Alimov Ulugbek Khudoyarovich1, Rustamov Uygun Tursunovich2
1Center for Professional Development of Medical Personnel, Tashkent, Uzbekistan
2Bukhara State Medical University named after Abu Ali ibn Sina, Bukhara, Uzbekistan
Correspondence to: Rustamov Uygun Tursunovich, Bukhara State Medical University named after Abu Ali ibn Sina, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
In recent years, increasing attention has been paid within the scientific community to the relationship between somatic and mental disorders. The development of these pathological conditions is multifactorial and is grounded in a systemic conceptual framework. To investigate this group of pathologies, 172 patients diagnosed with gastric and duodenal cancer who were hospitalized at the Bukhara Regional филиал of the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology between 2021 and 2024 were examined. It should be emphasized that, when describing the clinical manifestations of mental disorders in patients with gastric and duodenal cancer, there are no clear boundaries between psychogenic and somatogenic disturbances due to the complex dynamic interactions and mutual influence of key pathogenetic factors. However, from a practical standpoint, a differential approach to the analysis of their clinical features is considered appropriate, as it enables the development of pathogenetically substantiated and individually oriented methods for the correction of psychopathological changes.
Keywords:
Oncopathology, Psychopathology, Somatogenic mental disorders, Nosogenic reactions
Cite this paper: Alimov Ulugbek Khudoyarovich, Rustamov Uygun Tursunovich, Mental Disorders Observed in Malignant Tumors of the Stomach and Duodenum, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2280-2286. doi: 10.5923/j.ajmms.20261605.13.
1. Introduction
Gastric cancer is one of the most prevalent oncological diseases worldwide and is characterized by high morbidity and mortality rates among the population. According to the World Health Organization and GLOBOCAN data, approximately 968,000 to 1.1 million new cases of gastric cancer are registered annually worldwide [1,2,6]. This accounts for about 5–6% of all oncological diseases. Gastric cancer ranks 5th–6th in incidence and 4th in mortality among all malignancies [3,4].Globally, the age-standardized incidence rate of gastric cancer averages 9.2 cases per 100,000 population. This rate is significantly higher among men (15.8 per 100,000) compared to women (7.0 per 100,000) [5,6]. The highest incidence rates are observed in East Asian countries, particularly in Japan, South Korea, and China. Elevated rates are also reported in Eastern Europe and South America, whereas the lowest incidence is observed in Africa, North America, and Western Europe. Notably, the largest number of cases worldwide is registered in China, accounting for more than 40% of all cases globally. High incidence rates are also reported in India and Russia [7,12,14].In contrast, duodenal cancer is a relatively rare malignancy among gastrointestinal tumors. It accounts for approximately 0.3–1% of all gastrointestinal neoplasms and less than 0.5% of all oncological diseases. Globally, the incidence rate of duodenal cancer is less than 0.5 cases per 100,000 population. In Europe and North America, this figure is approximately 3–4 cases per 1 million population [8,9,10].The clinical structure and dynamics of psychopathological changes developing in patients with gastric and duodenal cancer under the simultaneous influence of psychogenic and somatogenic factors remain insufficiently studied. Specialized research in this field is limited, and the findings reported by different authors are often inconsistent and contradictory [11,14,15].At the same time, the insufficient understanding of the clinical features and dynamics of mental disorders significantly complicates the development of optimal, comprehensive treatment and preventive programs aimed at improving the quality of life of patients with gastric and duodenal cancer.
2. Aim
The aim of the study was to investigate the structure and clinical transformation of mental disorders in patients with gastric and duodenal cancer. This objective required determining the prevalence, clinical structure, and main psychopathological syndromes of mental disorders in this patient population, as well as assessing their clinical dynamics and syndromal transformation during the course of treatment.
