-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2373-2377
doi:10.5923/j.ajmms.20261605.29
Received: Apr. 6, 2026; Accepted: Apr. 29, 2026; Published: May 15, 2026

Pathomorphological Changes in the Thymus in Neonatal Necrotizing Enterocolitis in Newborn Infants
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLD. K. Chartakov1, A. N. Don2, M. A. Mamatalieva1
1Andijan State Medical Institute, Uzbekistan
2Tashkent State Medical University, Uzbekistan
Correspondence to: D. K. Chartakov, Andijan State Medical Institute, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The present study investigated the pathomorphological and morphometric features of immune organ disintegration in the thymus of newborn infants with necrotizing enterocolitis during the neonatal period, and developed a diagnostic algorithm. It was established that, in the early neonatal period, the thymus—being an incompletely developed gland—was unable to fully perform its functional activity. This was characterized by a marked decrease in various lymphocyte populations, induced apoptosis, and a compensatory proliferation of different mesenchymal cells. In addition, a reduction of the cortical layer and the loss of clear corticomedullary boundaries were observed. The thymic lobules were reduced in size compared to normal, with a significant decrease in the number of thymocytes or small lymphocytes within the cortical region of the parenchyma. Proliferative active foci were absent, while reticuloepithelial cells exhibited shortened and thickened processes, and multiple accumulations of reticulocytes were identified along the periphery. A pronounced deficiency and depletion of immune cells in the cortical layer were also noted. Between days 8 and 28, signs of thymic maturation were observed. In response to various infectious conditions, massive hyperplastic foci of small lymphocytes appeared in the cortical region. Enlarged nurse cells and dendritic epithelial cells of varying localization were detected, along with an increased number of lymphocytes surrounding their processes.
Keywords: Newborn, Neonatal period, Necrotizing enterocolitis, Pathomorphological changes
Cite this paper: D. K. Chartakov, A. N. Don, M. A. Mamatalieva, Pathomorphological Changes in the Thymus in Neonatal Necrotizing Enterocolitis in Newborn Infants, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2373-2377. doi: 10.5923/j.ajmms.20261605.29.
1. Introduction
- Necrotizing enterocolitis [NEC] is one of the most severe and life-threatening conditions among newborn infants, particularly in preterm neonates. Its pathogenesis involves ischemic injury of the intestinal wall, dysbiosis of the microbiota, and immaturity of the immune system. Therefore, NEC remains one of the most pressing challenges in modern neonatology [1,2].During the neonatal period, the thymus, as a central organ of the immune system, plays a crucial role in determining the newborn’s immune response to infections. Structural and functional alterations in the thymus, particularly disturbances in T-lymphocyte differentiation and proliferation, lead to impaired immune responses and an increased risk of infectious complications [3,4].Recent studies have demonstrated that, in addition to local intestinal damage, systemic immune dysfunction plays a significant role in the development of NEC. In particular, atrophic and degenerative changes in the thymus, lymphocyte depletion, and enhanced apoptosis contribute to the severity of the disease [5,6].Furthermore, morphometric assessment of pathomorphological changes in the thymus provides an opportunity to evaluate the degree of immune deficiency during the neonatal period and to predict disease outcomes. This approach is of great importance for early diagnosis and the development of individualized therapeutic strategies [7,8].Currently, thymic structural and functional alterations in NEC remain insufficiently studied, and there is a limited number of pathomorphological and morphometric investigations in this field. In particular, the assessment of dynamic changes in the thymus across different stages of the neonatal period remains a highly relevant issue [9,10].Therefore, comprehensive investigation of pathomorphological changes in the thymus in newborns with necrotizing enterocolitis, determination of their relationship with the immune system status, and development of a diagnostic algorithm represent important tasks of contemporary medical science [11,14].Purpose of the studyTo investigate the pathomorphological and morphometric features of immune organ disintegration in the thymus in newborn infants aged 0-28 days with necrotizing enterocolitis, and to develop a diagnostic algorithm.
2. Materials and Methods
- The study materials were obtained from archival records of Andijan Regional Multidisciplinary Pediatric Clinical Hospital and Fergana Regional Pathological Bureau for the period of 2015-2026. The analyzed data included patients’ medical histories, autopsy reports, and biopsy materials.A total of 386 patient cases were included in the study, of which 186 were medical histories and 200 consisted of autopsy and biopsy materials. Pathomorphological changes in the intestinal wall and thymus were examined.Pathomorphological investigations were carried out using standard histological methods. Morphometric analysis was performed to assess structural changes in the thymus and intestinal tissues. The obtained results were comparatively analyzed and correlated with clinical data.
