-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2754-2759
doi:10.5923/j.ajmms.20261605.101
Received: Apr. 15, 2026; Accepted: May 17, 2026; Published: May 30, 2026

Morphological and Immunohistochemical Features of Chronic Inflammation in the Breast
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRavshanova Nasiba Berdiyevna1, Shakirov Sardor Abdusaminovich2
1Independent Researcher, Fergana Medical Institute of Public Health, Fergana, Uzbekistan
2PhD., Associate Professor, Department of Pathological Physiology and Pathological Anatomy, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Ravshanova Nasiba Berdiyevna, Independent Researcher, Fergana Medical Institute of Public Health, Fergana, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Chronic inflammatory breast lesions are diagnostically challenging because they may mimic neoplastic disease and overlap with age-related tissue remodeling. Objective: To characterize the morphological and immunohistochemical features of chronic breast inflammation and assess their relationship to proliferative activity, local immune response, and cell-cycle regulation. Methods: The study included 63 breast tissue specimens: 13 morphologically normal controls and 50 cases of chronic inflammation. Histology, histochemistry, morphometry, and immunohistochemistry for Ki-67, CD45, and p53 were performed. Results: Chronic inflammation was associated with lymphoplasmacytic infiltration, stromal fibrosis, distortion of ductolobular structures, and reactive epithelial changes. Histochemistry demonstrated connective tissue remodeling and collagen condensation. Immunohistochemically, chronic inflammation showed lower Ki-67 expression, markedly higher CD45 expression, and no sharp increase in p53 compared with normal tissue. Conclusions: Chronic breast inflammation is characterized by coordinated epithelial, stromal, and immune-cellular remodeling. Combined morphological and immunohistochemical assessment improves the differential interpretation of biopsy and operative material and helps distinguish chronic inflammation from age-related involution.
Keywords: Breast, Chronic inflammation, Pathology, Histochemistry, Morphometry, Immunohistochemistry, Ki-67, CD45, p53, Fibrosis, Tissue remodeling
Cite this paper: Ravshanova Nasiba Berdiyevna, Shakirov Sardor Abdusaminovich, Morphological and Immunohistochemical Features of Chronic Inflammation in the Breast, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2754-2759. doi: 10.5923/j.ajmms.20261605.101.
1. Introduction
- Chronic inflammatory processes of the breast occupy an intermediate diagnostic position between purely reactive lesions and tissue changes that may simulate tumor-like growth. [1,4,5] In routine pathology practice, these lesions are challenging because stromal sclerosis, lymphoplasmacytic infiltration, architectural distortion, epithelial reactivity, and focal macrophage-rich areas may mimic proliferative or even neoplastic processes on both imaging and histologic examination. [14,15,16]To address this diagnostic challenge, the present study integrates routine microscopy with histochemistry, cytomorphometry, digital morphometry, and immunohistochemistry. [2] From a morphobiological perspective, chronic inflammation should not be regarded as a simple infiltrative event. Rather, it represents a prolonged and spatially heterogeneous remodeling process involving epithelial injury and repair, extracellular matrix reorganization, microcirculatory alterations, and a persistent local immune response. [3,6,17]This issue is relevant not only to the diagnosis of benign breast disease but also to the broader pathology of tissue remodeling associated with carcinogenesis-related microenvironments. Sustained inflammation may create a biologically active tissue background characterized by cytokine signaling, matrix remodeling, and altered balance between proliferation and regeneration. At the same time, chronic inflammatory lesions should not be interpreted as direct evidence of malignant transformation. [7,8,9] Careful morphologic and immunohistochemical evaluation is therefore required to avoid both underdiagnosis and overdiagnosis. [12]The aim of the present study was to characterize chronic inflammatory lesions of the breast with particular emphasis on histologic architecture, histochemical matrix alterations, representative morphometric patterns, and the expression profiles of Ki-67, CD45, and p53. [10,13]
2. Materials and Methods
- This comparative descriptive-analytical study was performed on breast tissue specimens obtained from biopsy material, surgical samples, and archival paraffin blocks. The total study cohort comprised 63 cases, including 13 morphologically normal or near-normal control specimens and 50 cases with clinicopathologically verified chronic inflammatory processes of the breast.To account for the confounding effect of age-related involution, the material was stratified into two age groups: 30–35 years and 35–65 years. The primary comparative statistical analysis was focused on the 30–35-year subgroup, as this interval minimized involutional and hormonal influences and allowed a more accurate interpretation of inflammation-associated epithelial and stromal alterations. The 35–65-year subgroup was used for descriptive analysis of age-related changes.
