Rasulova Nasiba Shavkatovna
Assistant Professor, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Rasulova Nasiba Shavkatovna, Assistant Professor, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The treatment of patients with disorders of the vocal apparatus, as well as the prevention of functional impairments, is one of the pressing issues in modern otorhinolaryngology. According to various authors, the prevalence of this pathology ranges from 6% to 43%. The larynx is one of the most common sites for tumour-like formations, as well as benign and malignant neoplasms, characterised by significant morphological diversity. Among tumours of the ENT organs, laryngeal lesions rank first both in terms of absolute numbers of cases and in terms of proportion (50–70%). This is due to the fact that the larynx is more exposed to various exogenous and endogenous factors that contribute to the development of neoplastic processes. Such factors include occupational hazards, in particular chronic vocal strain, smoking, alcohol abuse, chronic inflammatory diseases, as well as endocrine and neurovegetative disorders. These pathogenetic factors primarily contribute to the development of benign neoplasms, which are significantly more common than malignant tumours. However, the potential danger of benign lesions lies in the fact that, in the absence of adequate prevention and timely treatment, some of them may progress to precancerous conditions with subsequent malignancy. Benign tumours and tumour-like lesions of the larynx, which constitute the most common group of diseases, are capable of causing significant functional impairments, leading to reduced working capacity, and, in the absence of timely treatment, often to a fatal outcome. It should be noted that benign laryngeal neoplasms are often accompanied by prolonged voice dysfunction. In individuals in vocal and speech-related professions, this can lead to permanent loss of professional capacity, extending to professional incapacity and disability, which underscores the high medical and social significance of this problem.
Keywords:
Benign laryngeal tumours, Vocal fold nodules, Vocal fold polyps, Vocal fold cysts
Cite this paper: Rasulova Nasiba Shavkatovna, The Diagnostic Significance of Morphological Methods in Tumour-Like Pathologies of the Larynx, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2363-2369. doi: 10.5923/j.ajmms.20261605.27.
1. Introduction
In the current clinical setting, a comprehensive examination of the patient is essential for a timely and accurate diagnosis [1,2,3,4,5].With the development of endoscopic microsurgery of the larynx and its active introduction into clinical practice, there has arisen a need for an objective assessment of the functional outcomes of voice restoration and external respiration [6,7,8].In recent decades, the method of acoustic voice analysis has become widely used. However, according to the literature, such studies are predominantly conducted in the immediate postoperative period, whereas ensuring objectivity requires an analysis of both immediate and long-term treatment outcomes [9,10].Currently, the patient’s subjective assessment of quality of life is regarded as one of the most important criteria for the effectiveness of medical care. In everyday clinical practice, patients are increasingly paying attention not only to the quality of the treatment provided, but also to their quality of life following medical interventions [11,12,13,14,15,16].Despite the achievements of modern otorhinolaryngology and phoniatrics, a number of issues concerning the diagnosis and treatment of tumour-like diseases of the larynx remain unresolved. To date, the mechanisms underlying the development of this pathology, its tendency to recur and its chronic course have not been sufficiently studied, which lends this problem significant medical and social importance [17,18,19,20,21,22].
