-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2358-2362
doi:10.5923/j.ajmms.20261605.26
Received: Mar. 23, 2026; Accepted: Apr. 17, 2026; Published: May 15, 2026

Quadratic Dose-Response Model of Psychomotor Therapy in Post-Stroke Rehabilitation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIbodulloyeva Maftuna Baxtiyor qizi, Ibodullayev Zarifboy Rajabovich
Department of Neurology and Medical Psychology, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Ibodulloyeva Maftuna Baxtiyor qizi, Department of Neurology and Medical Psychology, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study examined the relationship between psychomotor therapy intensity and functional recovery after ischemic stroke using a dose-response approach. A prospective clinical study involving 50 patients was conducted over an 8-week rehabilitation program (32 sessions; total dose ≈1920 minutes). Functional outcomes were assessed using the Fugl-Meyer Assessment, Berg Balance Scale, Barthel Index, and HADS. Quadratic regression analysis revealed a nonlinear dose–response relationship, with the optimal therapeutic range identified at approximately 1000-1300 minutes, where the greatest functional improvement (Δ ≈ 10-11.4 points) was observed. These findings highlight the importance of optimizing rehabilitation intensity to maximize post-stroke functional recovery.
Keywords: Ischemic stroke, Psychomotor therapy, Neurorehabilitation, Dose–response relationship, Functional recovery
Cite this paper: Ibodulloyeva Maftuna Baxtiyor qizi, Ibodullayev Zarifboy Rajabovich, Quadratic Dose-Response Model of Psychomotor Therapy in Post-Stroke Rehabilitation, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2358-2362. doi: 10.5923/j.ajmms.20261605.26.
Article Outline
1. Introduction
- Stroke remains one of the leading causes of long-term disability worldwide and continues to represent a major challenge for modern healthcare systems. Although significant advances in acute stroke management over the past decades have led to a noticeable reduction in mortality, the burden of post-stroke disability remains substantial and poses serious medical, social, and economic challenges for global health services [8,3]. Recent epidemiological estimates indicate that more than 100 million people worldwide are currently living with the consequences of stroke. A considerable proportion of these individuals experience persistent impairments affecting motor function, balance, cognitive processes, and the ability to perform activities of daily living. Consequently, the development of effective and evidence-based rehabilitation strategies has become one of the key priorities in contemporary neurology and neurorehabilitation.The primary objective of post-stroke rehabilitation is to restore lost functions through the activation of neuroplastic mechanisms within the central nervous system. Neuroplasticity refers to the brain’s capacity to reorganize its structure and functional connections following injury. Repetitive and goal-directed motor activity plays a crucial role in facilitating this process [1]. Numerous studies have demonstrated that intensive and repetitive task-oriented movements stimulate sensorimotor integration, promote the formation of new neuronal connections, and contribute to improved motor recovery. For this reason, therapy intensity and the number of repetitions have increasingly been recognized as critical therapeutic factors in modern neurorehabilitation.In recent years, growing attention has been directed toward the concepts of therapeutic load, intensity, and training volume in rehabilitation research. A number of studies report that increasing the amount of rehabilitation training is associated with improved functional outcomes in stroke survivors [7,10]. Nevertheless, the optimal level of therapeutic intensity remains insufficiently defined. Considerable variability exists across studies regarding the duration, frequency, and overall volume of rehabilitation sessions. Moreover, in many rehabilitation trials the actual therapeutic load is not clearly quantified, which complicates the evaluation of the relationship between therapy dosage and clinical outcomes [4]. Therefore, accurate measurement of rehabilitation intensity and identification of the optimal therapeutic dose range represent important scientific challenges in contemporary neurorehabilitation research.Psychomotor therapy represents one of the integrative approaches increasingly applied in post-stroke rehabilitation. This therapeutic model focuses on the simultaneous development of motor control, body schema, balance, sensorimotor integration, and cognitive processes. By targeting multiple functional domains, psychomotor therapy aims to improve movement coordination, body awareness, and the functional control of posture and locomotion, thereby enhancing patients’ ability to perform everyday activities. Importantly, psychomotor interventions engage not only motor pathways but also sensory, proprioceptive, and cognitive mechanisms, which may further stimulate neuroplastic reorganization within the central nervous system. Despite its growing clinical application, however, the relationship between the therapeutic load of psychomotor interventions and clinical recovery outcomes remains insufficiently investigated.From this perspective, examining the relationship between rehabilitation intensity and functional recovery through a dose-response model is of particular scientific interest. The dose–response approach makes it possible to determine how clinical outcomes change as therapy intensity increases, to identify the optimal therapeutic range, and to evaluate the potential decline in effectiveness associated with excessive training loads. Such modeling may provide an important methodological framework for optimizing rehabilitation programs and for developing individualized therapeutic strategies in clinical neurorehabilitation practice.Objective. The aim of this study was to examine the relationship between the intensity of psychomotor therapy and functional recovery outcomes in patients during the post-ischemic stroke period, and to determine the optimal therapeutic dose range using a quadratic regression model.
