-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2269-2272
doi:10.5923/j.ajmms.20261605.10
Received: Apr. 12, 2026; Accepted: May 6, 2026; Published: May 9, 2026

Comparative Analysis of Maternal Hemodynamics, Renal Function Biomarkers and Uteroplacental Doppler Indices in Isolated Preeclampsia Versus Preeclampsia Superimposed on Pre-existing Arterial Hypertension
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDilfuza F. Najmetdinova1, Mastura N. Negmatullaeva2
1Doctoral Candidate, Republican Specialized Scientific-Practical Medical Center for Maternal and Child Health, Tashkent, Uzbekistan
2DSc. Professor, Department of Obstetrics and Gynecology No. 2, Bukhara State Medical Institute named after Abu Ali ibn Sino, Bukhara, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Preeclampsia (PE) that develops against a background of pre-existing arterial hypertension represents one of the most severe variants of hypertensive disorders of pregnancy and remains a leading cause of adverse maternal and perinatal outcomes. The present work compares key parameters of maternal central hemodynamics, serum biomarkers of renal function and Doppler indices of the uteroplacental and fetal circulation in four groups of pregnant women examined at 30–34 weeks of gestation: a control cohort with physiological pregnancy (n=50), pregnant women with isolated moderate PE (n=50), pregnant women in whom PE was superimposed on chronic arterial hypertension (CAH, n=15) and those with PE superimposed on gestational arterial hypertension (GAH, n=10). The results demonstrated that the highest total peripheral vascular resistance was recorded in patients with PE on CAH (1501±40 dyn·s·cm⁻⁵), while the most pronounced elevation of serum cystatin-C (1.12±0.26 mg/L, +103.6 % compared with control) and microalbuminuria (54.1±4.8 µg/mL) were detected in the isolated PE group. Doppler evaluation revealed that the uterine artery systole-to-diastole ratio reached its maximum in the PE on CAH subgroup (2.81±0.04), exceeding control values by 61.5 %. These findings indicate that the pathophysiological burden of PE on CAH is primarily driven by sustained vascular resistance, whereas isolated PE shows more prominent renal biomarker disturbances. Incorporation of cystatin-C and microalbuminuria into routine assessment of pregnant women with hypertensive disorders may therefore provide an additional tool for risk stratification and management individualization.
Keywords: Preeclampsia, Superimposed preeclampsia, Chronic arterial hypertension, Gestational hypertension, Cystatin-C, Microalbuminuria, Doppler ultrasonography, Central hemodynamics
Cite this paper: Dilfuza F. Najmetdinova, Mastura N. Negmatullaeva, Comparative Analysis of Maternal Hemodynamics, Renal Function Biomarkers and Uteroplacental Doppler Indices in Isolated Preeclampsia Versus Preeclampsia Superimposed on Pre-existing Arterial Hypertension, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2269-2272. doi: 10.5923/j.ajmms.20261605.10.
1. Introduction
- Hypertensive disorders complicate 5–12 % of pregnancies worldwide and account for approximately 14–18 % of maternal deaths. Preeclampsia (PE) is considered the most dangerous clinical form of this group, and its occurrence on the background of already existing arterial hypertension creates a particularly adverse clinical scenario [1,2]. When PE is superimposed on chronic arterial hypertension (CAH) or on gestational arterial hypertension (GAH), the risk of organ dysfunction, placental insufficiency and preterm delivery increases substantially — the probability of severe fetal growth restriction in such patients reaches three to four times the rate observed in isolated PE [3,4].The pathophysiological basis of PE involves generalised endothelial dysfunction, imbalance of angiogenic factors, elevated vascular resistance and progressive renal hypoperfusion. In women with pre-existing hypertension these mechanisms engage upon a vascular bed already modified by long-standing elevated blood pressure and endothelial remodeling, resulting in a distinct and often more severe clinical pattern [5,6]. Nevertheless, in routine obstetric practice the differentiation between isolated PE and superimposed PE still relies predominantly on clinical criteria (blood pressure, proteinuria) and does not account for subclinical shifts in maternal central hemodynamics or early biomarkers of renal impairment.Recent studies have highlighted cystatin-C, microalbuminuria and Doppler-derived flow indices as potential early indicators of maternal organ involvement in hypertensive disorders [7,8]. However, comparative data on these parameters in different forms of PE — isolated versus superimposed on CAH or GAH — remain limited, particularly with respect to Central Asian populations. The present study was therefore designed to analyse maternal hemodynamic, renal and Doppler parameters in a well-defined clinical cohort and to identify differences between isolated and superimposed forms of PE.