2. Materials and Methods
To comprehensively assess the functional state of the vocal apparatus and to conduct a comparative analysis of indicators between different clinical groups, subjective (questionnaire-based) and objective (acoustic analysis) research methods were applied to patients with tumour-like diseases of the larynx (nodules, polyps and cysts of the vocal folds).A control group of healthy individuals (n=40) was formed for the comparative analysis.The study patients were divided into three groups:• Group 1 — patients with vocal fold nodules (n=22); • Group 2 — patients with vocal fold polyps (n=20); • Group 3 — patients with vocal fold cysts (n=18). The results were analysed according to standard diagnostic criteria.Patient R.B. Shavkatov, born in 1989, presented for a routine check-up. No complaints.In accordance with the examination protocol, laryngeal stroboscopy was performed: the vocal folds vibrated symmetrically, the closure line was smooth, the mucosal wave was free, and no pathological dilation of the vascular pattern was detected.To improve diagnostic accuracy, a minimal biopsy sample was taken during microlaryngoscopy and sent for histological examination.On the histological specimen (Fig. 1), the layers of the vocal fold mucosa have an ordered structure. The superficial layer consists of densely packed cells, with no signs of marked thickening or tears.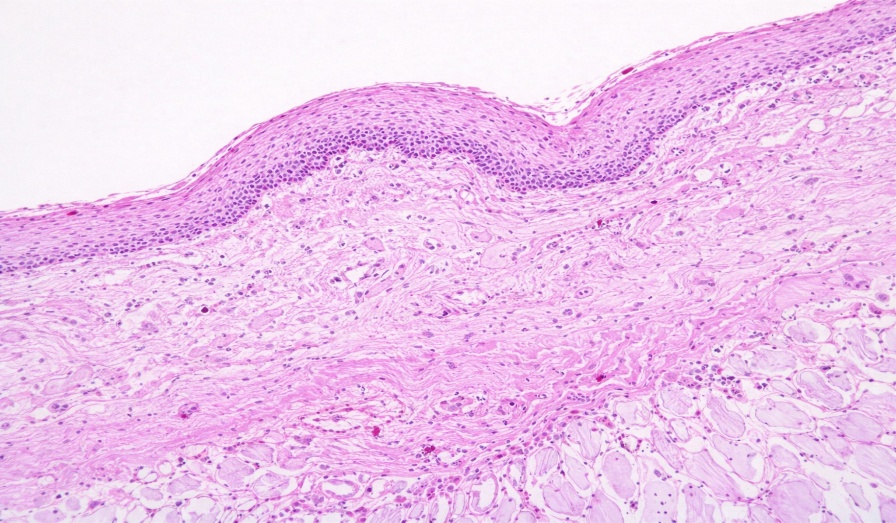 | Figure 1 |
In the underlying layer, the fibrous structure is uniform, with no signs of marked oedema or excessive fluid accumulation. The vascular network is normal, and no signs of inflammatory infiltration were detected.This morphological picture is characteristic of healthy individuals in the control group and indicates the preserved elasticity of the superficial (‘soft’) layer, which is necessary for full-fledged voice production.The figure presented is used as a benchmark for subsequent comparative analysis.In the present study, it was precisely this normal morphological structure that was adopted as the ‘reference standard’, allowing for the assessment of the nature and localisation of pathological changes in nodules, polyps and cysts of the vocal folds.The data obtained allowed us to establish a correlation between vibration abnormalities detected by stroboscopy (irregular closure, reduced amplitude of oscillations, hoarseness) and corresponding morphological changes in the tissues.A comprehensive approach, combining stroboscopy and histological examination, improves the accuracy of early diagnosis, avoids unnecessary drug therapy and enables the selection of the optimal treatment strategy.In the control group, the parameters of mucosal thickness, fibre density and vascular condition remained stable. This provides the ‘background’ necessary for differential diagnosis:• in nodules, thickening of the superficial layer and consolidation of the underlying fibrous tissue predominate; • in polyps, oedema and vascular changes predominate; • in cysts, a cavity with a