3. Materials and Methods
To achieve the stated aim and objectives, a total of 172 patients diagnosed with gastric and duodenal cancer were examined.The main group included patients with gastric and duodenal cancer accompanied by comorbid psychopathological disorders who, in addition to standard oncological treatment and surgical intervention, received:• psychocorrective interventions (supportive psychotherapy, psychoeducation); • psychotropic therapy according to clinical indications (antidepressants, anxiolytics, and low-dose antipsychotics); • dynamic psychiatric monitoring in the early postoperative period. The comparison group consisted of patients with similar oncological pathology and psychopathological disturbances who received:• standard oncological treatment and surgical intervention; • symptomatic somatic therapy. For comparative purposes, no specialized psychocorrective interventions or psychotropic medications were administered to this group.The study was conducted using the following methods:• clinical-psychopathological method; • clinical follow-up (catamnestic) method; • experimental-psychological assessment.
4. Results and Discussion
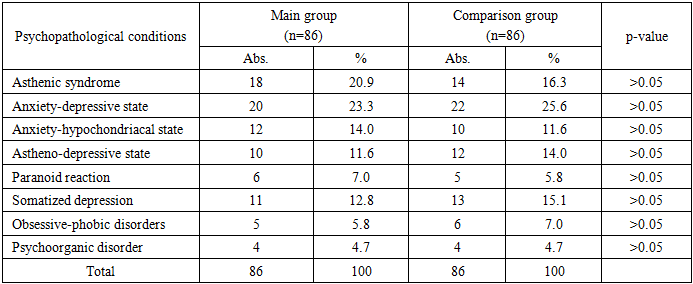
A retrospective analysis of anamnestic data demonstrated that in all patients, mental disorders had already developed at the pre-hospital stage, namely during the period of examination and diagnosis of gastric and duodenal cancer. These disturbances manifested as a psychological response of the individual to their illness and to the situation of interaction with oncological care services. The mental disorders showed a clear association with psychotraumatic circumstances, with their severity increasing during the waiting period for diagnostic results and after being informed about the need for radiotherapy, chemotherapy, or surgical intervention.In 96.3% of patients, somatogenic asthenia associated with the oncological disease was observed prior to the development of psychogenic reactions, and it further intensified during the course of chemotherapy or radiotherapy. Somatogenic asthenia was characterized by a hypersthenic pattern, manifesting as hypersthenic weakness, increased sensitivity to emotional stimuli, pronounced emotional lability, a tendency to tearfulness in response to minor triggers, rapid fatigability, and general weakness. These symptoms could progress to aspontaneity, passivity, apathy, and a subjective sense of inactivity, particularly during periods of radiotherapy and chemotherapy. In addition, agrypnic disturbances were noted, including impaired nocturnal sleep, inversion of the sleep–wake cycle (daytime somnolence and nocturnal insomnia), as well as autonomic dysfunctions.The manifestations of somatogenic asthenia can be considered a favorable “background” for the development of psychogenic reactions, which were observed to occur against the backdrop of persistent asthenic disturbances. Thus, by the time of admission to the oncological clinic, the majority of patients already exhibited varying degrees of mental dysfunction. In this context, the preoperative condition itself acted as an additional stressor, contributing to the exacerbation of psychopathological changes. Direct clinical observation of patients in the oncological setting enabled the identification of clinical forms and the assessment of the subsequent dynamics of mental disorders.The structure of mental disorders was analyzed in accordance with the study objectives and the obtained data on their prevalence and composition. A wide spectrum of psychopathological disturbances was identified across both the total sample and specific subgroups, regardless of their genesis and relationship with somatic pathology.The analysis of prevalence rates of clinically formed mental disorders, as well as the study of their clinical structure (including the mildest forms), confirmed a general trend reported in contemporary research: a high frequency of neurotic-spectrum disorders with a predominance of depressive and anxiety disturbances. At the same time, relatively more severe forms belonging to higher psychopathological registers (compared to neurotic and affective disorders) were also identified.It should be noted that psychopathological disturbances developing in the context of oncological pathology may manifest either as nosogenic (psychogenic) reactions to a severe somatic illness or as exogenous psychopathological disorders. However, clear differentiation between these clinical forms is often challenging, as distinct boundaries between them are difficult to establish (Table 1).Table 1. Distribution of Psychopathological Disorders in the Study Groups