2. Materials and Methods
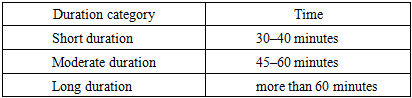
- This study was conducted as a prospective clinical observational investigation aimed at identifying the association between the intensity of psychomotor therapy and functional recovery indicators in patients undergoing rehabilitation after ischemic stroke. During the study, the volume of psychomotor therapy applied within the rehabilitation process (therapy dose) and the changes observed in patients’ clinical and functional outcomes were systematically analyzed. A dose–response approach was employed to evaluate the relationship between therapy intensity and clinical outcomes.The study protocol was organized in accordance with generally accepted ethical principles for clinical research. Prior to participation, all individuals provided written informed consent.A total of 50 patients diagnosed with ischemic stroke and undergoing the rehabilitation phase were included in the study. Participant selection was based on established clinical and neurological criteria. Patients were eligible for inclusion if they met the following conditions:• confirmed diagnosis of ischemic stroke;• stable neurological status;• ability to actively participate in rehabilitation training.Patients presenting with severe cognitive impairment, serious cardiovascular conditions, or other contraindications to active rehabilitation were excluded from the study.Psychomotor Therapy Protocol. The rehabilitation program was structured as a комплекс intervention incorporating elements of psychomotor therapy. The therapeutic program included exercises aimed at improving body schema, balance, coordination, sensorimotor integration, and functional movement. Each therapy session consisted of three main components:• Preparatory phase: light motor activation exercises;• Core therapeutic phase: exercises targeting balance, coordination, and movement control;• Final phase: relaxation and breathing exercises.The rehabilitation program was conducted over a period of eight weeks. Therapy sessions were performed four times per week, with each session lasting 60 minutes. Consequently, the total therapeutic exposure amounted to 32 sessions, corresponding to approximately 1920 minutes of psychomotor intervention.Calculation of Therapy Dose. To determine the dose of psychomotor therapy, the total duration of training sessions was considered the primary indicator. The therapy dose was calculated using the following formula:Dose (minutes) = session duration × number of sessionsThe classification of psychomotor therapy session durations applied in this study is presented in Table 1.
|
3. Results
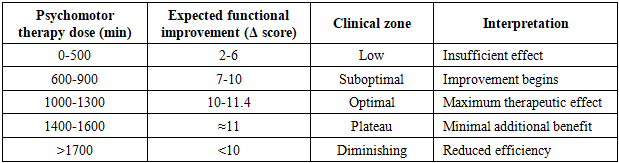
- During the study, the relationship between the intensity of psychomotor therapy and indicators of functional recovery was analyzed. The rehabilitation program was conducted over a period of eight weeks, and the total therapeutic exposure for each participant amounted to 32 sessions, corresponding to approximately 1920 minutes of therapy. Clinical outcomes were assessed using the Fugl-Meyer Assessment (FMA), the Berg Balance Scale (BBS), the Barthel Index, and the Hospital Anxiety and Depression Scale (HADS).To evaluate the influence of therapy dose on functional improvement, regression analysis was first performed. The results of the linear model indicated that increasing therapeutic load was associated with improvements in clinical outcomes. However, the distribution of the data suggested that the relationship was not strictly linear. Therefore, an additional quadratic regression model was applied.Quadratic regression analysis revealed a parabolic dose–response relationship between the intensity of psychomotor therapy and functional recovery. According to the model, increases in therapy dose were initially associated with rapid improvements in clinical indicators; however, beyond a certain point, the rate of improvement gradually slowed. Statistical modeling indicated that the optimal therapeutic range for psychomotor therapy was approximately 1000-1300 minutes. Within this interval, the average functional improvement ranged from 10 to 11.4 points.The relationship between psychomotor therapy dose and functional recovery dynamics is illustrated in Figure 1. The diagram demonstrates that functional outcomes improve substantially as therapeutic load increases, but the rate of improvement begins to decline after reaching a certain threshold.
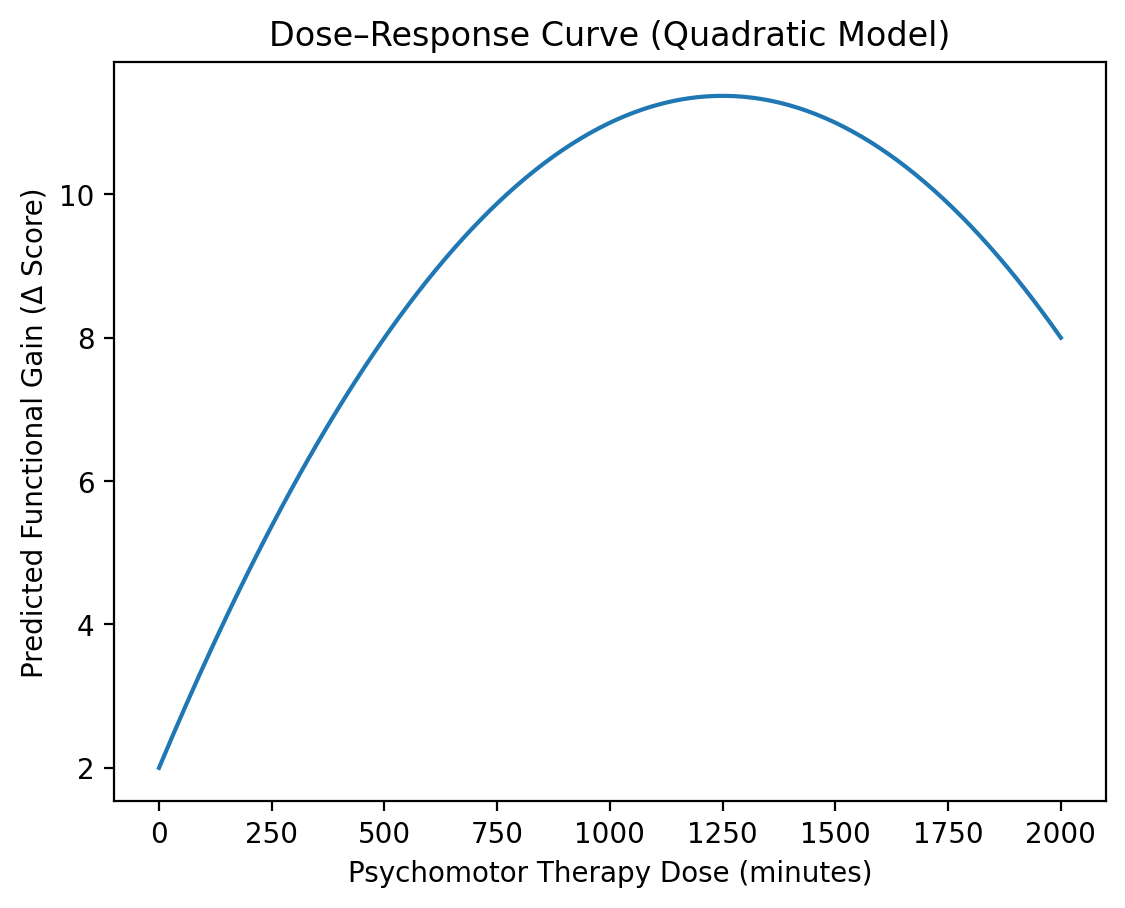 | Figure 1. Quadratic regression model of functional recovery in relation to psychomotor therapy dose |
|
4. Discussion of the Study Findings
- The findings of the present study demonstrate a clear dose–response relationship between the intensity of psychomotor therapy and indicators of functional recovery in patients after ischemic stroke. The results showed that increasing the therapeutic dose was associated with improvements in motor function, balance, and independence in activities of daily living. At the same time, regression analysis revealed that the relationship between therapeutic load and clinical response was not strictly linear. According to the statistical modeling results, the optimal therapeutic range for psychomotor therapy was approximately 1000-1300 minutes, within which the highest levels of functional recovery were observed.These results are consistent with previous clinical studies that have examined the relationship between rehabilitation intensity and functional recovery after stroke. For instance, a systematic review conducted by Langhorne and colleagues reported that increased intensity of rehabilitation training is associated with improved functional outcomes in stroke survivors [7]. Similarly, analyses of randomized controlled trials by Kwakkel and colleagues have demonstrated that both the duration and the repetition of rehabilitation exercises have a direct impact on the degree of motor recovery [6]. However, these studies also noted that once therapy intensity exceeds a certain threshold, the rate of clinical improvement tends to decline.The quadratic dose-response relationship identified in the present study further emphasizes the importance of determining an optimal therapeutic dose during rehabilitation. Insufficient training intensity may fail to adequately activate neuroplastic mechanisms, while excessive therapeutic load may exceed the adaptive capacity of the patient’s organism. Therefore, selecting an appropriate balance between therapy intensity and patient tolerance represents an important clinical consideration in the design of rehabilitation programs. The results of the present analysis suggest that the most effective therapeutic zone for psychomotor therapy lies within the range of approximately 1000-1300 minutes.The findings may also be interpreted within the framework of neuroplasticity theory. It is well established that the capacity of the central nervous system to reorganize after injury plays a critical role in post-stroke recovery. Repetitive and goal-directed movements promote the formation of new synaptic connections and facilitate functional reorganization of damaged neural networks [5]. Psychomotor therapy incorporates a variety of movement-based activities involving sensorimotor integration, balance, and body control, which are likely to stimulate these neuroplastic processes and thereby support functional recovery.In addition, the AVERT randomized clinical trial conducted by Bernhardt and colleagues demonstrated that early mobilization and rehabilitation intensity can significantly influence functional outcomes after stroke [2]. At the same time, that study also indicated that excessively intensive rehabilitation does not necessarily lead to additional clinical benefits. This observation corresponds with the phenomenon identified in the present study, namely the diminishing marginal therapeutic effect observed when therapy intensity exceeds an optimal level.Another important aspect of this study is the evaluation of the relationship between psychomotor therapy intensity and psycho-emotional indicators. The results suggest that although motor and balance outcomes were strongly associated with therapy dose, changes in psycho-emotional indicators measured by the HADS scale were more modest. This finding may indicate that mechanisms underlying motor recovery tend to respond more rapidly to rehabilitation interventions than psychological factors.From a clinical perspective, the results of this study have important practical implications for planning post-stroke rehabilitation programs. The proposed dose–response model provides a framework for optimizing therapeutic load, designing individualized rehabilitation strategies, and predicting potential clinical outcomes. Furthermore, this approach may contribute to the standardization of psychomotor therapy protocols and improve the overall effectiveness of rehabilitation interventions.
5. Conclusions
- The present study aimed to evaluate the relationship between the intensity of psychomotor therapy and functional recovery in patients undergoing rehabilitation after ischemic stroke within the framework of a dose-response paradigm. The results indicate that increasing the total volume of psychomotor therapy is associated with improvements in motor function, balance, and independence in activities of daily living. At the same time, statistical modeling demonstrated that the relationship between therapeutic load and clinical response is nonlinear.Using a quadratic regression model, the optimal therapeutic range for psychomotor therapy was identified as approximately 1000-1300 minutes, within which the highest levels of functional recovery were observed. Beyond this interval, the rate of clinical improvement tended to decline, suggesting that excessive therapeutic load does not necessarily lead to better outcomes.The findings of this study provide further scientific support for the concept of an optimal therapeutic dose in psychomotor rehabilitation. Repetitive and goal-directed movements stimulate the neuroplastic capacity of the central nervous system; however, for these processes to be effective, therapy intensity should be tailored to the patient’s individual functional capacity.The proposed dose–response model may serve as an important methodological tool for evidence-based planning of post-stroke neurorehabilitation, optimization of therapeutic load, and development of individualized rehabilitation programs. In clinical practice, such an approach may contribute to improving rehabilitation outcomes, personalizing therapeutic strategies, and enhancing the prediction of functional recovery.