capsule form. Thus, comparison with the normal morphological picture allows the diagnosis to be confirmed not only visually but also at the tissue level.From a practical point of view, stroboscopy reflects functional changes, whereas histology allows their morphological basis to be established. Their combination ensures the optimisation of the diagnostic process.Patient A.S. Ergashev, born in 1994, a teacher by profession. Over the past six months, he has complained of rapid vocal fatigue, hoarseness by the end of the working day, and episodes of his voice ‘breaking’ when speaking loudly.During the physical examination, laryngeal stroboscopy was performed: a moderate asymmetry in the vibrations of the vocal folds was identified; on closure, a small gap was noted in the central region, and the mucosal wave was reduced.During microlaryngoscopy, a targeted biopsy was taken from the suspicious area, followed by histological examination.The specimen presented (Fig. 2) shows thickening of the superficial layer of the vocal fold. In the epithelial layer, there is an increase in cell count and thickening of the layers; in some areas, the surface becomes irregular.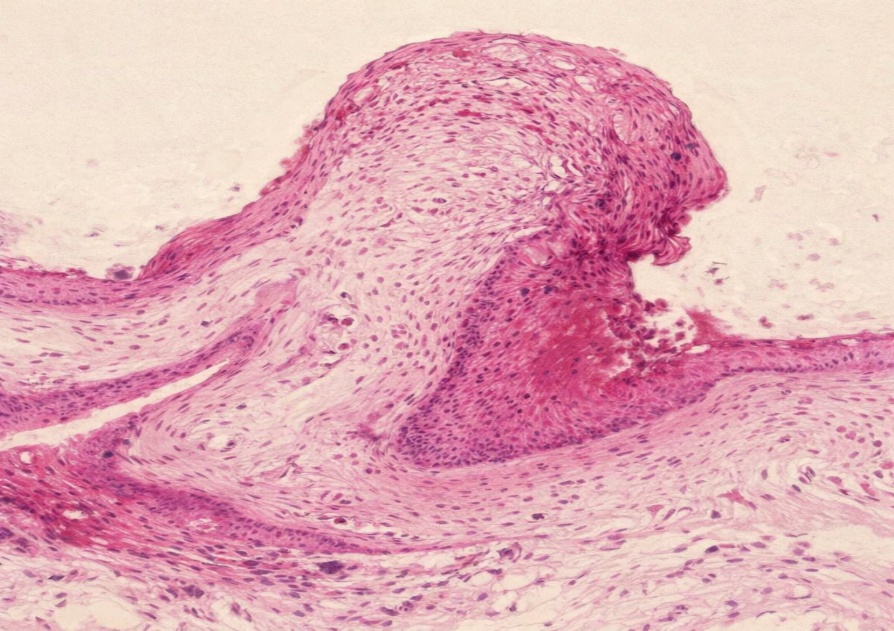 | Figure 2 |
In the underlying layer, compaction of fibrous tissue is detected, indicating the formation of areas of fibrosis (‘indurations’) that impede the free vibration of the vocal fold.A moderate accumulation of inflammatory cells is observed around the blood vessels, indicating long-standing mechanical irritation and microtrauma to the tissues.This morphological picture is characteristic of vocal fold nodules and is, as a rule, associated with chronic vocal strain.The study found that the main stroboscopic sign in patients in this group is incomplete closure of the vocal folds, which morphologically corresponds to thickening of the superficial layer and consolidation of the fibrous tissue.Thus, the clinical and morphological data complement one another.In contrast, in the case of polyps and cysts, the mechanisms of vibration disturbance are of a different nature:— in polyps, oedema and vascular changes predominate;— in cysts, there is a mechanical restriction of vibration due to the presence of a cavity.Consequently, the presented findings allow for the reliable confirmation of the diagnosis of a vocal fold nodule.The use of targeted biopsy followed by histological examination, in combination with stroboscopy, helps to optimise diagnosis, prevents unnecessary treatment and allows for the selection of an appropriate therapeutic approach (voice rest, phonopaedic exercises or microsurgical intervention).In the majority of patients in group 1 (n=22), similar changes were localised at the edges of both vocal folds, predominantly in the zone of maximum vibration.Clinically, this manifested as hoarseness, a narrowed vocal range, and rapid fatigue during prolonged speech.In the control group, no such morphological changes were detected, which is an important differential diagnostic feature.The practical significance of the data obtained lies in the need to assess not only the macroscopic picture but also the structure of the mucosal layers.Histological confirmation allows for individualised treatment:— where fibrosis predominates, surgical intervention may be required;— where inflammatory changes predominate, conservative therapy may be effective.The patient, Kodyrov J.N., born in 1978, is a professional singer (performing at formal