 |
| |
|
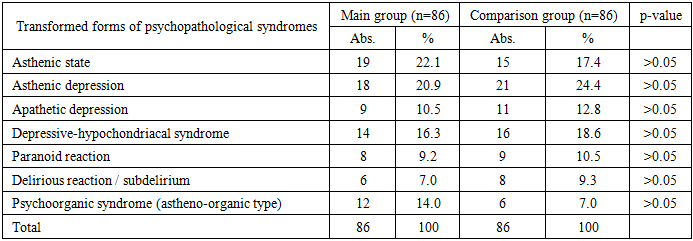
The distribution of psychopathological disorders did not reveal statistically significant differences between the main and comparison groups (p>0.05). Anxiety-depressive and asthenic syndromes predominated in both groups, confirming the leading role of neurotic-spectrum disorders in patients with gastric and duodenal cancer.Despite the heterogeneity of the psychopathological disorders presented in the table, all of them developed against the background of the primary oncological disease and manifested with varying degrees of clinical severity. No statistically significant differences were found between the main and comparison groups across all psychopathological syndromes (in all cases p > 0.05), indicating their comparability in terms of clinical and psychopathological structure.Following hospitalization, both study groups demonstrated a predominance of asthenic conditions and anxiety-depressive disorders (20.9% and 16.3%; 23.3% and 25.6%, respectively). The asthenic syndrome was characterized by pronounced physical, mental, and cognitive exhaustion, along with fatigue. Similar to other severe somatic conditions, in the oncological pathology studied, asthenia emerged as a leading psychopathological syndrome. Clinically, asthenic disturbances tended to follow a relatively chronic course, showed a propensity for progression, and varied depending on the patient’s somatic condition and the administered antitumor therapy.Anxiety-depressive disorders most often developed acutely as nosogenic reactions immediately following exposure to psychotraumatic factors. They were characterized by general restlessness, marked anxiety—sometimes reaching the level of fear—as well as feelings of hopelessness and meaninglessness of life. In the context of severe somatic illness, patients frequently developed thoughts about the inevitability of a painful death, with increasing overlap between anxiety and depressive affect. In cases where depressive affect was not profound, it was primarily expressed as emotional oppression and low mood, with anxiety components predominating in the syndrome structure.These manifestations were particularly pronounced upon being informed of the scheduled date of surgery and during the immediate preoperative period. In some cases, anxiety and fear were accompanied by marked agitation, which complicated preoperative preparation and the surgical process itself.Anxiety-hypochondriacal states ranked next in frequency (14.0% in the main group and 11.6% in the comparison group). Clinically, they manifested as persistent anxious anticipation of disease progression, combined with heightened attention to bodily sensations. Such patients frequently complained of vague internal sensations, suspected the presence of metastases, and continuously found new reasons for concern. They persistently addressed the treating physician with complaints and questions, inquiring about possible surgical outcomes, expressing concerns about delayed diagnosis, and fearing that surgical intervention might prove ineffective.Moreover, these patients often exhibited excessive concern about potential complications at subsequent stages of clinical follow-up. Particular attention was drawn to their fixation on thoughts related to bodily defects following radical surgical interventions on the stomach and duodenum.Astheno-depressive states (11.6% in the main group and 14.0% in the comparison group) were observed to develop relatively gradually. They were characterized by depressed mood, lethargy, indifference to one’s fate, and a passive acceptance of death associated with the illness and a perceived “unsuccessful operation.” Psychomotor retardation was markedly pronounced, with patients responding reluctantly and briefly to questions, particularly those of a closed or negative nature. The development of affective symptoms was closely associated with the course of somatogenic asthenia, manifesting as rapid mental exhaustion and decreased motivation for activity. These reactions tended to persist for a longer duration, with a slow and gradual recovery process, although the connection with the psychotraumatic situation remained evident.Obsessive-phobic disorders were identified in both study groups (5.8% and 7.0%, respectively). These conditions were characterized by the emergence of intrusive, emotionally charged and imagery-based thoughts against a background