-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2378-2383
doi:10.5923/j.ajmms.20261605.30
Received: Apr. 8, 2026; Accepted: Apr. 29, 2026; Published: May 15, 2026

Association of Maternal Iron Status with Labor Induction Outcomes and Neonatal Adaptation: A Prospective Cohort Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDilnoza Q. Salokhova, Dilchekhra Y. Yuldasheva
Department of Obstetrics and Gynecology, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Dilnoza Q. Salokhova, Department of Obstetrics and Gynecology, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective. To evaluate the association between maternal iron status and labor induction outcomes, obstetric complications, and early neonatal outcomes. Methods. This prospective cohort study included 225 pregnant women undergoing labor induction between May 2023 and June 2025 at a tertiary obstetric care center. Participants were stratified by gestational age (37-41 weeks and ≥41 weeks) and further subdivided according to serum ferritin and hemoglobin levels into normal iron status, latent iron deficiency, and manifest iron deficiency anemia. A comparison group of 40 women with spontaneous labor and normal ferritin levels was included. Induction efficacy, mode of delivery, intrapartum and postpartum complications, and neonatal outcomes (Apgar score and NICU admission) were analyzed using χ² tests and ANOVA/Kruskal-Wallis tests as appropriate. Results. Reduced serum ferritin levels (<30 ng/mL) were significantly associated with lower labor induction efficiency, prolonged induction-to-delivery interval, and increased resistance to prostaglandin-based induction methods (p < 0.05). Vaginal delivery rates decreased progressively with worsening iron deficiency, while cesarean section rates due to failed induction increased, reaching 32.5% at 37-41 weeks and 42.8% in post-term pregnancies among women with manifest anemia (p < 0.05). Iron-deficient women demonstrated higher rates of uterine inertia, atonic postpartum hemorrhage, and postpartum anemia. Neonatal outcomes were adversely affected by maternal iron deficiency, with lower Apgar scores and higher NICU admission rates observed exclusively among newborns of women with manifest iron deficiency. Conclusion. Maternal iron deficiency, including latent iron deficiency with normal hemoglobin, is associated with poorer labor induction outcomes, increased obstetric complications, and impaired early neonatal adaptation. Routine assessment of serum ferritin prior to labor induction may improve risk stratification, optimize clinical decision-making, and enhance maternal and neonatal outcomes.
Keywords: Labor induction, Iron deficiency, Serum ferritin, Pregnancy outcomes, Uterine contractility, Neonatal outcomes
Cite this paper: Dilnoza Q. Salokhova, Dilchekhra Y. Yuldasheva, Association of Maternal Iron Status with Labor Induction Outcomes and Neonatal Adaptation: A Prospective Cohort Study, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2378-2383. doi: 10.5923/j.ajmms.20261605.30.
1. Introduction
- The increasing use of labor induction (LI) has become a key issue in modern obstetrics because it directly affects maternal and perinatal outcomes. The World Health Organization reports that induced deliveries account for ~9.6% of births globally and may reach up to 25% of term births in high-income countries, reflecting a growing reliance on planned delivery in complicated pregnancies [1,3,5]. However, LI effectiveness remains variable and depends on cervical readiness, uterine contractility, hormonal factors, and maternal metabolic status [2,4,9]. Iron deficiency is one of the most common nutritional disorders in women of reproductive age and is increasingly linked to LI outcomes. UNICEF (2023) estimates that ~40% of women of childbearing age have iron deficiency and ~20% have anemia; in pregnancy, iron deficiency anemia may reach 40-50% (WHO) [3]. Evidence suggests that anemia and even latent iron deficiency (low ferritin with normal hemoglobin) are associated with induction failure, prolonged labor, and higher operative delivery rates. Low serum ferritin indicates depleted iron stores and may reflect impaired myometrial energy metabolism and reduced responsiveness to prostaglandins and oxytocin, increasing risks of labor dystocia, uterine atony, and postpartum hemorrhage, with potentially unfavorable neonatal outcomes [6,8,10]. Despite these concerns, there is no unified international standard for incorporating ferritin into LI planning. Integrating biochemical biomarkers into individualized induction strategies may improve risk stratification, optimize management, and enhance maternal-neonatal outcomes.