events).The patient reports that following intensive vocal exertion, his voice becomes hoarse for several days, and he experiences difficulty in producing sound in the mornings. Stroboscopy revealed an asymmetry in the vibrations of the vocal folds; in the anterior regions, an uneven closure was observed, forming a characteristic ‘hourglass’ configuration. During microlaryngoscopy, a biopsy was performed, followed by histological examination.The specimen (Fig. 3) shows deformation of the vocal fold layers with their bending in the area of maximum stress. In this region, there is marked thickening of the superficial layer.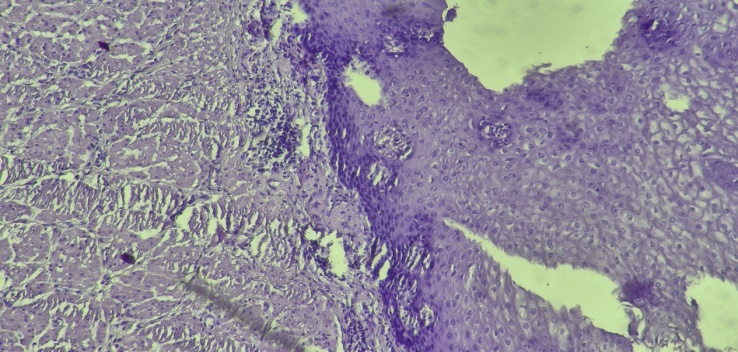 | Figure 3 |
In the underlying tissues, the order of the fibres is disrupted, with areas of thickening and disorganisation observed.In a number of areas, signs of microhaemorrhages and clusters of cellular elements around the vessels are identified, indicating chronic microtrauma.These changes reflect an adaptive-compensatory process: in response to constant mechanical stress, the tissue thickens, but its elasticity is reduced.During the study, three key interrelated features were identified in patients with nodules:1. a reduction in the amplitude of the mucosal wave during stroboscopy; 2. the presence of a central slit upon closure of the vocal folds; 3. thickening of the superficial layer and fibrosis of the underlying tissue on histological examination. The morphological picture presented confirms the aforementioned pathogenetic mechanism.In contrast to nodules:— in polyps, oedema and vascular changes predominate;— in cysts, the presence of a cavity is identified.Thus, Figure 3 is of significant importance for differential diagnosis.The combined use of stroboscopy and histology allows:— the diagnosis to be refined;— the treatment strategy to be determined;— an individual voice rehabilitation programme to be developed.In the majority of patients in this group, a link between the condition and occupational vocal strain (teachers, sales assistants, singers) has been identified.In contrast to the control group, where the tissue structure was homogeneous, signs of ‘mechanical adaptation’ are observed in this case.Early detection of such changes allows a positive outcome to be achieved without surgical intervention, whereas in advanced stages, longer-term treatment is required.The patient, L.U. Mamatova, born in 1983, works in the retail sector. She reports that approximately one month ago, following severe exposure to the cold and episodes of loud speech, she developed persistent hoarseness. Stroboscopy revealed a rounded mass at the edge of one vocal fold; vibration on this side was reduced, and the closure line was deviated. During microlaryngoscopy, a sample was taken from the area of the mass for histological examination.Figure 4 shows a rounded structure on the surface of the vocal fold. The interior of the lesion has a loose, oedematous structure, indicating a predominance of interstitial oedema (fluid accumulation). The blood vessels are dilated, and perivascular infiltration with cellular elements is noted in places. Unlike the nodule, the superficial layer has not undergone marked fibrotic thickening but covers the lesion, whilst the underlying oedematous layer impairs the free vibration of the vocal fold.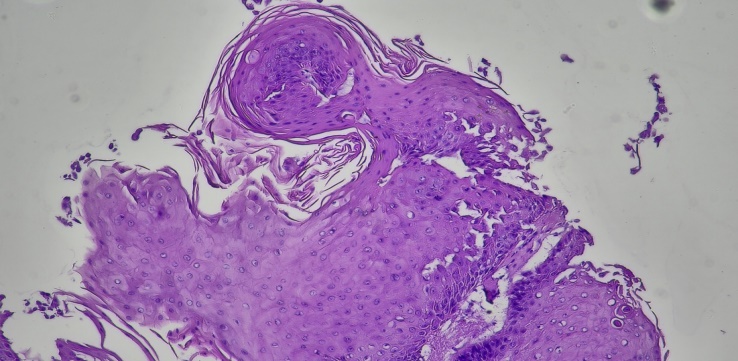 | Figure 4 |
This morphological picture is characteristic of a polyp, which is more commonly located on a single vocal fold and is associated with vocal strain and inflammatory factors. In the study of patients in group 2 (n=20), the following correlation was established: unilateral reduction in vibration and deviation of the closure line, as determined by stroboscopy, corresponded to histological features of oedema and vasodilation. In contrast, nodules are characterised by fibrous tissue thickening, whilst cysts are characterised by the presence of an intra-tissue cavity.Thus, Figure 4 allows a polyp to be distinguished from simple inflammatory oedema: in this case, the oedema is structured and localised. The combined use of stroboscopy and targeted biopsy followed by histological examination improves diagnostic accuracy and enables the selection of an appropriate treatment strategy — ranging from conservative measures to microsurgical intervention. This facilitates a more rapid recovery of vocal function and reduces the risk of recurrence.In the control group, such limited oedematous lesions were not detected, and the presence of a pronounced interstitial component was an important differential feature of a polyp. Clinically, the voice in such patients was characterised as ‘wet’, with a lowered pitch, and hoarseness increased with prolonged speech, which is associated with an increase in mass and a reduction in the vibratory capacity of the vocal fold. Furthermore, due to pronounced vascularisation, episodes of haemorrhage and sudden deterioration in voice quality are possible.Patient M.Z. Abdullaev, born in 1991, a long-distance lorry driver. He reports frequent night-time eating, heartburn and hoarseness in the morning. Over the last two months, his hoarseness has worsened. Stroboscopy revealed a large mass on one vocal fold, almost completely blocking the propagation of the mucosal wave and impairing closure.During microlaryngoscopy, a biopsy of the mass was performed, followed by histological analysis. Figure 5 shows the structure of the polyp, which occupies a significant area. Within the mass, loose, spongy tissue with marked fluid accumulation is observed. Areas of haemorrhage are visible in some sections. The vessels are dilated and their walls are thinned, increasing the risk of trauma.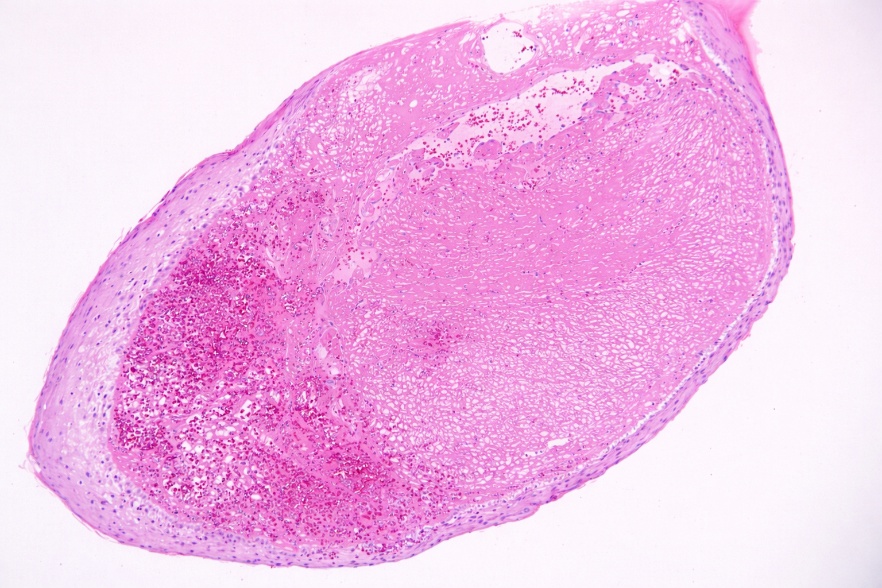 | Figure 5 |
The formation is covered by surface epithelium; however, the significant size of the polyp leads to deformation of the vocal fold and mechanical restriction of its vibration. The study found that an increase in the volume of the polyp is accompanied by a reduction in the amplitude of vibrations, a deviation of the closure line, and an increase in low-frequency hoarseness.Unlike nodules, which are characterised by bilateral fibrotic thickening, and cysts, which have a cavitary structure, polyps exhibit a pronounced oedematous-vascular component. Figure 5 highlights the need to assess not only the macroscopic appearance but also the internal structure of the lesion.Large polyps with marked vascularisation respond poorly to conservative therapy, which justifies the need for surgical treatment followed by voice rehabilitation. The combined use of stroboscopy and histology allows for the timely determination of indications for intervention.In the control group, there were no signs of marked oedema or vascular dilation. The presence of a ‘spongy’ structure is a reliable morphological marker of a polyp. It was also noted that gastro-oesophageal reflux may contribute to the progression of oedema and exacerbation of the clinical picture, which requires a comprehensive approach to treatment.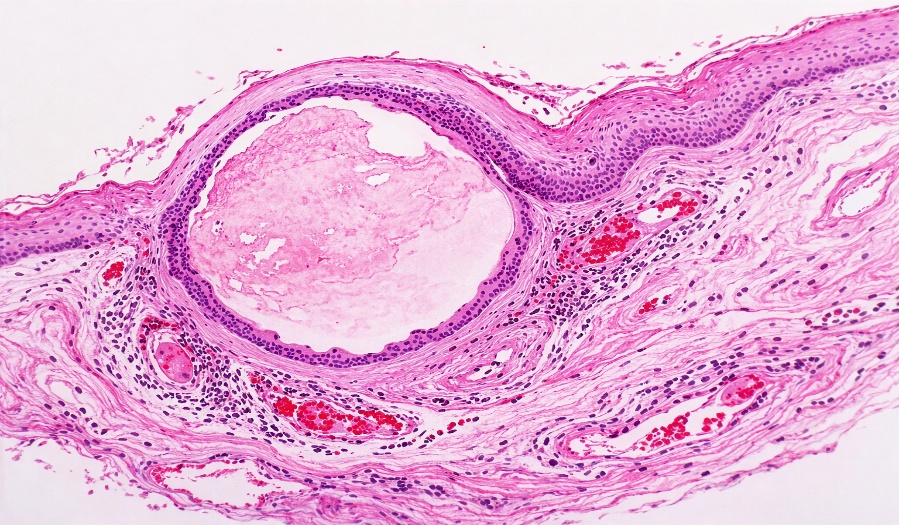 | Figure 6 |
Patient S.A. Tursunova, born in 1986, a bank clerk, had been experiencing hoarseness, a broken voice and a sensation of a foreign body in her throat for a year. Stroboscopy revealed a localised induration without a mucosal wave. Microlaryngoscopy with histological examination following incision of the suspicious area revealed a rounded intratissue cavity with a distinct wall. The inner surface was lined with an epithelioid layer containing a homogeneous dense substance.Compression of the surrounding tissue, inflammatory changes and vasodilation indicate the long-standing presence of the cyst and its chronic effect.The study confirmed the combination of stroboscopic features of the cyst (local rigidity, absence of mucosal wave) with morphological features (cavity and capsule), which distinguishes it from nodules and polyps.It is clinically significant that conservative treatment of cysts is ineffective due to the presence of a encapsulated cavity. Early diagnosis using microlaryngoscopy and histology allows for the optimisation of treatment and the determination of indications for surgical intervention. Differential diagnosis is important to rule out other volumetric lesions of the larynx. Vocal fold nodules usually occur bilaterally in the area of maximum contact between the folds and are histologically characterised by fibrosis and hyalinosis. Vocal fold polyps, as a rule, have more pronounced vascularisation and a loose structure.Thus, the present case demonstrates the importance of a comprehensive approach to the diagnosis of laryngeal diseases, incorporating both visual methods (stroboscopy, microlaryngoscopy) and histological examination. This allows not only for an accurate diagnosis but also for the determination of the optimal treatment strategy. In this case, given the ineffectiveness of conservative therapy, microsurgical removal of the cyst is the most appropriate course of action.Patient Sh.B. Nazarov, born in 1976, an office manager with a high vocal workload. He had been treated on several occasions for ‘laryngitis’, experiencing only temporary improvement. Stroboscopy revealed a large mass with a smooth surface, displacing the vocal fold and disrupting its vibration. During microlaryngoscopy, the mass was completely removed and subsequently examined histologically. Figure 7 shows a large cavity with a thick wall and epithelial lining. Inside, there is a homogeneous mass corresponding to an accumulation of secretions [23,24,25,26,27,28,29].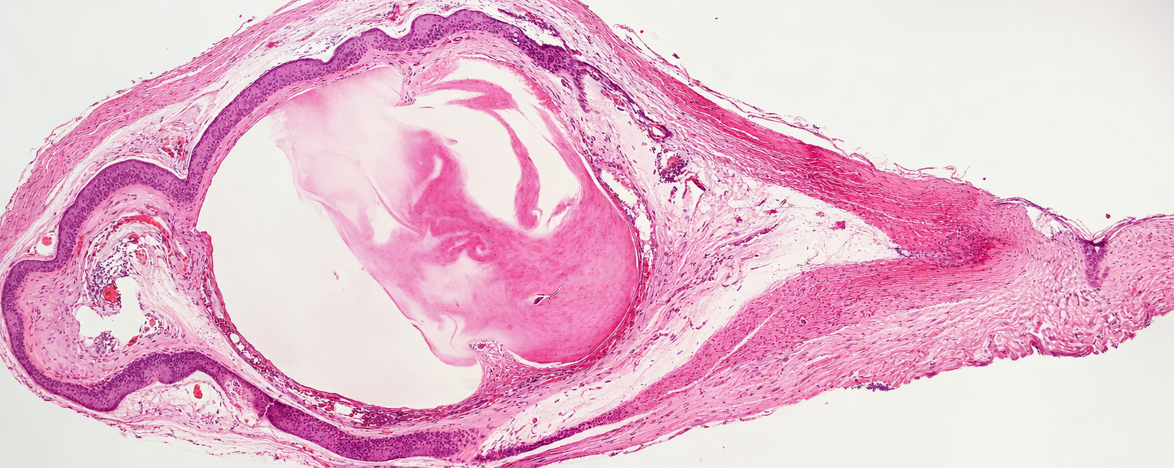 | Figure 7 |
The surrounding tissue is indurated due to prolonged pressure, with inflammatory changes and vascular abnormalities noted. It has been established that an increase in the size of the cyst leads to a progressive reduction in vibration and deterioration of vocal function.Unlike polyps, which are characterised by oedema and vascularisation, cysts have a concealed intra-tissue structure, which may complicate clinical diagnosis. The main differential criterion is the presence of a cavity with a capsule [30,31,32].The combined use of stroboscopy and histology enabled an accurate diagnosis to be made and the optimal treatment strategy to be determined — surgical removal followed by rehabilitation. This approach shortens the duration of treatment and enhances its effectiveness.