of pronounced anxiety. They were predominantly manifested as hypochondriacal phobias, including cardiophobia (fear of cardiac arrest), fear of suffocation, fear of not awakening after anesthesia, and concerns about “damage to vital organs” during surgery. In some cases, intrusive images related to one’s own death and funeral were also reported. Patients complained about the uncontrollable nature of these thoughts and reported unsuccessful attempts to resist them, “push them away,” or redirect attention, often seeking medical assistance. Notably, a reduced level of critical insight toward these obsessive experiences was observed.Paranoid-type mental disorders were observed in the study groups (7.0% and 5.8%, respectively), primarily as psychogenic reactions. These were characterized by suspicion, mistrust, and doubts directed toward physicians and medical staff. Such reactions manifested as social withdrawal, reluctance to engage, skepticism regarding the necessity of surgery, doubts about the adequacy of therapeutic strategies, and questioning of medical competence. Patients often demanded additional examinations and consultations. Paranoid ideas were predominantly overvalued in nature, frequently with hypochondriacal content, and accompanied by the formation of rigid personal beliefs about their illness. Patients strongly defended their subjective interpretations of their somatic condition and, in some cases, insisted on therapeutic interventions that did not correspond to their objective clinical status. Refusal by physicians to comply with such demands often led to increased mistrust. Against the background of lowered mood, irritability, dissatisfaction, and occasional episodes of anger were observed, along with anxiety and fear.The results of the observations indicate that psychoorganic syndrome occurred with equal frequency in both study groups (4.7%) and demonstrated a gradual course. During the initial clinical interviews, asthenic symptoms and mild cognitive impairments were identified, which had often been previously interpreted as consequences of worsening somatic condition or depressive reactions. Clinically, the psychoorganic syndrome was mild, presenting as asthenic states accompanied by mental and physical fatigue, emotional lability, and impaired concentration. A decrease in working memory was observed, while long-term memory remained relatively preserved. Fluctuations in symptom severity during the day were noted, with partial improvement in cognitive functioning following rest.The depressive syndrome observed in the study groups (12.8% and 15.1%, respectively) differed from classical affective disorders by its atypical clinical presentation and pronounced somatization. In many patients, asthenic, autonomic, and somatic symptoms predominated, giving depression a “masked” character and significantly complicating its timely diagnosis in oncological patients. Depressive states represented the most frequently observed syndrome among affective disorders and were present within the clinical structure of all identified psychopathological disturbances.In some patients, depressive syndrome was observed in combination with asthenic and cognitive impairments, manifesting as a component of psychoorganic syndrome. This finding suggests a transformation of nosogenic depression into an affective disorder of organic genesis, likely associated with progression of the underlying disease.At all stages of inpatient treatment, mental disorders manifested against the background of somatogenic asthenia, which was directly обусловлено the oncological condition. In 95.4% of patients, mental disturbances had already developed at the pre-hospital stage. Their development could be clearly linked to gastric and duodenal cancer, as no psychiatric disorders were identified in the premorbid period. A distinctive feature of these disturbances was their persistent course and their tendency to worsen during chemotherapy and radiotherapy.Thus, depressive syndrome should be regarded as a complex, multidimensional mental disorder formed under the combined influence of psychogenic, somatic, and organic mechanisms. This substantiates the need for early detection and a comprehensive, interdisciplinary approach to management, involving mandatory participation of psychiatrists and clinical psychologists in the treatment of oncological patients.Furthermore, in gastric and duodenal tumors, psychoorganic syndrome can be considered a закономерное complication arising under the influence of nutritional, metabolic, hypoxic, and