|

|

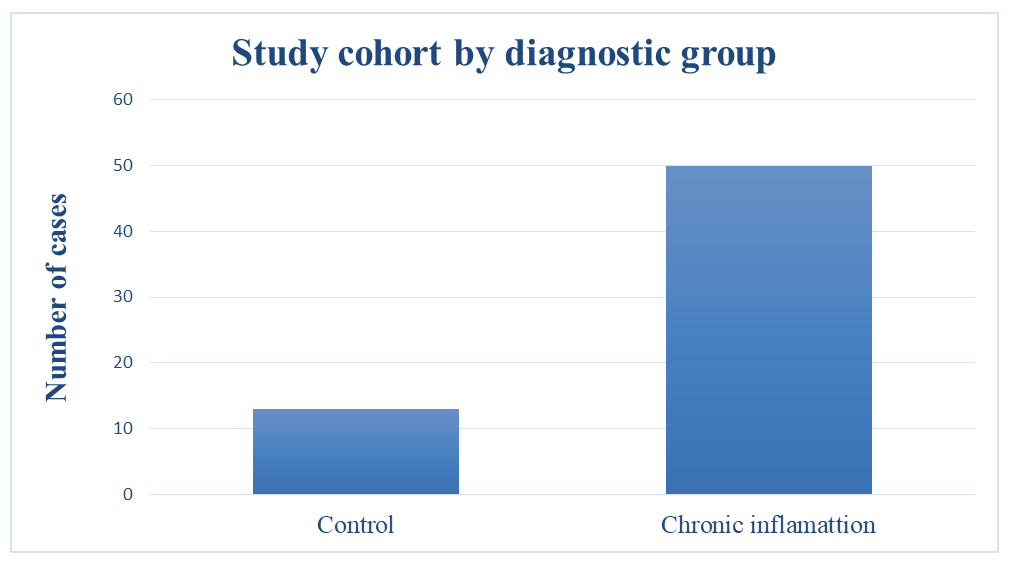 | Figure 1. Distribution of the study cohort by diagnostic group |
3. Results
- A total of 63 cases were analyzed, including 13 controls and 50 chronic inflammatory lesions. Twelve of the 13 control cases belonged to the 30-35-year age group, whereas one control case and 25 chronic inflammatory cases belonged to the 35-65-year age group. Accordingly, the principal comparative design emphasized the younger age stratum, while the older cases provided an additional descriptive framework for assessing the interaction between chronic inflammation and involutional change.
|
|

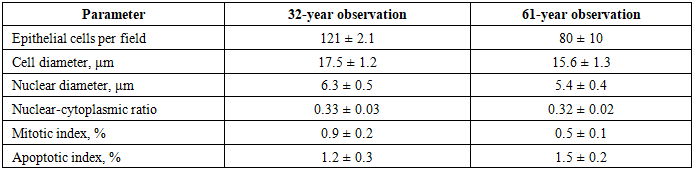
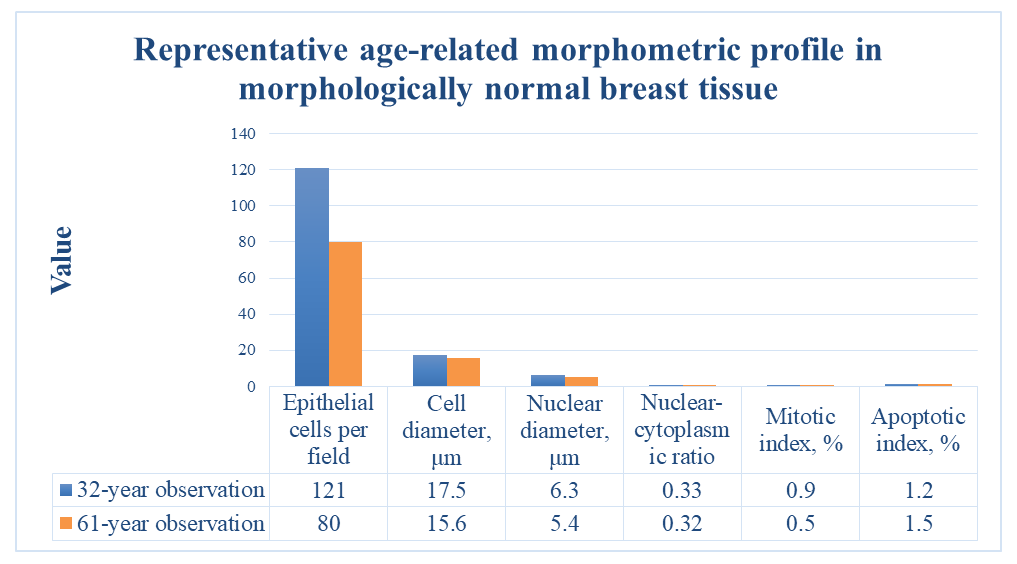 | Figure 2. Representative age-related morphometric profile in morphologically normal breast tissue |
|
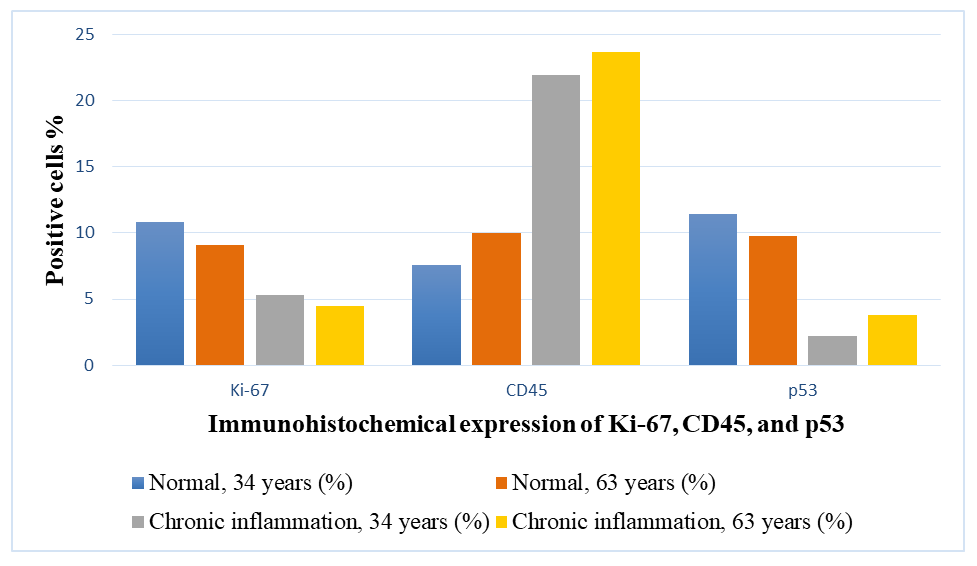 | Figure 3. Comparative immunohistochemically expression of Ki-67, CD45, and p53 in normal breast tissue and chronic inflammation |
4. Discussion
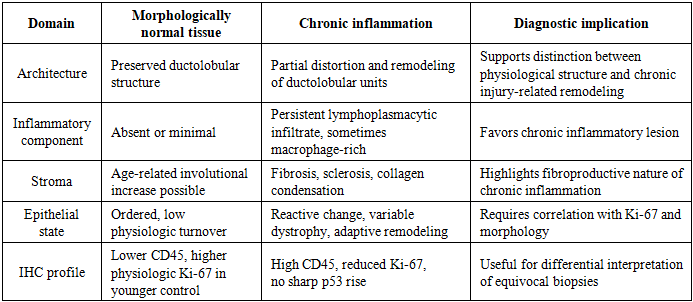
- The present analysis supports the view that chronic breast inflammation should be interpreted as a complex morphobiological process combining persistent inflammatory activity, reparative remodeling, epithelial adaptation, and progressive stromal fibrosis. This interpretation is important because the histologic appearance of chronic inflammatory lesions may overlap both with involutional changes and with lesions that raise concern for neoplasia.One of the central findings of the study is the distinction between inflammation-related remodeling and physiologic involution. In morphologically normal tissue, aging was associated primarily with reduced epithelial cellularity and functional activity, accompanied by relative stromal expansion. In chronic inflammation, however, the remodeling pattern included persistent mononuclear infiltration, fibrosclerosis, reorganization of ductolobular units, and a more heterogeneous cytomorphometric profile. These observations indicate that age alone cannot account for the architectural and cellular alterations seen in inflamed tissue.The histochemical findings further refine this distinction. Redistribution of PAS-positive material and increased collagen condensation on Van Gieson staining indicate that chronic inflammation is accompanied by matrix-level and basement membrane-associated alterations. These changes are consistent with a tissue microenvironment in which injury, repair, fibrosis, and altered epithelial-stromal interaction occur simultaneously. From a diagnostic perspective, such findings may be misinterpreted if evaluation relies on routine histology alone, particularly in small biopsy specimens.The immunohistochemical profile adds an additional biologically coherent layer of interpretation. Lower Ki-67 expression in chronically inflamed tissue suggests that the dominant process in these lesions is not excessive epithelial proliferation, but rather structural remodeling with limited regenerative turnover. This observation is of particular importance because reactive lesions might be expected to show increased proliferative activity, whereas the present data indicate that prolonged inflammation may instead be associated with a constrained proliferative state.By contrast, markedly increased CD45 expression confirms that chronic inflammatory lesions remain immunologically active even when epithelial proliferation is relatively low. The combination of reduced Ki-67 and increased CD45 represents one of the most informative patterns identified in the study. This profile helps distinguish chronic inflammatory lesions from processes in which epithelial expansion is the dominant morphologic feature and underscores the diagnostic importance of evaluating inflammatory-cell architecture in addition to epithelial morphology.The p53 findings require cautious interpretation. In the analyzed material, p53 expression did not show a marked increase in chronic inflammatory lesions. This does not exclude stress-related signaling or localized regulatory disturbances, but it suggests that widespread overt p53-associated dysregulation was not a dominant feature in the studied cases. Accordingly, p53 should be regarded as a contextual marker that is most informative when interpreted in conjunction with morphologic and proliferative features rather than as an isolated