiency of the cortical and paracortical zones representing the main immunologically active areas.In deceased neonates aged 0-7 days with NEC, a marked reduction of lymphocytes was observed in both the cortical and medullary regions of lymph nodes. This included a significant decrease in B-lymphocyte populations within lymphoid follicles, reduction in follicular size, and absence of germinal centers. In the paracortical zones, a decreased number of T-lymphocytes, particularly CD3 receptor–positive cells, was also identified.The CD3 marker is a surface co-receptor protein of T-lymphocytes that plays a key role in antigen-presenting cell interaction and initiation of primary immune responses. It is characterized by a strong positive expression in response to infectious stimuli and is considered a key indicator of cellular immune activation. The observed findings confirm a deficiency of CD3+ T-lymphocytes in mucosa-associated lymphoid tissue (MALT) structures and mesenteric lymph nodes in NEC (see Figure 1).
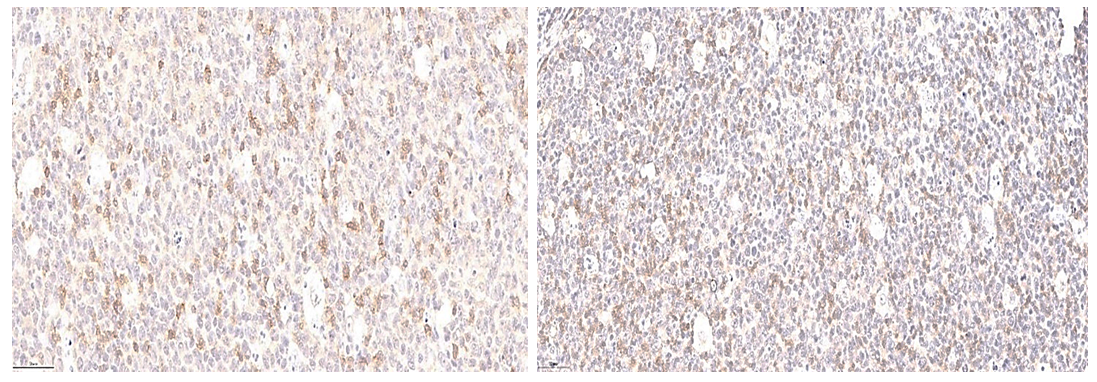 | Figure 1. Early neonatal period. 6-day-old neonate. Low positive expression of the CD3 marker. In the paracortical region, the intensity of CD3 immunostaining on the lymphocyte membranes was very weak. Cystic spaces were also observed, likely associated with apoptotic processes. Staining method: DAB chromogen. Magnification: 10 × 10 |
|
|
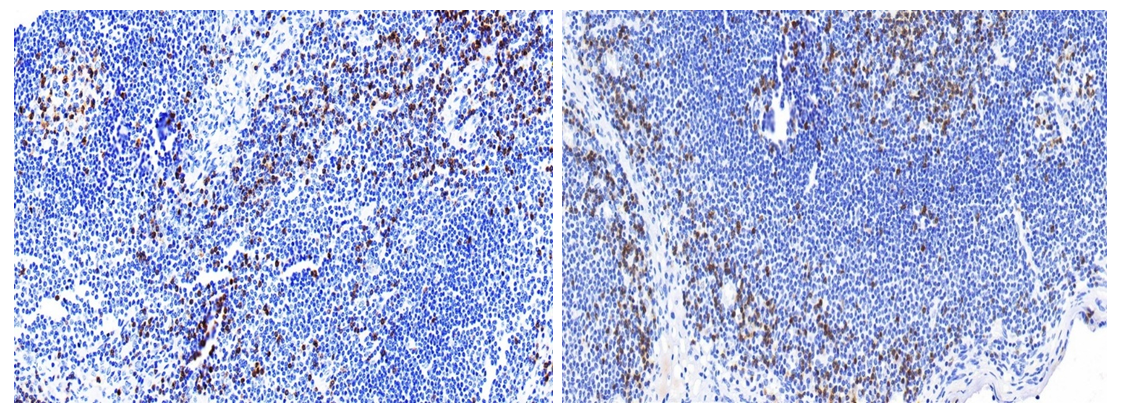 | Figure 2. Late neonatal period (18–25 days). Low positive expression of the CD3 marker. A small number of T lymphocytes were detected around lymphoid follicles. Staining method: DAB chromogen. Magnification: 4 × 10 |
|
4. Conclusions
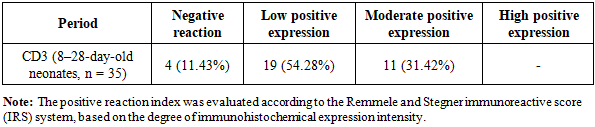
- In the early neonatal period (0–7 days), mesenteric lymph nodes (MLNs) were morphologically immature and incompletely developed. This structural and functional immaturity was identified as a key factor contributing to immune deficiency in the course of necrotizing enterocolitis (NEC).A pronounced T-lymphocyte deficiency was observed in 0–7-day-old neonates, characterized by a marked reduction in CD3+ T lymphocytes, with low expression detected in 65.71% of cases. This finding reflects a weakened specific immune response to antigenic stimulation.In age-related dynamics, by the late neonatal period (8–28 days), functional zones of mesenteric lymph nodes showed significant maturation, and CD3 marker expression increased approximately 3.33-fold compared with the early neonatal period. This indicates a gradual restoration and improvement of T-cell–mediated immune activity during postnatal development.