iatrogenic factors. Its early identification and inclusion in a comprehensive treatment strategy are essential for improving therapeutic outcomes, enhancing patients’ quality of life, and optimizing medical and social rehabilitation.During clinical follow-up, changes in the clinical presentation of psychopathological disorders were observed in patients from both study groups. In patients with gastric and duodenal cancer, pronounced somatopsychic disturbances developed as a result of surgical stress (in operated patients), metabolic disorders, and acute changes in somatic condition. This was manifested either by clinical transformation of pre-existing mental disorders or by the emergence of new psychopathological syndromes.The obtained clinical observations indicate that, during follow-up, mental disorders were predominantly transient and syndromally polymorphic. However, in a proportion of patients, they served as a starting point for the development of stable organic mental disorders (Table 2).Table 2. Clinical-Dynamic Transformation of Psychopathological Disorders During Follow-up
 |
| |
|
The data presented in the table indicate that the initially predominant asthenic syndrome, during clinical follow-up, most frequently transformed into either asthenic states (22.1% and 17.4%, respectively) or astheno-depressive forms (20.9% and 14.0%) in both study groups. These conditions were characterized by increased mental and physical exhaustion, reduced tolerance to sensory and emotional stressors, sleep disturbances, and autonomic lability. In a subset of patients, asthenic disturbances progressed to the level of astheno-organic syndrome, accompanied by cognitive decline and partial reduction of insight into their condition.In its dynamic course, astheno-depressive syndrome often evolved into apathetic depression (29% and 24.4%, respectively) or astheno-organic forms (14.0% and 7.0%). These clinical variants were characterized by apathy, decreased activity, psychomotor retardation, and emotional blunting against a background of subjectively experienced sadness. They were associated with higher severity of depressive symptoms and reflected early signs of psychoorganic process formation. In cases initially presenting with anxiety-depressive syndrome, the reactive component of depression decreased over time, with astheno-depressive or apathetic variants becoming predominant. Anxiety symptoms were frequently somatized, manifesting as dyspeptic complaints and subjective discomfort related to the cardiovascular and respiratory systems.Anxiety-hypochondriacal syndrome predominantly transformed into depressive-hypochondriacal forms (16.3% and 18.6%), characterized by rigid fixation on somatic sensations, excessive concern regarding surgical outcomes, and, in some cases, reduced trust in treatment.In patients initially presenting with obsessive-phobic disorders, follow-up observations demonstrated that these symptoms were frequently combined with asthenic and depressive features. Obsessive thoughts and phobic fears became integrated with concerns related to physical condition and surgical intervention, contributing to the intensification of a psychasthenic profile.Although paranoid reactions were less frequent at later stages of follow-up, in some patients (9.2% and 10.5%, respectively) they acquired an organic-paranoid character, manifested by suspiciousness, misinterpretation of others’ actions, and emotional instability. These conditions were particularly evident against the background of severe somatic status and reduced cognitive resources.Of particular clinical significance, acute exogenous-organic reactions, including delirious and subdelirious states, were observed in both groups (7.0% and 9.3%, respectively). These conditions were typically transient and regressed with stabilization of the somatic condition; however, they were considered unfavorable prognostic indicators for the subsequent development of psychoorganic syndrome.Thus, during clinical follow-up, the dynamics of psychopathological disorders were characterized by an increase in asthenic, depressive, and organic components, as well as a transition of anxiety from reactive forms to somatic and organic variants. The identified clinical transformations reflect a continuum in the formation of psychoorganic syndrome and substantiate the need for early psychiatric intervention and psychoprophylactic measures.The presence of somatogenic asthenia associated with gastric and duodenal cancer rendered patients more vulnerable and less resilient