2. Material and Methods
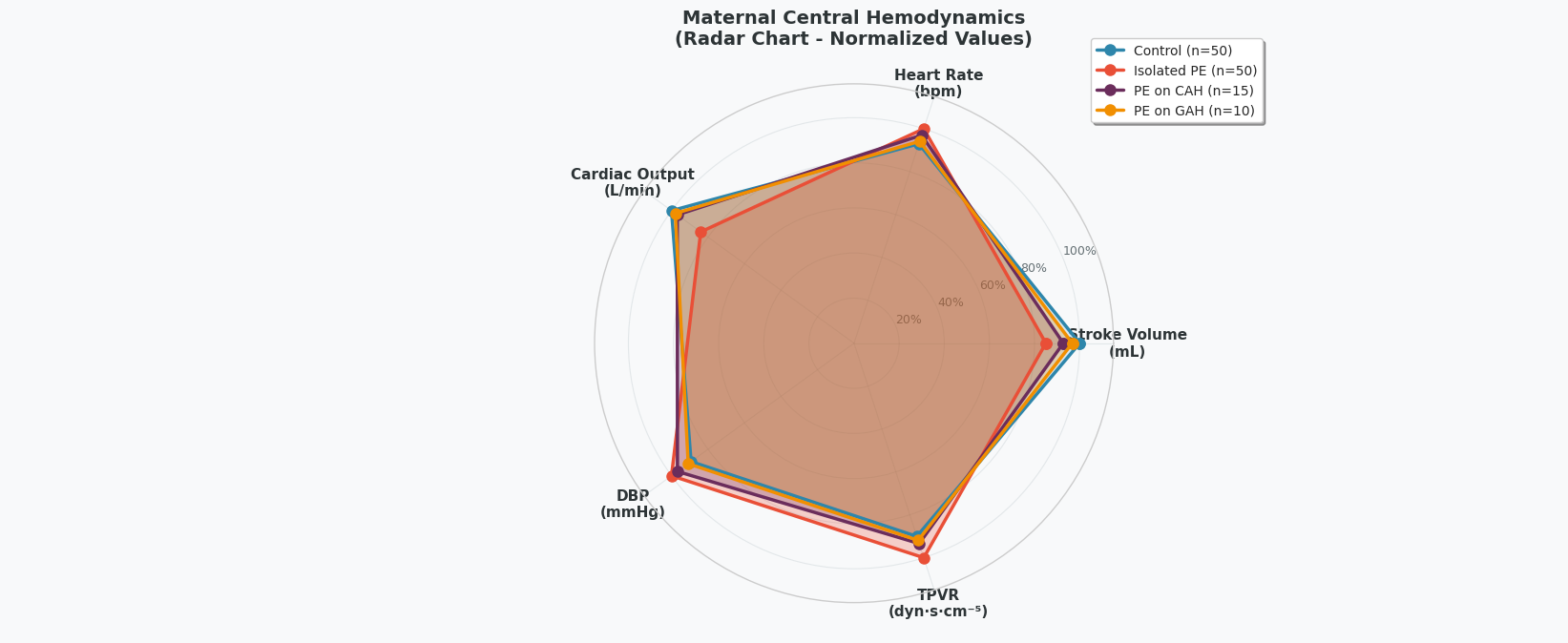
- The present open, prospective, comparative cohort study was carried out between February 2023 and April 2025 at the clinical bases of the Department of Obstetrics and Gynecology No. 2 of the Bukhara State Medical Institute named after Abu Ali ibn Sino (Bukhara, Uzbekistan) and the Republican Specialized Scientific-Practical Medical Center for Maternal and Child Health (Tashkent, Uzbekistan). The study included 125 pregnant women aged 19 to 42 years (mean age 29.6±3.8 years) examined at 30–34 weeks of gestation, and was approved by the ethical committees of both institutions prior to its initiation. Written informed consent was obtained from each participant.Participants were allocated to four clinically defined groups. The control group (n=50) comprised women with uncomplicated gestation. The isolated PE group (n=50) included pregnant women in whom moderate PE developed against a background of normal blood pressure before pregnancy. Two further groups represented superimposed PE: PE on CAH (n=15) and PE on GAH (n=10). The diagnosis of PE and its superimposition were established in accordance with the ISSHP 2022 classification and the clinical protocols of the Ministry of Health of the Republic of Uzbekistan. Exclusion criteria comprised multiple pregnancy, antiphospholipid syndrome, diabetes mellitus, systemic connective tissue disorders, and fetal malformations.Central maternal hemodynamic parameters — stroke volume (SV), stroke index (SI), heart