-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2273-2276
doi:10.5923/j.ajmms.20261605.11
Received: Apr. 15, 2026; Accepted: May 7, 2026; Published: May 9, 2026

Early Diagnosis of Hyperandrogenism Syndrome Based on Hormonal and Ultrasound Indicators
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSaidova Gavxaroy Olimovna1, Nadjmitdinov Otabek Bakhritdin ugli2
1Independent Researcher, Department of Obstetrics and Gynecology, Andijan State Medical Institute, Andijan, Uzbekistan
2Head of the Department of Medical Radiology, Interventional Cardiology, Nephrology-Hemodialysis and Clinical and Laboratory Diagnostics, Andijan State Medical Institute, Andijan, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Hyperandrogenism (HA) is a common endocrine disorder affecting women of reproductive age and is associated with infertility, menstrual dysfunction, and metabolic disturbances. According to epidemiological data, its prevalence ranges from 5–15% in the general population and up to 40% among women with anovulatory infertility. The purpose of this study is to improve early diagnostic approaches for hyperandrogenism using hormonal and ultrasound indicators. The study included women aged 18–30 years with different forms of HA. Hormonal analysis included testosterone, DHEA-S, LH, FSH, prolactin, thyroid hormones, and SHBG levels, while ultrasound was used to assess ovarian morphology. The results showed that patients with manifest HA had significantly elevated androgen levels and LH/FSH ratio, along with characteristic ovarian changes such as increased volume and multiple follicles. In contrast, latent HA presented with mild hormonal and structural alterations, making diagnosis more challenging. The findings suggest that a combined diagnostic approach integrating hormonal and ultrasound parameters significantly improves early detection and differential diagnosis of hyperandrogenism.
Keywords: Hyperandrogenism, Hormones, Ultrasound diagnostics, PCOS, Infertility
Cite this paper: Saidova Gavxaroy Olimovna, Nadjmitdinov Otabek Bakhritdin ugli, Early Diagnosis of Hyperandrogenism Syndrome Based on Hormonal and Ultrasound Indicators, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2273-2276. doi: 10.5923/j.ajmms.20261605.11.
1. Introduction
- Hyperandrogenism is one of the most common endocrine disorders affecting women of reproductive age and represents a significant medical and social problem due to its close association with infertility, menstrual dysfunction, metabolic disturbances, and decreased quality of life [1,5,8]. Epidemiological studies indicate that hyperandrogenism occurs in approximately 5–15% of women in the general population and accounts for up to 40% of cases of anovulatory infertility [11,14]. Furthermore, according to data from the World Health Organization, endocrine-related infertility linked to androgen excess reaches 46-77%, while early pregnancy loss is observed in 21–32% of affected women [2,5,9].The pathophysiology of hyperandrogenism is complex and involves dysregulation at multiple levels of the endocrine system, particularly within the hypothalamic–pituitary–ovarian axis. Increased secretion of luteinizing hormone stimulates ovarian theca cells, leading to excessive androgen production, which disrupts normal follicular development and ovulation. In addition to ovarian mechanisms, adrenal hyperandrogenism and peripheral androgen metabolism also contribute to the development of the syndrome, reflecting its heterogeneous nature. In clinical practice, hyperandrogenism is most commonly associated with polycystic ovary syndrome, which accounts for the majority of cases and is characterized by a combination of hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology [3,6,12].Despite substantial progress in understanding the etiology and pathogenesis of hyperandrogenism, early diagnosis remains a major challenge. This is primarily due to the variability of clinical manifestations, ranging from pronounced symptoms such as hirsutism, acne, and menstrual irregularities to latent forms with minimal or nonspecific signs. In such cases, standard diagnostic approaches based solely on clinical presentation may lead to underdiagnosis or delayed identification of the condition. Moreover, hormonal parameters may fluctuate within borderline ranges, and ultrasound findings may not always meet classical diagnostic criteria, particularly in early stages of the disease.Another important issue is the lack of a unified diagnostic algorithm capable of accurately differentiating between ovarian, adrenal, and mixed forms of hyperandrogenism. This differentiation is essential for selecting appropriate treatment strategies, as the underlying mechanisms and therapeutic approaches differ significantly depending on the origin of androgen excess. Therefore, there is a growing need for integrated diagnostic approaches that combine hormonal, biochemical, and imaging data to improve diagnostic accuracy.In this context, the use of combined hormonal profiling and ultrasound examination represents a promising direction for early detection of hyperandrogenism. Hormonal indicators such as testosterone, DHEA-S, LH/FSH ratio, and SHBG provide insight into endocrine dysfunction, while ultrasound imaging allows visualization of structural ovarian changes that reflect underlying pathophysiological processes.Therefore, the aim of the present study is to improve the early diagnosis of hyperandrogenism by evaluating the diagnostic value of hormonal and ultrasound indicators and by developing a more comprehensive and clinically applicable diagnostic approach.
