-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2353-2357
doi:10.5923/j.ajmms.20261605.25
Received: Apr. 13, 2026; Accepted: May 6, 2026; Published: May 13, 2026

Clinical and Anamnestic Characteristics of Women with Endometriosis-Associated and Tubo-Peritoneal Infertility: A Retrospective Case–Control Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMukhammadjonova Mohidil Muzaffarovna, Gafurova Feruza Akhrorovna
Center for the Development of Professional Qualifications of Medical Workers, Department of Obstetrics, Gynecology and Perinatal Medicine, Tashkent, Republic of Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

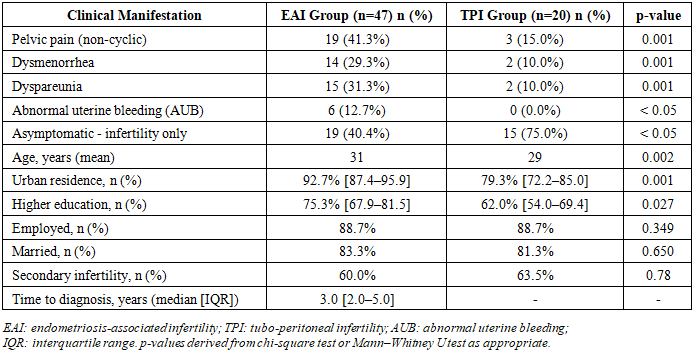
Background: Endometriosis affects approximately 10% of women of reproductive age and is a leading cause of both chronic pelvic pain and infertility. Despite its high prevalence, the condition is frequently underdiagnosed, with an average delay of up to 12 years from symptom onset to confirmed diagnosis reported in some international series. Objective: To compare clinical, anamnestic, and reproductive characteristics in women with endometriosis-associated infertility (EAI) and tubo-peritoneal infertility (TPI). Study Design: Retrospective case–control study. Methods: Sixty-seven women were enrolled: 47 with EAI and 20 with TPI presenting to two tertiary gynaecological departments in Tashkent. All patients underwent comprehensive clinical and gynaecological evaluation, transvaginal ultrasound with Doppler velocimetry, hysteroscopy, laparoscopy with lesion staging per the revised American Society for Reproductive Medicine (r-ASRM) classification, and Endometriosis Fertility Index (EFI) scoring. Statistical analysis was performed using Microsoft Excel and Statistica v6.1. Results: Women with EAI were significantly older (31 vs. 29 years; p=0.002) and more frequently urban residents (92.7% vs. 79.3%; p=0.001). The prevalence of pelvic pain (41.3% vs. 15.0%), dysmenorrhea (29.3% vs. 10.0%), and dyspareunia (31.3% vs. 10.0%) was significantly higher in the EAI group (all p=0.001). Abnormal uterine bleeding occurred exclusively in EAI patients (12.7%). In 40.4% of EAI cases, infertility was the sole presentation. Early-stage disease (r-ASRM I–II) was found in 57.3%, with advanced stages in 42.7%. The most common lesion sites were uterine ligaments (80.0%), pelvic peritoneum (60.0%), and ovaries (40.0%). Mean EFI was 6.7±2.6. Diagnostic delay reached 3.0 [2.0–5.0] years. Conclusions: EAI has a distinct clinical phenotype, yet nearly 40% of affected women are asymptomatic, underscoring the diagnostic challenge. An EFI of 6.7 predicts favorable reproductive outcomes after surgery. Earlier referral for diagnostic laparoscopy in infertile women with suspected endometriosis is warranted.
Keywords: Endometriosis, Endometriosis-associated infertility, Tubo-peritoneal infertility, Endometriosis Fertility Index, Pelvic Pain, Dysmenorrhea, Laparoscopy, Adenomyosis
Cite this paper: Mukhammadjonova Mohidil Muzaffarovna, Gafurova Feruza Akhrorovna, Clinical and Anamnestic Characteristics of Women with Endometriosis-Associated and Tubo-Peritoneal Infertility: A Retrospective Case–Control Study, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2353-2357. doi: 10.5923/j.ajmms.20261605.25.
1. Introduction
- Endometriosis - the ectopic implantation of endometrial-like glands and stroma outside the uterine cavity - is one of the most prevalent and clinically consequential gynaecological disorders of the reproductive age. It affects an estimated 190 million women worldwide, representing approximately 10% of all women of reproductive age. [7] The condition accounts for up to 50% of cases of female infertility presenting for specialist evaluation, [7,14] and is the leading cause of chronic pelvic pain, dysmenorrhea, and dyspareunia in women of reproductive age. [1,7] The economic burden of endometriosis is substantial: direct treatment costs and productivity losses are estimated to exceed €10,000 per patient per year in European health systems. [7] In parallel with its reproductive consequences, endometriosis is associated with a significantly elevated risk of ovarian cancer (primarily clear-cell and endometrioid subtypes), [10] an increased risk of rheumatoid arthritis and other autoimmune conditions, [5] and cardiovascular comorbidities attributable to chronic inflammation and hormonal dysregulation.The pathogenesis of endometriosis remains incompletely understood and is considered multifactorial. The most widely accepted theory - retrograde menstruation with peritoneal implantation - does not fully explain the diverse anatomical presentations of the disease, including deep infiltrating, ovarian, and extrapelvic forms. [7] Contemporary models emphasize the critical role of immune dysfunction: women with endometriosis demonstrate impaired natural killer cell activity, macrophage dysregulation, and a pro-inflammatory peritoneal environment characterized by elevated concentrations of interleukin-6 (IL-6), tumour necrosis factor-alpha (TNF-α), and vascular endothelial growth factor (VEGF). [6] Haemoglobin-induced continuous macrophage activation within endometriotic cysts has been proposed as a mechanism driving both inflammatory progression and malignant transformation. [6] Genetic predisposition, epigenetic modifications, and microbiome alterations are additional contributors to disease susceptibility and severity. [7]One of the most clinically significant challenges associated with endometriosis is the persistent delay in diagnosis. Population-based studies from Europe and North America consistently report mean diagnostic lags of 7–12 years from the onset of symptoms to surgical confirmation. [7,11] In a landmark analysis, Chapron et al. (2019) attributed this delay to the normalization of dysmenorrhea by patients and clinicians, the non-specific character of pelvic pain symptoms, and the historical reliance on surgical confirmation as the diagnostic gold standard. [7] This delay has direct reproductive consequences: progressive ovarian reserve depletion associated with endometriomas - affecting anti-Müllerian hormone levels even at early disease stages [8,9] - and the accumulation of pelvic adhesions and tubal damage reduce fertility potential with each year of untreated disease.Tubo-peritoneal infertility (TPI), arising from tubal occlusion, peritubal adhesions, or hydrosalpinx secondary to pelvic inflammatory disease, represents a pathologically and clinically distinct cause of female infertility. [14] While both EAI and TPI may coexist within the same patient and share peritoneal involvement, their clinical presentations, risk factor profiles, and surgical management strategies differ substantially. A systematic understanding of the clinical, anamnestic, and morphological differences between these two entities is essential for optimizing the diagnostic pathway and reducing the delay to definitive treatment - particularly in Central Asian reproductive medicine contexts where standardized screening protocols for endometriosis remain underdeveloped.The Endometriosis Fertility Index (EFI), validated by Adamson and Pasta (2010) as a reproducible postoperative scoring tool, integrates key clinical, historical, and surgical parameters to predict non-ART pregnancy probability following endometriosis surgery. [15,17] Recent data confirm that EFI outperforms the r-ASRM staging system in predicting natural conception rates, [18] and guidelines from the European Society of Human Reproduction and Embryology (ESHRE, 2022) recommend its use as a standardized element of postoperative counseling. [7] However, EFI-based data from Central Asian populations with mixed EAI and TPI pathology are lacking.The purpose of the present study was to conduct a comparative evaluation of clinical, anamnestic, and morphological characteristics in women with endometriosis-associated versus tubo-peritoneal infertility, and to assess postoperative reproductive prognosis using the Endometriosis Fertility Index.