rate (HR), cardiac output (CO), total peripheral vascular resistance (TPVR) and diastolic blood pressure (DBP) — were determined by impedance cardiography and Doppler echocardiography. Renal function was evaluated using serum creatinine, urea, cystatin-C (immunoturbidimetric assay) and 24-hour urinary microalbumin (MAU), with glomerular filtration rate estimated by the Hoek formula. Uteroplacental and fetal circulation was assessed by Doppler ultrasonography in the maternal renal artery, uterine artery, umbilical artery, fetal aorta and fetal middle cerebral artery, with calculation of the systole-to-diastole (S/D) ratio and resistance index (RI).Data processing was performed using IBM SPSS Statistics 26.0 and MedCalc 20.0. Continuous variables are presented as mean ± standard deviation (M±m). Intergroup comparisons used Student's t-test, Mann-Whitney U-test and one-way ANOVA with Bonferroni correction as appropriate. A p-value less than 0.05 was considered statistically significant.Comparative analysis of central maternal hemodynamics (Picture 1) revealed distinct patterns across the four groups. In women with isolated PE, stroke volume was reduced to 70.4±1.6 mL (−14.9 % versus control, p<0.0001), heart rate was elevated to 94.0±1.4 beats per minute (+7.6 %, p<0.0001), and cardiac output decreased to 6.08±0.23 L/min. Diastolic blood pressure reached 95.2±2.3 mmHg and total peripheral vascular resistance rose to 1501.2±51.1 dyn·s·cm⁻⁵ (+11.0 % above control). In contrast, in women with PE superimposed on