2. Materials and Methods
- This study was conducted between 2023 and 2025 at the Andijan regional branch of the Republican Specialized Scientific and Practical Medical Center “Mother and Child.” A total of 120 women aged 18–30 years diagnosed with various forms of hyperandrogenism were included in the study.A comprehensive diagnostic approach was applied, including clinical, laboratory, and instrumental methods. Hormonal evaluation included measurement of total testosterone, DHEA-S, androstenedione, luteinizing hormone, follicle-stimulating hormone, prolactin, thyroid-stimulating hormone, triiodothyronine, thyroxine, and sex hormone-binding globulin. Ultrasound examination of pelvic organs was performed to assess ovarian volume, follicular number, and stromal structure.Statistical analysis was carried out using correlation and comparative methods, with significance set at p<0.05.
3. Results and Discussion
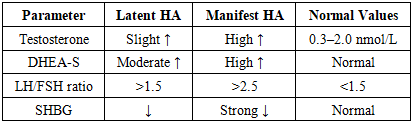
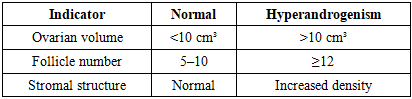
- The analysis of clinical, hormonal, and ultrasound data obtained in this study confirms that hyperandrogenism is characterized by significant endocrine imbalance accompanied by structural changes in the ovaries. A comparative evaluation of patients with latent and manifest forms of hyperandrogenism revealed statistically significant differences in key hormonal parameters. In particular, patients with manifest hyperandrogenism demonstrated markedly elevated levels of total testosterone and DHEA-S, reflecting increased androgen production from both ovarian and adrenal sources. At the same time, a significant increase in the LH/FSH ratio was observed, indicating dysregulation of the hypothalamic–pituitary–ovarian axis and a predominance of luteinizing hormone activity.A decrease in sex hormone-binding globulin (SHBG) levels was identified in both groups, with a more pronounced reduction in patients with manifest forms of hyperandrogenism. This finding is of particular clinical importance, as SHBG plays a key role in regulating the bioavailability of circulating androgens. Reduced SHBG levels lead to an increase in free, biologically active testosterone, thereby enhancing clinical manifestations of hyperandrogenism even when total testosterone levels are only moderately elevated. This mechanism may explain the discrepancy between laboratory values and clinical symptoms observed in certain patients.Ultrasound examination provided additional evidence of structural ovarian changes associated with hyperandrogenism. In patients with manifest forms, a significant increase in ovarian volume and the presence of multiple small antral follicles were observed, often arranged peripherally, forming the typical polycystic ovarian morphology. Increased stromal echogenicity was also detected, reflecting stromal hyperplasia and enhanced androgen-producing activity of theca cells. In contrast, patients with latent hyperandrogenism demonstrated less pronounced changes, including borderline increases in follicle number and mild enlargement of ovarian volume. These findings suggest that morphological alterations develop progressively and are closely associated with the severity of hormonal imbalance.