to stress. Somatogenic asthenia created a background for the development of reactive syndromes and significantly influenced both the clinical presentation and course of psychogenic reactions. A close interweaving of psychogenic and somatogenic mental disturbances within its structure was clearly observed.During clinical follow-up (week 3), psychopathological disorders were characterized clinically by syndromal transformation and psychometrically by changes in scores on the HDRS, HAM-A, and Mini-Mult scales. The integrative analysis of clinical and psychometric data demonstrated that these disturbances were not purely reactive but increasingly acquired a somatogenic-organic nature (Table 3).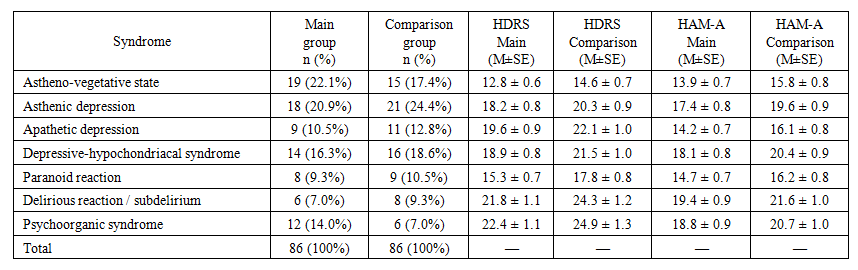 | Table 3. Psychometric Indicators of Transformed Psychopathological Syndromes |
According to the data presented in the table, the results of clinical-dynamic follow-up of patients in the study groups demonstrated that the transformation of asthenic syndrome into astheno-vegetative, astheno-depressive, and astheno-organic forms corresponded to a steady increase in depressive symptomatology as measured by the Hamilton Depression Rating Scale (HDRS). In astheno-vegetative variants, total HDRS scores were predominantly within borderline ranges (12.8 ± 0.6 and 14.6 ± 0.7, respectively), whereas in astheno-depressive and particularly astheno-organic forms, HDRS scores ≥17 predominated (22.4 ± 1.1 and 24.9 ± 1.3, respectively). These findings indicate that the observed psychopathological states were largely shaped by somatized and apathetic components of depressive disorders.Data obtained using the Hamilton Anxiety Rating Scale (HAM-A) confirmed that, in asthenic transformations, psychic anxiety tended to decrease, while somatic anxiety became predominant. Clinically, this corresponded to the dominance of fatigue, autonomic lability, and somatic discomfort.The clinical-dynamic transformation of initially identified psychopathological disorders in the study groups followed consistent patterns during follow-up. Astheno-depressive, apathetic depressive, and astheno-organic forms predominated and showed a reliable association with higher levels of depressive symptomatology (HDRS), increased somatic components of anxiety (HAM-A), and strengthening of organic and obsessive-phobic profiles according to the Mini-Mult scale.Although obsessive-phobic disorders and paranoid reactions were less frequent, they demonstrated high clinical significance in psychometric assessment and may be considered risk factors for early psychoorganic transformation. The shift toward a leading position of astheno-depressive disorders is likely associated with temporary deterioration of the patients’ general condition following radiotherapy, chemotherapy, and complex surgical interventions, as well as with significant limitations in self-care functions and variability in adaptation processes.Clinically, patients exhibited increased irritability, weakness, and hyperesthesia to external physical stimuli, while fatigue and exhaustion were sometimes less prominently expressed. Such patients often demonstrated explosiveness, impatience, irritability, and dissatisfaction with minor triggers in interpersonal interactions. Episodes of anger were typically short-lived and followed by tearfulness and feelings of self-devaluation. Marked mood lability, increased sensitivity to emotional stimuli, and sleep disturbances were also observed. In some patients, irritability and explosiveness were accompanied by dysphoric mood states.Within the clinical structure of somatogenic asthenia, pronounced weakness, rapid mental and physical fatigability, asthenia, and adynamia predominated, indicating a relatively severe course of asthenic syndrome. In elderly patients, periodic general cerebral symptoms such as headaches and dizziness were commonly observed. Emotional lability, including tearfulness, irritability, and a tendency toward persistently lowered mood, was sufficiently pronounced. As asthenia progressed, signs of aspontaneity, passivity, and indifference to the environment increased.A notable feature was that, in the early stages, emotional stress inherent to stressful conditions did not immediately lead to pronounced changes in mental state. In this group of patients, mental disturbances were largely limited to asthenic symptoms that had already developed at the pre-hospital stage. The dynamics of psychopathological disorders demonstrated a close relationship with changes in the patients’ overall somatic condition.