indicator of preneoplastic transformation.Taken together, these findings support a practical diagnostic approach to chronic breast inflammation. First, the overall architecture and inflammatory pattern should be assessed on routine histology. Second, matrix remodeling and fibrosis should be further characterized using histochemical methods. Third, morphometric and cytomorphometric parameters, when available, may help objectify epithelial and stromal alterations. Fourth, a focused immunohistochemical panel including Ki-67, CD45, and p53 may be applied in diagnostically difficult cases. Such a layered approach may improve the standardization of pathology reporting and reduce interpretive ambiguity in biopsy and operative material.
5. Conclusions
- Chronic inflammatory processes in the breast are characterized by a reproducible constellation of pathomorphological changes, including mononuclear inflammatory infiltration, stromal fibrosis and sclerosis, architectural remodeling of ductolobular units, and reactive epithelial alterations.Histochemical techniques, particularly the periodic acid–Schiff (PAS) reaction and Van Gieson staining, provide diagnostically valuable information on basement membrane-associated changes, connective tissue remodeling, and collagen condensation, thereby complementing routine histologic evaluation.Morphometric and cytomorphometric analyses facilitate differentiation between inflammation-related remodeling and age-associated involution by objectively assessing epithelial cellularity, nuclear parameters, proliferative–apoptotic balance, and structural variability.The immunohistochemical profile characterized by reduced Ki-67 expression, increased CD45 expression, and the absence of marked p53 elevation supports the interpretation of chronic inflammation as a process dominated by immune-cellular activation and tissue remodeling rather than by overt dysregulated epithelial proliferation.An integrated morphological approach is therefore recommended for the differential diagnosis of chronic inflammatory breast lesions in biopsy and surgical specimens, particularly in cases where clinical or radiologic findings raise concern for neoplasia.