|
|
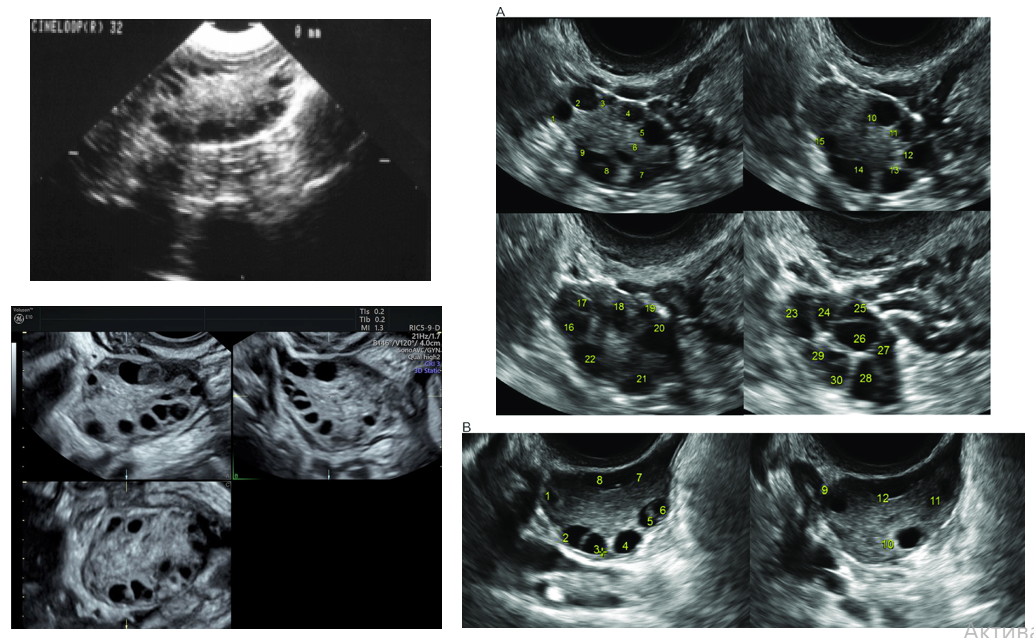 | Figure 1. Ultrasound Features of Polycystic Ovaries |
4. Conclusions
- The present study confirms that hyperandrogenism is a complex, multifactorial endocrine disorder in which hormonal imbalance plays a central role in disrupting reproductive function. Elevated levels of circulating androgens, particularly testosterone and DHEA-S, in combination with altered gonadotropin secretion (increased LH/FSH ratio), reflect significant dysregulation of the hypothalamic–pituitary–ovarian axis. These hormonal disturbances directly contribute to impaired folliculogenesis, anovulation, and subsequent infertility [4,7,15].The findings demonstrate that ultrasound examination provides essential complementary diagnostic information by revealing characteristic structural changes in the ovaries, including increased ovarian volume, multiple small follicles, and enhanced stromal echogenicity. These features are particularly pronounced in patients with manifest forms of hyperandrogenism and are consistent with polycystic ovary morphology.Importantly, the study highlights that latent forms of hyperandrogenism may present with only mild hormonal deviations and subtle ultrasound findings, which often remain undetected in routine clinical practice. This underlines the necessity of applying an integrated diagnostic approach that combines detailed hormonal profiling with high-resolution ultrasound assessment.The correlation analysis confirms a strong interrelationship between endocrine and structural parameters, suggesting that neither hormonal nor imaging indicators alone are sufficient for accurate diagnosis. Instead, their combined evaluation significantly increases diagnostic sensitivity and specificity, especially in early-stage or subclinical cases [10,13].From a clinical perspective, the proposed diagnostic approach allows for earlier identification of patients at risk of reproductive dysfunction, enabling timely therapeutic intervention and improving reproductive outcomes. Furthermore, it provides a basis for individualized treatment strategies tailored to the underlying pathophysiological mechanisms of hyperandrogenism.In conclusion, the integration of hormonal and ultrasound diagnostics represents a reliable and effective method for the early detection and differential diagnosis of hyperandrogenism. Future research should focus on refining diagnostic algorithms, incorporating additional biomarkers, and evaluating long-term clinical outcomes associated with early intervention strategies.