3. Conclusions
1. In the study, the healthy control group (n=40) exhibited well-organised mucous membranes, a smooth fibrous structure of the lamina propria, blood vessels within normal limits, and minimal inflammatory infiltration; these findings were used as a ‘reference standard’ for subsequent groups. 2. In cases of vocal fold nodules (VF, n=22), the main histological feature was thickening of the superficial layer of the mucous membrane, consolidation of the layers, and hardening of the fibrous portion of the lamina propria (‘petrification’), which corresponds to stroboscopy findings — incomplete closure and a reduction in the amplitude of the mucosal wave. 3. In cases of vocal fold polyps (VFP, n=20), the histological picture was characterised predominantly by oedema (fluid accumulation), dilation of blood vessels and, in some cases, microhaemorrhages; clinically, unilateral reduction in vibration and deviation of the closure line were more frequently observed. 4. In cases of vocal fold cysts (VFC, n=18), the most important distinguishing feature was a clearly defined cavity within the fold and its wall (thick capsule/inner lining layer), which manifests on stroboscopy as local rigidity, absence of the mucosal wave and a reduction in the area of vibration. 5. In the case of polyps and cysts, given the ‘mass effect’ and mechanical restriction of the structure, conservative treatment alone is often insufficient; in the case of nodules, the changes depend on the stage of the process, and the use of phonopaedic rehabilitation and vocal hygiene allows a high therapeutic effect to be achieved.
4. Practical Recommendations
1. In patients with dysphonia, prolonged hoarseness or ‘vocal fatigue’, an endoscopic examination (with stroboscopy if necessary) is recommended; where suspicious lesions are identified, a targeted biopsy must be performed, followed by histological examination. 2. Any tumour-like formation in the larynx removed (during microlaryngoscopy) should be sent for histological examination; the precise location of the lesion and clinical/stroboscopic findings must be specified in the referral, which improves the accuracy of the differential diagnosis. 3. If a nodule is suspected, it is necessary to assess not only the macroscopic appearance but also the degree of thickening of the mucosal layers and the consolidation of the fibrous component; this allows for the correct determination of the boundaries of conservative (voice hygiene, phonopaedic exercises) and minimally invasive intervention. 4. If a polyp is suspected, the predominance of oedema and the vascular component should be taken into account; the identification of unilateral reduced vibration and deviation of the closure line on stroboscopy, followed by histological confirmation, allows the treatment strategy to be justified (surgical removal + rehabilitation). 5. If a cyst is suspected, and stroboscopy reveals a local ‘stiff area’ and the absence of a mucosal wave, it is recommended to perform a microlaryngoscopic examination and confirm the cyst wall histologically without prolonged medical observation.
References
| [1] | Ahmad K., Yan Y., Bless D. Histopathologic correlates of benign vocal fold lesions. // J Voice. – 2016. – 30(3). – P. 297–303. |
| [2] | Altman K.W., Atkinson C., Lazarus C. Current and emerging concepts in muscle tension dysphonia. // J Voice. – 2015. – 29(1). – P. 62–67. |
| [3] | Arens C., Glanz H., Dreyer T. Advances in laryngeal imaging. // HNO. – 2018. – 66(3). – P. 176–184. |
| [4] | Behlau M., Zambon F., Madazio G. Epidemiology of dysphonia in voice professionals. // J Voice. – 2017. – 31(2). – P. 240.e1–240.e9. |
| [5] | Boessenecker A., Ziethe A., Nawka T. High-speed videoendoscopy in benign laryngeal lesions. // Laryngoscope. – 2019. – 129(3). – P. 707–712. |
| [6] | Cielo C.A., Ribeiro V.V., Hoffmann C.F. Voice therapy in vocal fold nodules: systematic review. // CoDAS. – 2016. – 28(4). – P. 467–474. |