2. Materials and Methods
- The study protocol was approved by the Local Ethics Committee, and the study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.This study was conducted from May 2023 to June 2025 at a tertiary obstetric care center. Pregnant women aged 19-42 years with medical indications for labor induction were enrolled based on predefined clinical and laboratory criteria. Participants were stratified according to gestational age into two main groups. The first group included women at 37-41 weeks of gestation undergoing planned labor induction, while the second group consisted of women at ≥41 weeks of gestation undergoing post-term induction. Each main group was further subdivided based on serum ferritin and hemoglobin (Hb) levels into three subgroups:(a) women with normal iron status (serum ferritin >30 ng/mL and Hb ≥110 g/L; n=40);(b) women with latent iron deficiency (serum ferritin <30 ng/mL and Hb ≥110 g/L; n=40);(c) women with manifest iron deficiency anemia (serum ferritin <30 ng/mL and Hb <110 g/L; n=40).Women in the ≥41-week group were similarly subdivided according to ferritin and hemoglobin levels, with 35 participants in each subgroup. A control group of 40 pregnant women with normal ferritin levels and spontaneous onset of labor was also included. Diagnostic assessment comprised obstetric and gynecological history, clinical examination, laboratory investigations, and ultrasound evaluation. During labor induction, all participants underwent comprehensive clinical and laboratory monitoring. Induction efficacy was assessed by labor progression parameters, mode of delivery, and intrapartum complications, while neonatal outcomes were evaluated using standard clinical indicators, including Apgar scores.Statistical analysis was performed using SPSS software (version 26.0). Normality was assessed using the Shapiro-Wilk test. A p-value < 0.05 was considered statistically significant. Categorical variables were compared using the χ² test (Fisher’s exact test when appropriate); continuous variables were analyzed using ANOVA (Kruskal-Wallis for non-normal data).
3. Results
- Overall, 225 women undergoing labor induction and 40 women with spontaneous labor were analyzed. The groups were comparable in baseline characteristics.Indications for labor inductionHypertensive disorders were the leading indication for labor induction at 37-41 weeks of gestation, accounting for 47.5%, 55.0%, and 60.0% of cases in groups 1A, 1B, and 1C, respectively. In contrast, post-term pregnancy was the predominant indication at ≥41 weeks, observed in 77.1% of group 2A, 88.6% of group 2B, and 71.4% of group 2C. Fetal macrosomia was more frequent in post-term pregnancies, particularly among women with iron deficiency. Indications for labor induction differed significantly according to gestational age and iron status (χ² test, p < 0.05) (Table 1).