3. Results and Discussion
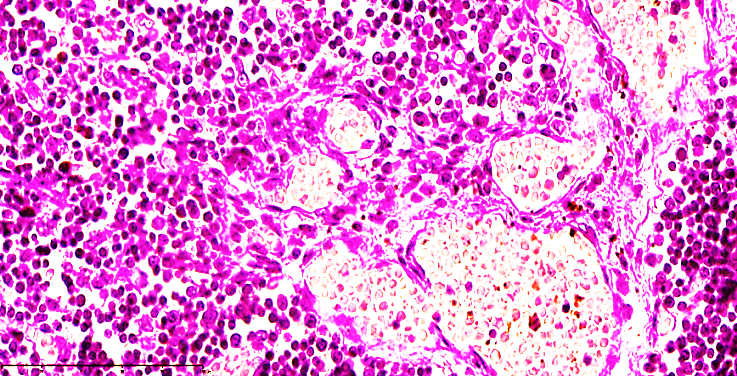
- In the early neonatal period, the thymus performing its functional responsibilities is highly sensitive to various stress factors, including glucocorticoid-associated immunosuppression. Microscopically, the thymus was surrounded by a fibrous capsule of uniform thickness, its sparse-fibered structures remained unchanged, and vascular integrity was preserved. Thymic lobules were reduced in size compared to normal. Within the parenchyma, there was a quantitative reduction of thymocytes and small lymphocytes in the cortical layer, absence of active proliferative foci, and reticuloepithelial cell processes appeared shortened and thickened, with multiple accumulations of reticulocytes observed along the periphery. A marked deficiency or depletion of immune cells in the cortical layer was identified.During days 0–7 of the early neonatal period, newborns who developed necrotizing enterocolitis, often in combination with pneumonia, sepsis, or septic shock, exhibited multi-organ dysfunction. Classical patterns of accidental thymic transformation were not consistently observed. Microscopically, the main morphological features included a reduction in thymocyte numbers, apoptosis of nurse (epithelial) cells, and an increase in reticulocytes within the processes of reticuloepithelial cells. Consequently, the ratio of stromal to mesenchymal tissue in the thymus was altered, mainly manifested as an increase in sparse-fibered connective tissue within the cortical layer.Small-caliber vessels demonstrated complete filling, erythrocytes exhibited sludging phenomena, and perivascular areas showed edema and plasmatic condensation within the stroma. These changes led to disruption of thymic histoarchitecture, marked depletion of young or small thymocytes around nurse cells, a quantitative reduction of lymphocytes in subcapsular regions and around reticuloepithelial cells, and an increase in dendritic cells, fibroblasts, and histiocytes. As a result, massive parenchymal depletion or stromal collapse in the cortical region of the thymus was observed.At the corticomedullary boundary, homogeneous, rounded Hassall’s bodies composed of epithelial whorls were identified. Normally, Hassall’s bodies are absent in corticomedullary areas (see Figure 1 and 2).
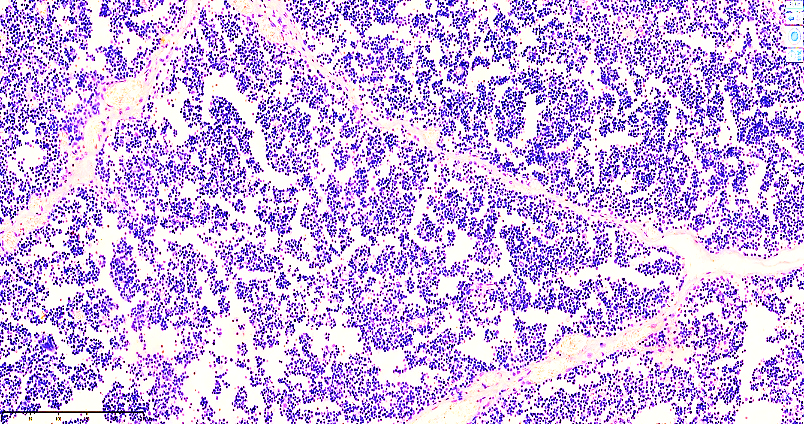 | Figure 1. Thymic tissue in the early neonatal period. Thymic tissue of a deceased patient, R., on day 3. The boundaries between the cortical and medullary regions are almost indistinguishable. Numerous spaces are observed. The stroma shows fibrillar structures at various stages of maturation. Most of the blood vessels appear fully filled. Staining: H&E. Magnification: 4×10 |
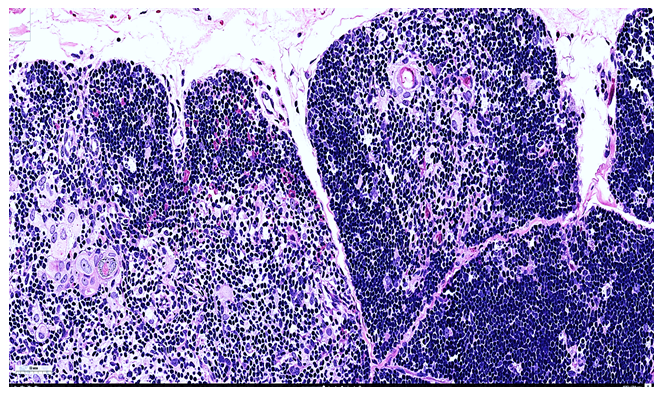 | Figure 2. Thymic tissue in the early neonatal period. Thymic tissue of a deceased patient, Y., on day 7. Focal hypercellularity is observed in the cortical region, and the postcapillary venules are fully filled. Large and elongated reticuloepithelial and nurse epithelial cells are visible. In the corticomedullary and medullary regions, Hassall’s bodies of varying sizes and degrees of maturation are identified. Most lymphoblasts and histiocytes are clearly seen, and in areas of sparse stroma, phagocytically active macrophages are present. Staining: H&E. Magnification: 10×10 |
|
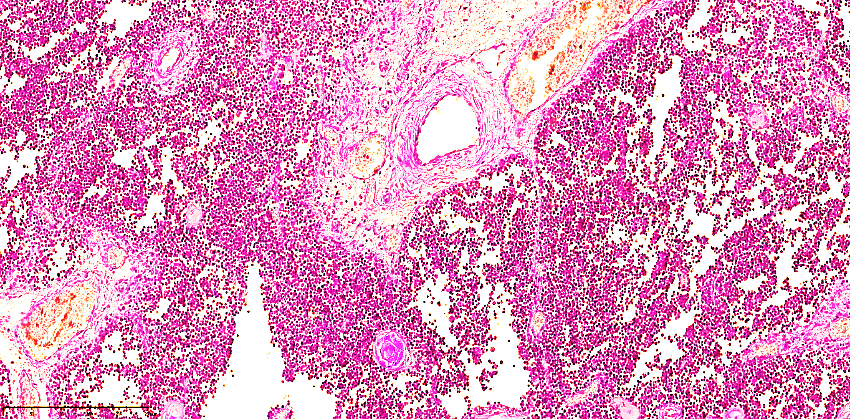 | Figure 3. Thymic Tissue in the Late Neonatal Period (Day 12). Thymic tissue at 12 days of the late neonatal period. Development of dense fibrous connective tissue is observed between the cortical and medullary layers. In the cortex, gaps are formed in areas where small lymphocytes undergo pronounced apoptosis. Hassall’s bodies at various stages of maturation are present in the central region. Staining: H&E. Magnification: 4×10 |
 | Figure 4. Thymic Tissue in the Late Neonatal Period (Day 18). Thymic tissue at 18 days of the late neonatal period. In the medullary layer, mature lymphocytes are localized in perivascular regions. The vessel walls are massively dilated, and vascular permeability is disrupted. Large mature lymphocytes with foci of apoptosis are observed. Staining: H&E. Magnification: 40×10 |
|
4. Conclusions
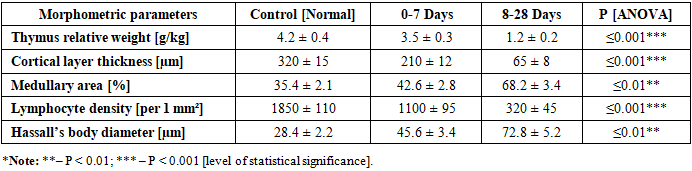
- The study demonstrates distinct patterns of accidental thymic transformation during both early and late neonatal periods in newborns with necrotizing enterocolitis (NEC). In the early neonatal period (0-7 days), the thymus is still morphologically immature, particularly in the cortical region, where there is a pronounced depletion of thymocytes. This depletion occurs simultaneously across both cortical and medullary layers, resulting in the near absence of mature thymocytes. These observations indicate that the thymus during this stage is highly vulnerable to stress and immune challenges, and its structural and functional capacity to support T-cell differentiation is significantly limited.In the late neonatal period (8-28 days), although the thymus shows more advanced maturation, functional disruptions are evident. Mature thymocytes form proliferatively active foci; however, these areas are interspersed with apoptotic gaps, reflecting ongoing cell death. In the medullary layer, mature lymphocytes accumulate around postcapillary venules, suggesting impaired lymphocyte egress into the peripheral circulation. These phenomena indicate that even in a structurally more mature thymus, NEC induces localized immunological stress, triggering apoptotic processes and stromal alterations that compromise the organ’s integrity.Overall, these findings highlight the critical impact of NEC on thymic structure and function across the neonatal period. The differential patterns of thymocyte depletion, apoptotic gap formation, and perivascular lymphocyte accumulation provide a morphofunctional basis for understanding the development of immunodeficiency in affected neonates. The results underscore the importance of early detection and monitoring of thymic changes, as these alterations may significantly influence systemic immune competence and the risk of secondary infections.