5. Conclusions
Our clinical observations convincingly demonstrate that, under conditions of emotional stress in patients with gastric and duodenal cancer, there are no clearly demarcated boundaries between psychogenic and somatogenic reactions. The clinical picture of mental disorders was characterized by dynamic shifts—from predominantly reactive disturbances toward somatogenic disorders associated with deterioration of the somatic condition. This finding highlights the close interrelationship, variability, and dynamic nature of psychogenic and somatogenic factors.At the same time, based on the dominant clinical features of mental disorders, it is possible to assess the relative contribution of specific pathogenetic mechanisms. Accordingly, both in the preoperative period and at subsequent stages of treatment, a differentiated approach to the correction of mental disorders can be effectively implemented.Thus, during clinical follow-up, the transformation of psychopathological disorders was fully consistent with the results obtained using the Hamilton Depression Rating Scale (HDRS), Hamilton Anxiety Rating Scale (HAM-A), and Mini-Mult. Psychometric data objectively confirmed clinically observed astheno-depressive states, apathetic depression, and obsessive-phobic disorders, demonstrating that depressive and anxiety symptomatology was not purely reactive but largely associated with somatogenic mechanisms.This integrative approach indicates a progressive pattern in the formation of psychoorganic syndrome and provides a scientific basis for the necessity of comprehensive psychiatric and psychoprophylactic interventions during the course of clinical management.
References
| [1] | Yuri Alexandrovsky. Borderline Mental Disorders. Moscow: GEOTAR-Media; 2011. |
| [2] | Belozer A.S. Structure of mental disorders in oncological patients. Voprosy Onkologii. 2018; (3): 55–60. |
| [3] | Berezantsev A.Yu. Mental disorders in oncological diseases. Mental Health. 2017; (5): 32–38. |
| [4] | Veltishchev D.Yu. Mental disorders in oncology. Russian Psychiatric Journal. 2019; (4): 21–28. |
| [5] | Zozulya I.S. Mental disorders in oncological diseases. Bulletin of Psychiatry. 2019; (1): 37–42. |
| [6] | Krasnov V.N. Depressive disorders in general medical practice. S.S. Korsakov Journal of Neurology and Psychiatry. 2015; (4): 12–18. |
| [7] | Krivonis T.A., Levchenko V.A. Psychopathological symptoms in patients with oncological diseases. Bulletin of Psychiatry. 2020; (2): 41–48. |
| [8] | Krylov V.N. Mental disorders in cancer patients. Psychiatry and Psychopharmacotherapy. 2016; (2): 25–31. |
| [9] | Vladimir Mendelevich. Clinical Psychology. St. Petersburg: Piter; 2016. |
| [10] | Mosolov S.N., Kostyuk G.P. Depression in somatic diseases. Psychiatry and Psychopharmacotherapy. 2017; (3): 33–39. |
| [11] | Rumyantseva G.M. Psychoorganic Syndrome. Moscow: Medicine; 2012. |
| [12] | Anatoly Smulevich, Syrkin A.L. Psychosomatic Disorders. Moscow: MIA; 2015. |
| [13] | Strazhev S.V., Kuznetsov A.V. Psychosomatic aspects of oncological diseases. Medical Psychology in Russia. 2018; (4): 18–24. |
| [14] | Trunov A.N. Mental disorders in somatic diseases. Journal of Psychiatry. 2018; (2): 17–22. |
| [15] | Jarilkasinova G., Mukhamadiyeva N. Correlation analysis of clinical and dynamic features of psychopathological conditions of patients in a multidisciplinary hospital. BIO Web of Conferences. 2024; 121. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML