-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2277-2279
doi:10.5923/j.ajmms.20261605.12
Received: Feb. 10, 2026; Accepted: Mar. 3, 2026; Published: May 9, 2026

Surgical Treatment of Degenerative Spondylolisthesis by Transpedicular Correction with Fixation in Combination with PLIF Cages (Analysis of 109 Patients)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSattarov A. R., Rakhmanov Kh. M., Kobilov A. O., Abdiev Sh. E., Saidov S. S.
National Center of Rehabilitation and Prosthetics of Persons with Disabilities
Correspondence to: Sattarov A. R., National Center of Rehabilitation and Prosthetics of Persons with Disabilities.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Аim of the study to evaluate the clinical and radiographic efficacy of surgical treatment of degenerative spondylolisthesis using transpedicular correction and fixation in combination with PLIF cages. Materials and Methods. We analyzed the surgical outcomes of 109 patients with degenerative lumbar spondylolisthesis. All patients underwent posterior decompression, transpedicular correction, and fixation with interbody fusion using PLIF cages. Outcomes were assessed using clinical scores (VAS, ODI) and imaging data. Results. Most patients experienced a significant reduction in pain, improved functional status, and restoration of segmental stability. Interbody fusion formation was radiographically confirmed at long-term follow-up. Conclusion. The use of transpedicular correction with fixation in combination with PLIF cages is an effective and proven method for the surgical treatment of degenerative spondylolisthesis, providing a lasting clinical effect and reliable stabilization of the spinal segment.
Keywords: Degenerative spondylolisthesis, Transpedicular fixation, PLIF, Interbody fusion, Surgical treatment
Cite this paper: Sattarov A. R., Rakhmanov Kh. M., Kobilov A. O., Abdiev Sh. E., Saidov S. S., Surgical Treatment of Degenerative Spondylolisthesis by Transpedicular Correction with Fixation in Combination with PLIF Cages (Analysis of 109 Patients), American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2277-2279. doi: 10.5923/j.ajmms.20261605.12.
1. Introduction
- Degenerative spondylolisthesis is one of the most common causes of chronic low back pain in older patients. The disease develops due to degenerative changes in the intervertebral discs, facet joints, and ligaments, leading to vertebral displacement, spinal segment instability, and compression of neural structures.Conservative therapy is often ineffective, especially with progressive neurological symptoms and severe pain. Therefore, the search for optimal surgical techniques that ensure adequate decompression, restoration of anatomical relationships, and stable fixation of the affected segment remains urgent.One modern and widely used approach is transpedicular correction with fixation combined with posterior lumbar interbody fusion (PLIF) using cages. One of the main causes of spinal instability is degenerative-dystrophic diseases of the spine (DDSD). This is a polyetiological and multifactorial disease characterized by the degradation of the intervertebral discs, bone and ligamentous apparatus and manifested by various neurological, orthopedic and visceral disorders, and is a common pathology, especially in the elderly, and one of the most common causes of disability [1]. Surgical treatment of DDSD is currently a dynamically developing area of neurosurgery [2,3,4]. Thus, according to a report conducted by American marketing companies on the use of spinal implants [5], in 2015 it was estimated at 4.7 billion US dollars in 2015, and it is expected to grow to 5.6 billion dollars by 2020. Spinal fusion instrumentation represented the largest segment, accounting for approximately 57.4% of the total market, followed by dynamic stabilization devices (18.8%), systems for treating spinal compression fractures (vertebroplasty, kyphoplasty) (14.4%), and artificial cervical/lumbar discs (9.3%). The countries covered by this report included the top 5 markets in the European Union (France, Germany, Italy, Spain), Japan, and the United States. The indication for stabilization surgery is spinal instability, which can occur with isolated segmental hyperluxation, intervertebral disc herniations (often recurrent), degenerative stenosis, spondylosis, kyphoscoliosis, and other spinal disorders. The surgery involves installing an artificial prosthesis in the interdiscal space, followed by stabilization (in most cases, TPF). Spinal instability is generally understood to be the loss or absence of the ability of the spinal motion segment to maintain the midphysiological position of the vertebrae relative to each other at rest and during movement. It occurs as a stage in the development of degenerative-dystrophic processes in the spine and intervertebral disc [6]. Functional radiographs reveal a displacement of the vertebral bodies of more than 4 mm (anteroposterior or lateral) or an angular displacement of more than 10° compared to adjacent levels [7]. Most authors agree that instability is a complex of clinical manifestations and radiographic changes [8,9]. Surgical interventions for spinal instability consist of joining the vertebral bodies (spondylodesis) and include the following types: 1) Posterior (PLIF - posterior interbody fusion). 2) Posterolateral (TLIF - Transforaminal Interbody Fusion). 3) Lateral (XLIF, DLIF, LLIF - Extreme or Lateral Interbody Fusion). 4) Anterior-lateral (OLIF - Oblique Lateral Interbody Fusion). 5) Anterior (ALIF - Anterior Lumbar Interbody Fusion).There is no clear, convincing evidence that one approach is superior to another in terms of fusion or clinical outcomes. In general, traditional posterior approaches are used more frequently due to the availability of a technique that can produce satisfactory fusion late after surgery. However, they are limited by the presence of dural sac and nerve root retraction factors, along with iatrogenic damage to the paraspinal muscles. Minimally invasive (MIS) approaches have been developed in an attempt to reduce these neurological complications [10,11].
2. Materials and Methods
- The study included 109 patients diagnosed with degenerative lumbar spondylolisthesis who underwent surgical treatment. Among them, the majority were able-bodied and elderly patients. The gender ratio was as follows: 80 women and 29 men, respectively. The patients' ages ranged from 23 to 71 years, with an average age of 43.2±1.6 years. The main indications for surgery were:• persistent pain syndrome refractory to conservative therapy;• progressive neurological Symptoms;• Clinically and radiographically confirmed segmental instability.Preoperative evaluation included a clinical examination, radiography with functional tests, CT, and MRI. Pain was assessed using the visual analogue scale (VAS), and functional impairment was assessed using the Oswestry Disability Index (ODI).Surgery was performed through a posterior approach and included decompression of neural structures, placement of pedicle screws, correction of vertebral displacement, and interbody fusion using PLIF cages filled with bone autograft.
3. Results
- In the early postoperative period, most patients experienced a significant reduction in pain. According to the VAS scale, a significant reduction in pain intensity was observed, and ODI scores indicated an improvement in quality of life and functional activity.Radiographic examination confirmed adequate correction of vertebral displacement and restoration of sagittal balance. In the long-term follow-up Over the course of the follow-up period, a reliable interbody bone block was formed in the majority of patients, indicating the effectiveness of the fusion.The complication rate was minimal and did not exceed data presented in the current literature. Figure 1 shows VL4 spondylolisthesis before and after surgery.
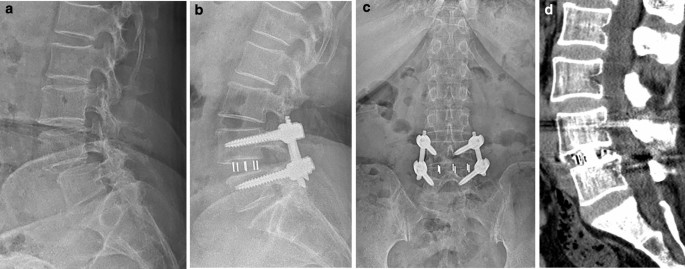 | Figure 1. Patient C, 43, with degenerative VL4 spondylolisthesis. Before operation Xray picture, after operation Xray picture and CT picture, short-term stabilization at the VL4-5 level with the TPF system and peek cage fusion |
4. Discussion
- The obtained results confirm the high efficacy of combining transpedicular fixation and PLIF cages in the treatment of degenerative spondylolisthesis. This method allows for the simultaneous achievement of several key objectives: decompression of neural structures, restoration of anatomical relationships, and provision of stable fixation of the spinal segment.Comparison with other surgical treatment methods shows that interbody fusion Spinal fusion using cages promotes faster bone block formation and reduces the risk of postoperative instability.
5. Conclusions
- Surgical treatment of degenerative spondylolisthesis using transpedicular correction with fixation in combination with PLIF cages is an effective and safe method.The use of this technique in 109 patients demonstrated good clinical and radiographic results, allowing it to be recommended for widespread use in clinical practice.