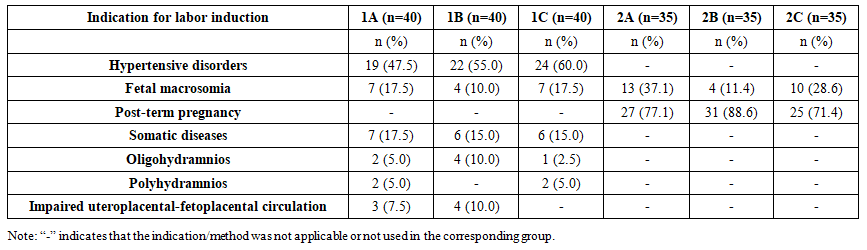 | Table 1. Indications for labor induction across study groups |
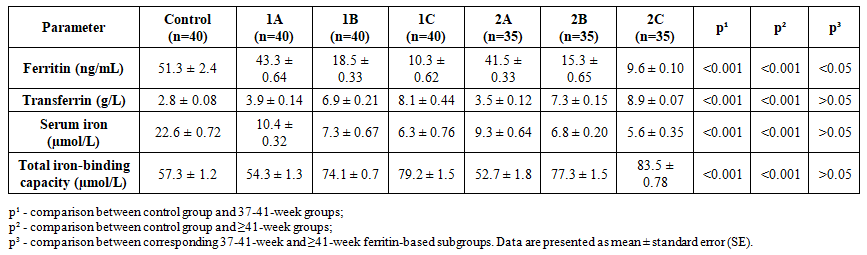 | Table 2. Iron metabolism parameters in pregnant women undergoing labor induction |
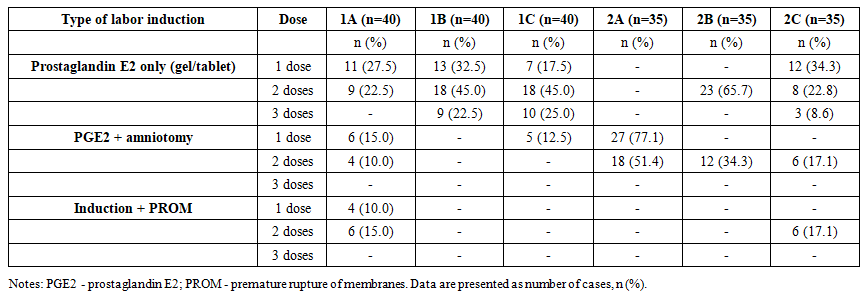 | Table 3. Types of labor induction used in the studied groups |
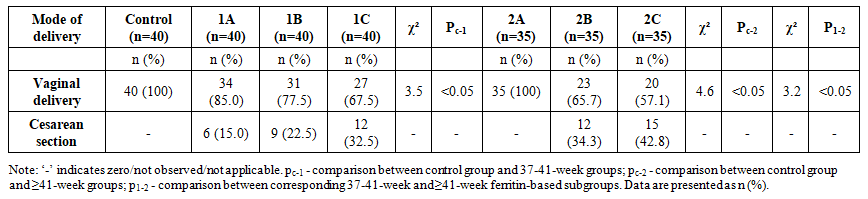 | Table 4. Mode of delivery in women undergoing labor induction |
 | Table 5. Main indications for cesarean section in women undergoing labor induction |
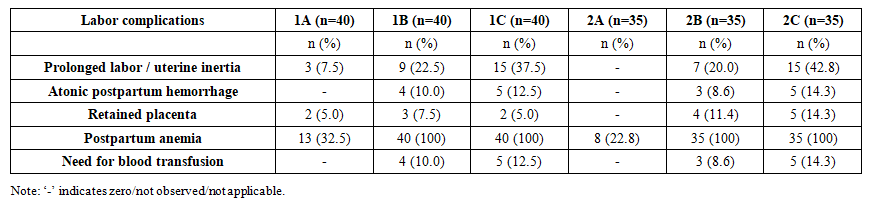 | Table 6. Labor complications in women undergoing labor induction |
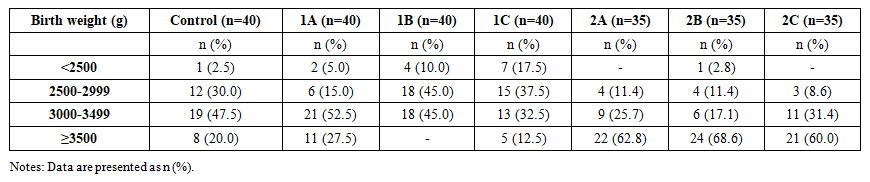 | Table 7. Birth weight of newborns in the studied groups |
 | Table 8. Neonatal outcomes assessed by Apgar score |
 | Table 9. Proportion of newborns transferred to the neonatal intensive care unit (NICU) |
4. Discussion
- Labor induction outcomes were closely associated with maternal iron status. Progressive iron deficiency was linked to higher rates of induction-related complications, particularly prolonged labor, uterine inertia, postpartum hemorrhage, and operative delivery, with more pronounced effects in post-term pregnancies and women with manifest anemia. Lower ferritin levels were consistently associated with poorer neonatal outcomes, including reduced Apgar scores, lower birth weight, and increased NICU admission. Importantly, even latent iron deficiency was associated with less favorable outcomes compared with normal iron status. These findings underscore the clinical relevance of ferritin assessment and support the incorporation of iron status evaluation into pre-induction risk stratification to improve maternal and neonatal outcomes.
5. Conclusions
- This study confirms that labor induction outcomes are closely related to maternal iron status. Reduced ferritin levels were associated with increased induction-related complications and poorer neonatal outcomes, including lower Apgar scores, reduced birth weight, and higher NICU admission rates. Even latent iron deficiency was linked to less favorable outcomes compared with normal iron status. These findings identify ferritin as a clinically relevant biomarker for pre-induction risk assessment. Incorporating iron status evaluation into labor induction planning may improve maternal and neonatal outcomes and enhance obstetric safety.