2. Materials and Methods
- A retrospective case–control study was conducted enrolling 67 women who presented to the gynaecological departments of the Tashkent Branch of the Republican National Center for Maternal and Child Health and Tashkent City Maternity Hospital No. 3. The study population comprised 47 women with endometriosis-associated infertility (EAI; Group I) and 20 women with tubo-peritoneal infertility (TPI; Group II). Diagnosis of endometriosis was established based on integrated clinical, instrumental, and histological criteria; adenomyosis was classified per histological criteria of spread. All patients underwent laparoscopy with staging per the revised American Society for Reproductive Medicine (r-ASRM) classification and postoperative EFI scoring.Clinical assessment included systematic documentation of symptoms, menstrual history, obstetric and gynaecological history, somatic comorbidities, and prior interventions. All patients underwent transvaginal ultrasound with colour Doppler velocimetry, hysteroscopy, serological testing for sexually transmitted infections, and standard biochemical and haematological evaluation. Statistical analysis was performed using Microsoft Excel and Statistica v6.1 (StatSoft Inc., USA); p < 0.05 was considered statistically significant.
3. Results and Discussion
- The mean age of patients in Group I was 31 years versus 29 years in Group II (p=0.002). Women with EAI were more frequently urban residents (92.7% vs. 79.3%; p=0.001) and had higher educational attainment (75.3% vs. 62.0%; p=0.027). Both groups were comparable in employment and marital status (p > 0.05). The full comparison of clinical manifestations and patient characteristics is presented in the Table.
|
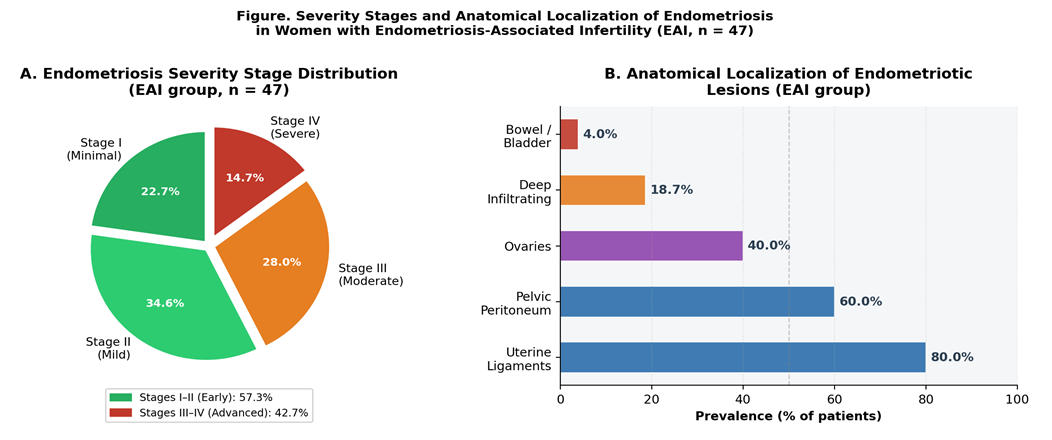 | Figure 1. A: Distribution of endometriosis severity stages (r-ASRM classification) in EAI patients (n=47). B: Anatomical localization of endometriotic lesions (percentage of patients; multiple localizations per patient possible). The predominance of ligamentous and peritoneal involvement is consistent with published data on deep compartment disease in infertile women |
4. Conclusions
- Women with endometriosis-associated infertility demonstrate a distinct clinical and anamnestic phenotype compared to those with tubo-peritoneal infertility, characterized by significantly higher rates of pelvic pain, dysmenorrhea, dyspareunia, and abnormal uterine bleeding, as well as older age at presentation. Critically, approximately 40% of EAI patients are entirely asymptomatic at diagnosis, indicating that pain-free presentation does not exclude active endometriosis in an infertile woman. A mean EFI score of 6.7±2.6 in the EAI cohort indicates a favorable postoperative reproductive prognosis for the majority of surgically treated patients, consistent with current prognostic benchmarks. Despite a diagnostic delay shorter than in Western series, the 3-year median delay remains clinically significant given the progressive impact of endometriosis on ovarian reserve.These findings reinforce the need for a low threshold for laparoscopic evaluation in infertile women regardless of pain symptom burden, routine EFI scoring as a postoperative counseling standard, and prospective multicenter studies to establish optimal timing and indications for surgical intervention in Central Asian reproductive medicine contexts.