| [7] | Cohen S.M., Garrett C.G. Utility of voice therapy in the management of vocal fold nodules and polyps. // Otolaryngol Clin North Am. – 2019. – 52(4). – P. 627–635. |
| [8] | Dejonckere P.H., Lebacq J. Objective assessment of voice quality: current perspectives. // Eur Arch Otorhinolaryngol. – 2016. – 273(5). – P. 1211–1218. |
| [9] | Fang T.J., Li H.Y., Gliklich R.E. Outcomes of microlaryngoscopic surgery for benign vocal fold lesions. // Ann Otol Rhinol Laryngol. – 2017. – 126(3). – P. 207–214. |
| [10] | Friedrich G., Dikkers F.G. Benign vocal fold lesions: European consensus. // Eur Arch Otorhinolaryngol. – 2016. – 273(10). – P. 2935–2944. |
| [11] | Halum S.L., McRae B.R. Office-based laser treatment of benign vocal fold lesions. // Otolaryngol Clin North Am. – 2019. – 52(4). – P. 691–703. |
| [12] | Heman-Ackah Y.D., Barr A. Voice therapy and outcomes in benign vocal fold lesions. // Curr Opin Otolaryngol Head Neck Surg. – 2016. – 24(3). – P. 209–214. |
| [13] | Hsiung M.W., Pai L., Kang B.H. Histopathology and clinical correlation in vocal fold cysts. // J Formos Med Assoc. – 2019. – 118(3). – P. 677–683. |
| [14] | Kim J., Nam I., Park J. Voice outcomes after surgical treatment of vocal fold polyps. // Clin Exp Otorhinolaryngol. – 2020. – 13(2). – P. 168–175. |
| [15] | Kinnari T.J., Laukkanen A.M. Acoustic voice analysis in clinical practice. // Folia Phoniatr Logop. – 2017. – 69(4). – P. 179–187. |
| [16] | Nakagawa H., Miyamoto M., Kusuyama T. Histological features of vocal fold nodules and polyps. // Auris Nasus Larynx. – 2018. – 45(5). – P. 1011–1017. |
| [17] | Nawka T., Verdonck-de Leeuw I. Voice rehabilitation after phonosurgery. // Curr Opin Otolaryngol Head Neck Surg. – 2019. – 27(6). – P. 439–444. |
| [18] | Omori K. Advances in endoscopic laryngeal surgery. // Auris Nasus Larynx. – 2018. – 45(4). – P. 645–651. |
| [19] | Pedersen M., Eeg M. Vocal fold nodules in professional voice users. // Logoped Phoniatr Vocol. – 2016. – 41(3). – P. 101–107. |
| [20] | Remacle M., Eckel H.E., Antonelli A. Endoscopic cordectomy for early glottic cancer and benign lesions: ELS recommendations. // Eur Arch Otorhinolaryngol. – 2017. – 274(5). – P. 1987–2004. |
| [21] | Remacle M., Van Haverbeke C., Eckel H.E. Laser surgery of benign vocal fold lesions. // Eur Arch Otorhinolaryngol. – 2016. – 273(5). – P. 1209–1215. |
| [22] | Roy N., Barkmeier-Kraemer J., Eadie T. Evidence-based clinical voice assessment. // J Speech Lang Hear Res. – 2017. – 60(11). – P. 3027–3046. |
| [23] | Rosenfeld R.M., Piccirillo J.F. Clinical practice guideline update: adult sinusitis. // Otolaryngol Head Neck Surg. – 2020. – 162(2). – P. S1–S45. |
| [24] | Sataloff R.T., Hawkshaw M.J., Gupta R. Benign vocal fold lesions: update on diagnosis and management. // Curr Opin Otolaryngol Head Neck Surg. – 2017. – 25(6). – P. 453–458. |
| [25] | Sulica L. Vocal fold polyps and nodules. // Otolaryngol Clin North Am. – 2019. – 52(4). – P. 657–670. |
| [26] | Van Haverbeke C., Remacle M. Phonomicrosurgery for benign laryngeal lesions: long-term results. // Eur Arch Otorhinolaryngol. – 2017. – 274(5). – P. 2041–2048. |
| [27] | Verdunck-de Leeuw I.M., Mahieu H.F. Voice handicap and quality of life in benign laryngeal disease. // J Voice. – 2018. – 32(4). – P. 512–518. |
| [28] | Wang C.T., Liao L.J., Cheng P.W. Laryngeal stroboscopy: diagnostic accuracy in benign lesions. // PLoS One. – 2018. – 13(6). – e0198845. |
| [29] | Woo P. Stroboscopy and high-speed imaging of vocal fold vibration. // Otolaryngol Clin North Am. – 2019. – 52(4). – P. 627–640. |
| [30] | Zeitels S.M., Burns J.A., Akst L.M. Advances in phonomicrosurgery. // Laryngoscope. – 2017. – 127(1). – P. 1–13. |
| [31] | Mortensen M., Woo P. Office-based management of benign vocal fold lesions. // Otolaryngol Clin North Am. – 2019. – 52(4). – P. 677–689. |
| [32] | Mehta D.D., Hillman R.E. Voice assessment: updates on acoustic and aerodynamic measures. // Otolaryngol Clin North Am. – 2019. – 52(4). – P. 627–643. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML