-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2384-2387
doi:10.5923/j.ajmms.20261605.31
Received: Apr. 8, 2026; Accepted: May 3, 2026; Published: May 15, 2026

The Role of Therapeutic Plasmapheresis in the Multimodal Management of Diffuse Peritonitis Complicated by Sepsis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSh. N. Khasanov1, N. K. Ibragimov2
1Assistant, Department of Anesthesiology, Resuscitation and Emergency Medical Care, Andijan State Medical Institute, Andijan, Uzbekistan
2Head of the Department of Anesthesiology and Resuscitation, Tashkent Medical University, Tashkent, Uzbekistan
Correspondence to: Sh. N. Khasanov, Assistant, Department of Anesthesiology, Resuscitation and Emergency Medical Care, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Acute diffuse peritonitis remains a significant clinical challenge with persistently high global mortality, especially when complicated by sepsis and multi-organ failure. This study aims to evaluate the impact of therapeutic plasmapheresis (TP) on hemodynamics, oxygen transport, and endotoxemia in the multimodal management of these patients. Methods: A prospective analysis was conducted on 85 patients (59 men, 26 women; age 18-75 years) with diffuse purulent peritonitis (toxic stage, n=56; terminal stage, n=29) treated between 2022 and 2026. All underwent source control surgery and intensive care. Parameters assessed included circulating blood volume (CBV), central hemodynamics (via impedance cardiography), serum middle-mass molecules (MMM), and oxygen transport (TO₂). The effects of different plasma replacement solutions during TP were compared. Results: Two distinct postoperative hemodynamic patterns were identified: hyperdynamic (n=57) and hypodynamic (n=28). Hypodynamic circulation was associated with significantly lower stroke volume index (SVI: 25.1±0.82 vs. 45.6±1.5 ml/m², p<0.001) and cardiac index (CI: 2.13±0.07 vs. 4.56±0.15 L/min/m², p<0.001), and higher MMM levels (470.5±16.0 mg/mL in severe cases). MMM concentration showed a strong inverse correlation with SVI, CI, and TO₂. Plasma replacement with crystalloids alone worsened hypovolemia and cardiac performance. In contrast, using hydroxyethyl starch (HES) or albumin significantly improved volemia, stroke volume, and TO₂ (p<0.05). For hyperdynamic circulation, a 1:1.5 replacement-to-exsanguinated plasma ratio was optimal, while a 1:1 ratio was recommended for hypodynamic circulation. Conclusions: High endotoxemia in diffuse peritonitis necessitates the inclusion of TP. However, the choice of plasma replacement solution is critical. Crystalloid-only replacement is suboptimal, while HES, albumin, or combined solutions provide superior hemodynamic support and detoxification efficacy.
Keywords: Abdominal Sepsis, Diffuse Peritonitis, Hemodynamics, Middle-Mass Molecules, Oxygen Transport, Plasmapheresis
Cite this paper: Sh. N. Khasanov, N. K. Ibragimov, The Role of Therapeutic Plasmapheresis in the Multimodal Management of Diffuse Peritonitis Complicated by Sepsis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2384-2387. doi: 10.5923/j.ajmms.20261605.31.
Article Outline
1. Introduction
- Acute generalized peritonitis remains a formidable challenge for clinicians, particularly surgeons. Despite advances in diagnostics and treatment, global mortality rates range from 4.5% to 58%, increasing to 70% when complicated by sepsis, septic shock, or multiple organ failure [1-3]. A critical driver of poor outcomes is severe endogenous intoxication (EI), caused by microbial influx, release of biologically active substances from necrotic tissues, and subsequent microcirculatory disturbances leading to vital organ dysfunction [4].Therapeutic plasmapheresis (TP) is an advanced method for managing endogenous intoxication syndrome (EIS). It allows for the removal of pathological proteins and immune complexes while replenishing deficient blood components [5]. However, information remains scarce on how different TP techniques and plasma replacement solutions affect circulatory parameters, blood volume, oxygen transport, and serum levels of medium-mass molecules (MMM) in peritonitis patients. Timely detection and correction of these disturbances are crucial for improving outcomes. This study aims to improve short-term treatment outcomes in patients with generalized secondary peritonitis by identifying optimal surgical and perioperative strategies, with a focus on the role of TP.
2. Materials and Methods
2.1. Study Design and Patients
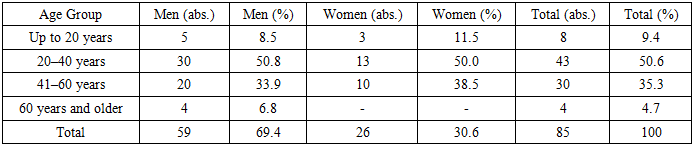
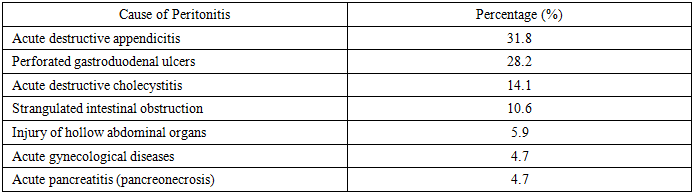
- From 2022 to 2026, 85 patients with diffuse purulent peritonitis in the toxic (n=56) or terminal (n=29) stages were treated at the Clinic of Surgical Diseases and the Intensive Care Unit of the Andijan State Medical Institute (AGMI). The cohort included 59 men (69.4%) and 26 women (30.6%), aged 18 to 75 years (Table 1). The leading causes were acute destructive appendicitis (31.8%), perforated gastroduodenal ulcers (28.2%), and acute destructive cholecystitis (14.1%) (Table 2). Patient severity was assessed using the B.D. Savchuk (1979) classification, APACHE II, SAPS, SOFA, and MODS scales.
|
|
2.2. Surgical and Intensive Care Protocol
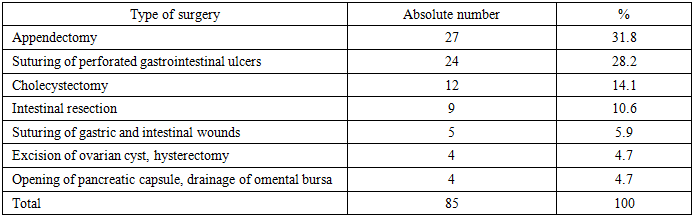
- All patients underwent short-term preoperative correction of water-electrolyte and acid-base balance. Surgical intervention via midline laparotomy under general endotracheal anesthesia aimed to eliminate the source of peritonitis (Table 3). The comprehensive treatment protocol included:Source control and peritoneal lavage with 8-10 L of antiseptic solution.Intraoperative decompression and transnasal intubation of the small intestine using a modified double-lumen silicone enteral tube.Postoperative peritoneal dialysis and continued intestinal lavage.In severe cases, prolonged intra-arterial catheter therapy via the superior mesenteric artery.
|
2.3. Assessment of Endogenous Intoxication and Hemodynamics
- Endogenous intoxication was assessed via leukocytosis, leukocyte intoxication index (LII), and serum MMM concentration using gel chromatography on Sephadex G-25 columns (normal: 0.245±0.04 µg/mL, n=50 donors). Circulating blood volume (CBV) and components were measured using the plasma-hematocrit method with Evans Blue dye [6]. Central hemodynamics (stroke volume [SV], cardiac output [CO], stroke index [SI], cardiac index [CI]) were evaluated via impedance cardiography using a UM-300 monitor (UTAS). Systemic vascular resistance (SVR) was calculated using standard formulas. Oxygen transport (TO₂) was calculated as: TO₂ = (Hb × 1.34 × HbO₂ + 0.0031 × PaO₂) × CI.
2.4. Statistical Analysis
- Data were processed using variation statistics on Microsoft Excel. Results are presented as mean ± standard error (M ± m). Differences between means were assessed using Student's t-test, with p < 0.05 considered statistically significant.
3. Results
3.1. Postoperative Hemodynamic Patterns
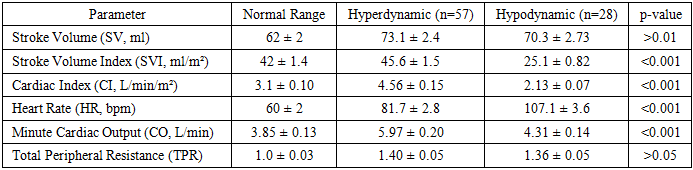
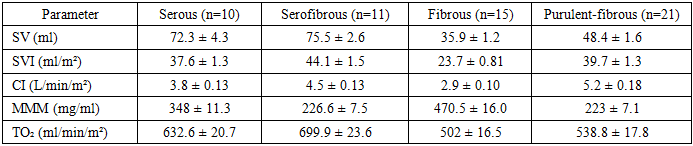
- On the first postoperative day, despite source control, patients remained critically ill with significant endotoxemia (mean MMM 470.5±16.0 mg/mL in severe cases), hypovolemia (CBV 59.2±1.8 mL/kg), and dysproteinemia (protein 56.2±1.2 g/L). Two distinct hemodynamic patterns were observed:Hyperdynamic circulation (n=57): Characterized by elevated CI and CO, associated with reactive/toxic phase peritonitis.Hypodynamic circulation (n=28): Characterized by significantly reduced SVI and CI (p<0.001), higher MMM levels, and reduced TO₂. This pattern was associated with terminal phase, fecal peritonitis, and higher mortality risk (Table 4).
|
|
3.2. Impact of Plasmapheresis and Plasma Replacement
- Plasma replacement using only crystalloids, while reducing MMM, led to worsened hypovolemia, decreased cardiac performance, and increased SVR. In contrast, replacement with hydroxyethyl starch (HES) or albumin significantly improved SV, CI, and CBV (p<0.05). Albumin also preserved plasma protein levels and improved the albumin/globulin ratio. Mixed replacement solutions (crystalloids + HES + albumin) showed similar benefits. The optimal replacement volume was 1:1.5 (replacement: exsanguinated plasma) for hyperdynamic circulation and 1:1 for hypodynamic circulation.
4. Discussion
- This study confirms that severe endogenous intoxication is a primary driver of postoperative hemodynamic compromise and reduced oxygen transport in patients with diffuse peritonitis. The identification of two distinct hemodynamic patterns—hyperdynamic and hypodynamic—aligns with the known pathophysiology of sepsis, where an initial hyperdynamic state can decompensate into a hypodynamic state associated with poor outcomes [7].Our data demonstrate a clear, inverse correlation between serum MMM concentration and key cardiovascular parameters (SVI, CI) and oxygen delivery (TO₂). This supports the central role of medium-mass molecules as markers of endotoxemia and direct contributors to myocardial depression and vasoplegia in this setting [4,8]. The high MMM levels observed in patients with fecal, fibrous, and pancreatogenic peritonitis correlate with the most severe clinical courses.The most critical finding of this study relates to the management of therapeutic plasmapheresis. While TP is effective at removing MMM, our results show that the choice of plasma replacement fluid is not neutral. Crystalloid-only replacement, though commonly used, exacerbated hypovolemia and impaired cardiac function, likely due to rapid redistribution out of the intravascular space [9]. In contrast, colloid-based replacement using HES or albumin provided superior intravascular volume expansion, improved stroke volume and cardiac output, and was associated with better oxygen transport parameters. This is consistent with the physiological principle that adequate preload is essential for maintaining stroke volume, particularly in a vasodilated, hypovolemic septic patient [10]. The finding that mixed solutions are also effective offers practical flexibility.Based on these results, we propose a physiology-guided approach to TP: the replacement ratio should be tailored to the patient's hemodynamic state (1:1.5 for hyperdynamic, 1:1 for hypodynamic). This personalized strategy aims to avoid fluid overload in patients who may not need it while ensuring adequate volume support in those with cardiac depression.Limitations: This is a single-center study with a moderate sample size. Long-term outcomes and survival data were not the primary focus. Further randomized controlled trials are needed to compare specific replacement fluids directly.
5. Conclusions
- High levels of endogenous intoxication in diffuse purulent peritonitis necessitate the inclusion of modern detoxification methods like therapeutic plasmapheresis in comprehensive treatment.Plasma replacement using only crystalloid solutions is not recommended due to the associated worsening of hypoproteinemia, hypovolemia, and cardiac performance.The optimal plasma replacement media during plasmapheresis are hydroxyethyl starch (HES), albumin, or combined solutions. The replacement volume should be guided by the patient's hemodynamic pattern (1:1.5 for hyperdynamic, 1:1 for hypodynamic circulation) and administered under central venous pressure monitoring.
ACKNOWLEDGEMENTS
- The authors wish to thank the medical and nursing staff of the Intensive Care Unit at Andijan State Medical Institute for their dedicated patient care.
Conflict of Interest and Funding
- The authors declare no conflict of interest. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.