CAH, the reduction of stroke volume was less pronounced (76.8±1.7 mL), whereas TPVR remained considerably elevated at 1401.5±40.1 dyn·s·cm⁻⁵, reflecting the persistent baseline vascular constriction inherent to this subgroup. In PE superimposed on GAH, hemodynamic alterations were least marked, with stroke volume (80.1±2.3 mL) and DBP (86.5±2.6 mmHg) approaching control values.
 | Picture 1 |
 | Picture 2 |
 | Picture 3 |
3. Conclusions
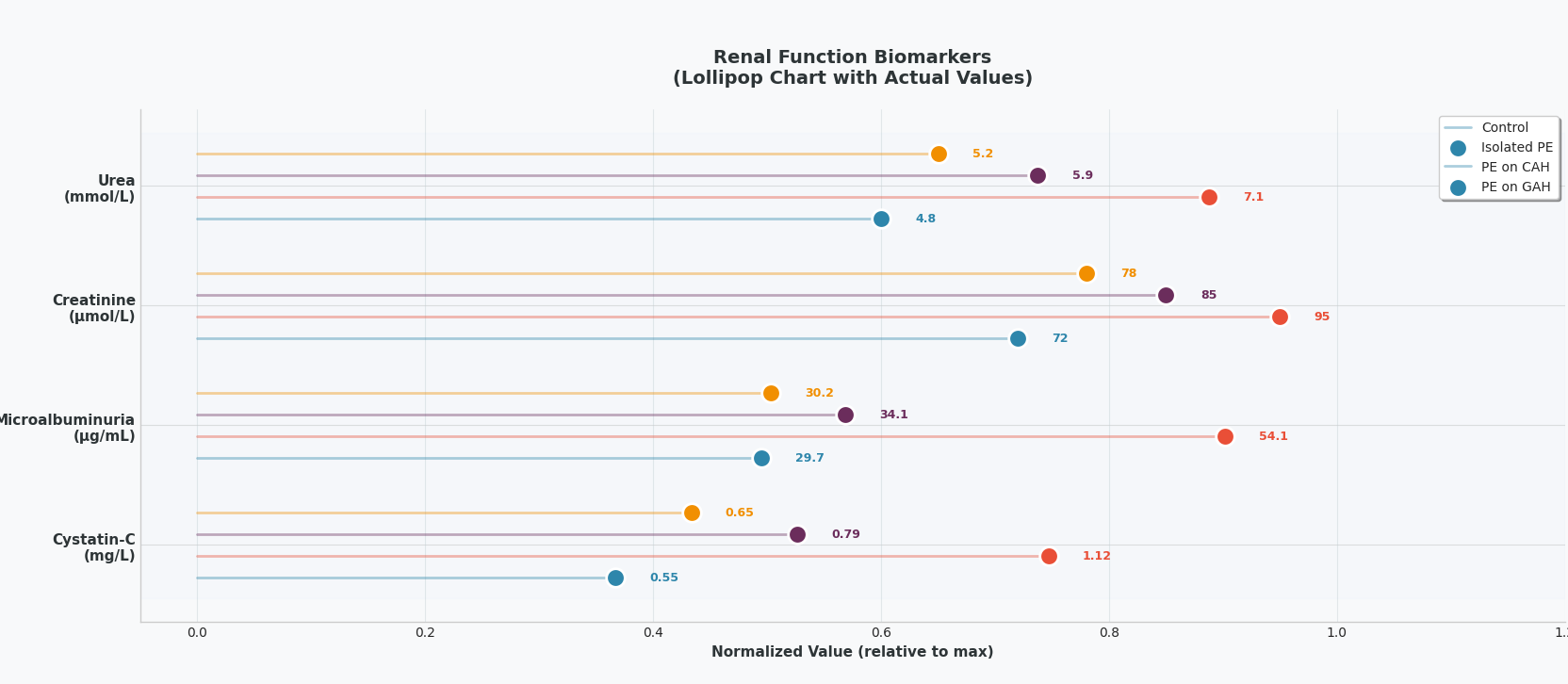
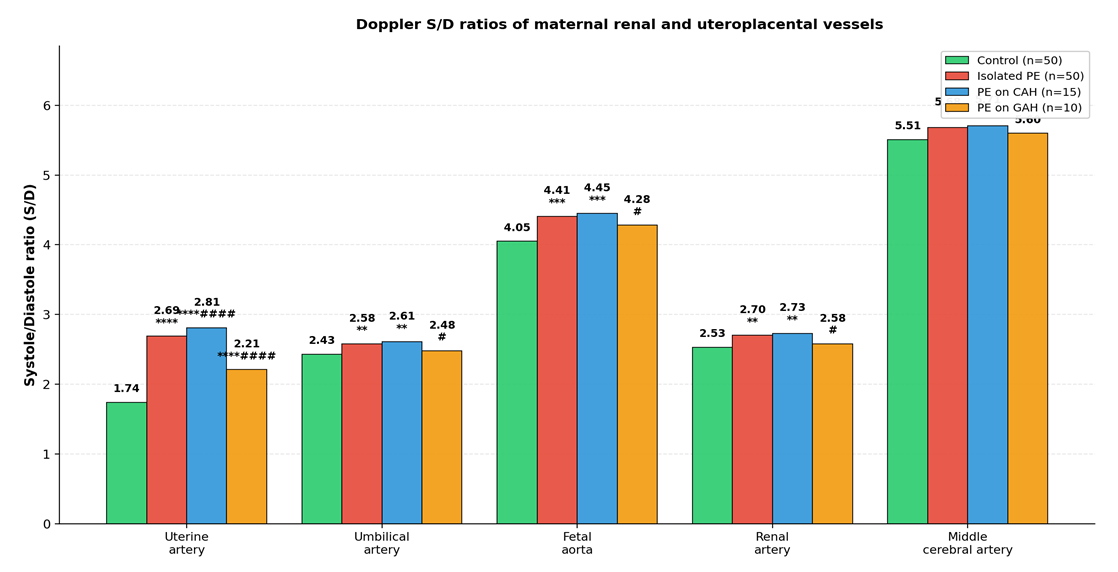
- 1. Maternal central hemodynamic, renal and Doppler parameters demonstrate clinically meaningful differences between isolated PE and PE superimposed on pre-existing arterial hypertension. The most pronounced elevation of total peripheral vascular resistance (1501±40 dyn·s·cm⁻⁵) and uterine artery S/D ratio (2.81±0.04) was recorded in women with PE superimposed on chronic arterial hypertension.2. Cystatin-C and microalbuminuria proved more sensitive markers of renal involvement than creatinine and urea in all hypertensive subgroups; the highest absolute values of both biomarkers were observed in isolated PE (cystatin-C 1.12±0.26 mg/L; MAU 54.1±4.8 µg/mL), reflecting acute glomerular endothelial disruption.3. Integrated evaluation of cystatin-C, microalbuminuria and Doppler indices improves differentiation between clinical forms of PE and may be incorporated into standard antenatal monitoring of pregnant women with hypertensive disorders to support earlier decision-making and individualized management.