-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2260-2268
doi:10.5923/j.ajmms.20261605.09
Received: Apr. 15, 2026; Accepted: May 3, 2026; Published: May 9, 2026

Features of Endothelial Dysfunction Depending on the Type of Obesity in Children: A Cross-Sectional Comparative Study with TMAO Biomarker Profiling
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIbragimova Elnara Farmanovna, Garifulina Lilya Maratovna
Samarkand State Medical University, Samarkand, Republic of Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Endothelial dysfunction is one of the earliest markers of cardiovascular disease in children with obesity. Trimethylamine N-oxide (TMAO), a gut microbiota-derived metabolite, has been proposed as a novel biomarker linking obesity, oxidative stress, and endothelial injury. The differential impact of obesity type - uniform versus abdominal - on TMAO levels and endothelial function in the pediatric population remains insufficiently characterized. Objective: To evaluate the features of endothelial dysfunction, TMAO levels, and cardiometabolic risk profile in children with uniform obesity versus abdominal obesity, and to assess the correlations between TMAO, endothelium-dependent vasodilation (EDVD), and metabolic parameters. Study Design: Cross-sectional, comparative, single-center clinical study. Subjects and Methods: Ninety-four participants aged 10–18 years were enrolled: 38 children with uniform obesity (Group I), 26 children with abdominal obesity (Group II), and 30 healthy controls. Obesity type was classified using BMI standard deviation scores (BMI SDS, WHO Anthro) and waist-to-hip ratio (WC/HC). All participants underwent anthropometric evaluation (BMI, WC, HC, WC/HC), endothelial function assessment by brachial artery reactive hyperemia testing (EDVD; Celermajer method, 1992), and laboratory profiling including fasting glucose, 2-hour post-load glucose (OGTT), HbA1c (with ADA 2024 cut-offs: <5.7% normal; 5.7–6.4% prediabetes; ≥6.5% diabetes), fasting insulin, HOMA-IR, lipid panel, and serum TMAO (ELISA; ELK Biotechnology, USA). Statistical analysis: STATISTICA software; between-group comparisons with appropriate parametric tests; Pearson correlation analysis; significance threshold p < 0.05. Results: Children with abdominal obesity demonstrated significantly higher TMAO levels (6.11 ± 0.13 mmol/L vs. 5.32 ± 0.11 in uniform obesity vs. 3.37 ± 0.16 in controls; all p < 0.01) and lower EDVD (10.62 ± 0.89% vs. 12.36 ± 0.62% vs. 14.78 ± 0.41%; p < 0.001). Endothelial dysfunction (EDVD < 10%) was detected in 58.0% of the abdominal obesity group versus 19.2% in the uniform obesity group. Mean HbA1c was 5.64 ± 0.07% in abdominal obesity (prediabetes zone by ADA criteria) and 5.32 ± 0.09% in uniform obesity (upper-normal range), compared with 4.50 ± 0.03% in controls. HOMA-IR was elevated above the threshold of 2.5 in 34.62% of the abdominal obesity group. TMAO correlated strongly with WC/HC ratio (r = +0.715; p < 0.05), BMI SDS (r = +0.612), HOMA-IR (r = +0.655), and inversely with HDL-C (r = −0.572) and EDVD (r = −0.607). Conclusions: Abdominal obesity in children is associated with significantly greater endothelial dysfunction, higher TMAO levels, and more severe cardiometabolic disturbances compared to uniform obesity. TMAO correlates strongly with markers of visceral adiposity, insulin resistance, dyslipidaemia, and impaired endothelial function, supporting its role as a clinically relevant biomarker of cardiovascular risk in the pediatric population.
Keywords: Endothelial dysfunction, Childhood obesity, Abdominal obesity, Trimethylamine N-oxide, TMAO, Endothelium-dependent vasodilation, HbA1c, Insulin resistance, Cardiometabolic risk, Gut microbiota
Cite this paper: Ibragimova Elnara Farmanovna, Garifulina Lilya Maratovna, Features of Endothelial Dysfunction Depending on the Type of Obesity in Children: A Cross-Sectional Comparative Study with TMAO Biomarker Profiling, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2260-2268. doi: 10.5923/j.ajmms.20261605.09.
Article Outline
1. Introduction
- Childhood and adolescent obesity has emerged as one of the leading global health challenges of the twenty-first century, with prevalence rates continuing to rise across all world regions. [2,16] Beyond its immediate metabolic consequences, pediatric obesity is recognized as a major determinant of early cardiovascular morbidity, acting through a cascade of interrelated pathological mechanisms that collectively accelerate the onset of cardiovascular disease in adulthood. [2,14] One of the earliest and most clinically informative markers of this process is endothelial dysfunction - the impairment of normal vascular endothelial homeostasis manifested by reduced vasodilatory capacity, a pro-inflammatory phenotype, and prothrombotic endothelial activation. [14,18] Endothelial dysfunction precedes detectable structural arterial changes and has been documented in children and adolescents with obesity, underlining the importance of early biomarker-based risk stratification. [10,18]In recent years, trimethylamine N-oxide (TMAO) - a gut microbiota-derived metabolite of dietary phosphatidylcholine, choline, and L-carnitine - has attracted substantial research attention as a novel mediator of cardiometabolic injury. [3,22] TMAO has been demonstrated to promote endothelial dysfunction through multiple mechanistic pathways: activation of vascular inflammatory signalling, inhibition of reverse cholesterol transport, stimulation of foam cell formation, impairment of bile acid metabolism, platelet hyperactivation, and augmentation of oxidative stress. [3,6,13] Elevated TMAO levels have been associated with obesity, [9] insulin resistance, [13] type 2 diabetes mellitus, [17] chronic kidney disease, [21] heart failure, [7] and increased all-cause cardiovascular mortality across multiple large-scale studies. [5,12] Most published evidence, however, derives from adult populations, with a critical gap in the understanding of TMAO's role in pediatric cardiovascular risk, particularly as modulated by obesity phenotype. [8,15]The distinction between uniform (generalised) obesity and abdominal (visceral) obesity is clinically important, as these phenotypes differ substantially in their metabolic and cardiovascular risk profiles. [16] Visceral adipose tissue is metabolically active, producing greater quantities of pro-inflammatory adipokines, reactive oxygen species, and lipid metabolites that amplify systemic inflammatory and oxidative stress. [16,18] These mechanistic differences predict that abdominal obesity would produce more severe endothelial dysfunction and higher TMAO elevations than uniform obesity, yet a direct comparative investigation in the pediatric setting - incorporating both TMAO biomarker profiling and functional endothelial assessment - has not been reported for Central Asian populations.A further methodological limitation of existing pediatric TMAO research is the absence of body composition data - specifically percentage body fat and lean mass - which would allow more precise characterisation of the adipose tissue metabolic burden beyond BMI-based classification alone. The present study acknowledges this limitation and explicitly incorporates it as a direction for future investigation (see Section 5).The present study was aimed at evaluating the features of endothelial dysfunction, TMAO levels, and cardiometabolic risk profiles in children with uniform versus abdominal obesity, and at establishing correlations between TMAO, EDVD, and anthropometric and metabolic parameters in a controlled comparative design.
2. Materials and Methods
2.1. Study Design and Setting
- This was a cross-sectional, comparative, single-center clinical study conducted at Samarkand State Medical University (Samarkand, Republic of Uzbekistan). The study enrolled participants over a defined data collection period. The cross-sectional design allows characterisation of associations between variables at a single time point; causal inferences are not drawn from the observed correlations.
2.2. Study Participants
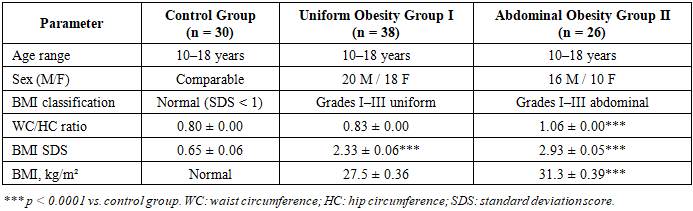
- A total of 94 participants were enrolled. The study group comprised 64 children with exogenous constitutional obesity aged 10 to 18 years (37 boys, 27 girls). The control group included 30 healthy children of the same age range with normal body weight. Exclusion criteria were: secondary obesity; genetic syndromes; chronic diseases; congenital endocrine pathology; and grade IV obesity. The study design is summarised in Table 1.
|
2.3. Anthropometric Assessment and Limitations
- Anthropometry included measurement of body weight, height, waist circumference (WC), and hip circumference (HC). BMI was calculated and expressed as SDS using WHO age- and sex-specific references. WC/HC ratio was calculated as the primary indicator of abdominal adiposity distribution. Physical development data were assessed against WHO-recommended percentile tables for children aged 5–19 years.Limitations of anthropometric assessment: BMI is a moderately accurate measure of adiposity and does not directly quantify body fat percentage, lean mass, or the distribution of visceral versus subcutaneous fat. Similarly, WC/HC ratio, while widely used, has recognised limitations in children due to age- and puberty-related variability. Body composition assessment - specifically percentage body fat and skeletal muscle mass by dual-energy X-ray absorptiometry (DXA) or bioelectrical impedance analysis (BIA) - was not performed in the present study. This constitutes a significant methodological limitation, as body fat percentage provides a more precise and biologically meaningful characterisation of adiposity than BMI alone, and would allow more accurate segregation of metabolically obese normal-weight phenotypes from lean subjects. Future studies should incorporate DXA-derived body composition data alongside BMI-based classification to refine the relationship between adiposity phenotype, TMAO, and endothelial function.
2.4. Endothelial Function Assessment
- Endothelial vascular function was assessed by reactive hyperemia testing of the brachial artery using the method of D.S. Celermajer (1992). After 10 minutes of supine rest, brachial artery diameter was measured at rest by ultrasound. A sphygmomanometer cuff was inflated to 250 mmHg for 5 minutes to produce forearm ischaemia; the cuff was then released and brachial artery diameter was remeasured at 60 seconds. EDVD was calculated as the percentage increase from baseline. A ≥ 10% increase indicated preserved endothelial vasomotor function; EDVD < 10% was classified as endothelial dysfunction.Limitations: Reactive hyperemia testing of the brachial artery by ultrasound (flow-mediated dilation) is a non-invasive, validated, and widely applied method for endothelial function assessment in children. However, it is operator-dependent and has moderate inter-study reproducibility. Future studies should consider supplementary markers of endothelial activation - including serum endothelin-1, asymmetric dimethylarginine (ADMA), and vascular cell adhesion molecule-1 (VCAM-1) - to provide a more comprehensive assessment of endothelial dysfunction.
2.5. Laboratory Investigations
- Venous blood was sampled on an empty stomach after a 12-hour fast. Fresh serum was used for biochemical analysis. Fasting glucose, 2-hour post-load glucose (standard OGTT), HbA1c, fasting insulin, total cholesterol, HDL-C, LDL-C, and triglycerides were measured on a Cobas Integra 400 analyser (Roche Diagnostics, Germany).
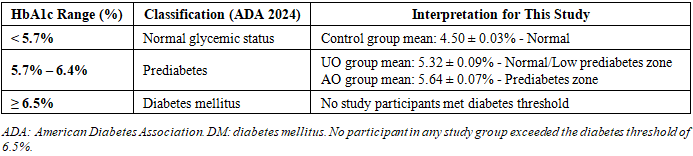
2.5.1. HbA1c Classification
- HbA1c results were interpreted according to American Diabetes Association (ADA) 2024 diagnostic criteria (Table 2):
|
2.6. Ethical Considerations
- The study was conducted in accordance with the principles of the Declaration of Helsinki. The protocol was approved by the Local Bioethics Committee of Samarkand State Medical University. Written informed consent was obtained from all participants and their legal guardians prior to enrolment. Participation was entirely voluntary and withdrawal carried no consequence for clinical care. All data were analysed anonymously.
2.7. Statistical Analysis
- Statistical analysis was performed using the STATISTICA for Windows software package. Continuous data are presented as mean ± standard deviation (M ± SD). Between-group comparisons used analysis of variance (ANOVA) with post hoc pairwise testing; the chi-square test was used for categorical variables. Pearson correlation coefficients were calculated for all pairs of continuous variables. Statistical significance was set at p < 0.05.
3. Results
3.1. Anthropometric Characteristics
- Children with abdominal obesity (Group II) demonstrated statistically significantly higher values across all key anthropometric indicators compared with uniform obesity (Group I) and controls. BMI was 31.3 ± 0.39 kg/m² in Group II versus 27.5 ± 0.36 kg/m² in Group I (p = 0.0001). Waist circumference was 92.13 ± 1.07 cm versus 72.19 ± 0.85 cm (p = 0.0001). The WC/HC ratio - the primary objective indicator of abdominal visceral fat distribution - was significantly elevated in Group II (1.06 ± 0.00) compared with Group I (0.83 ± 0.00; p = 0.0001) and controls (0.80 ± 0.00; p = 0.0001). BMI SDS was 2.93 ± 0.05 in Group II versus 2.33 ± 0.06 in Group I (p = 0.0001) and 0.65 ± 0.06 in controls.
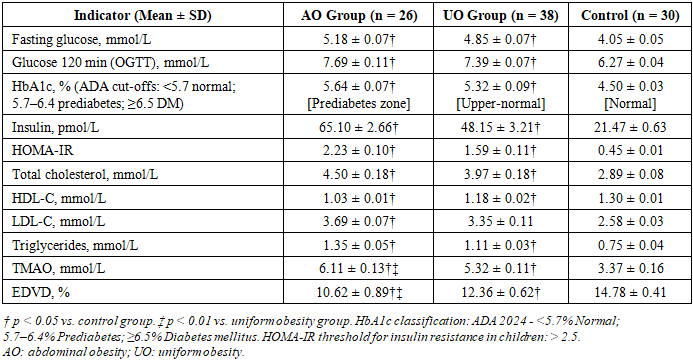
3.2. Carbohydrate and Lipid Metabolism
- The full panel of carbohydrate and lipid metabolism indicators is presented in Table 3 with HbA1c classification according to ADA 2024 cut-offs. Fasting hyperglycaemia was observed in 34.62% of Group II versus 18.42% of Group I. Impaired glucose tolerance (2-hour OGTT glucose 7.8–11.0 mmol/L) was detected in 46.15% of Group II versus 26.32% of Group I. HbA1c in the abdominal obesity group (5.64 ± 0.07%) falls within the prediabetes zone (5.7–6.4% by ADA criteria), while the uniform obesity group mean (5.32 ± 0.09%) is in the upper-normal range. No participants in any group reached the diabetes threshold (HbA1c ≥ 6.5%). Hyperinsulinaemia was present in 50.0% of Group II versus 26.32% of Group I, and elevated HOMA-IR (> 2.5) in 34.62% versus 18.42% respectively. Hypertriglyceridaemia and low HDL-C were significantly more prevalent in abdominal obesity (46.15% and 42.31% respectively) compared to uniform obesity (15.79% and 18.42%; both p < 0.05). Figure 1 provides a graphical comparison of metabolic abnormality frequencies.
|
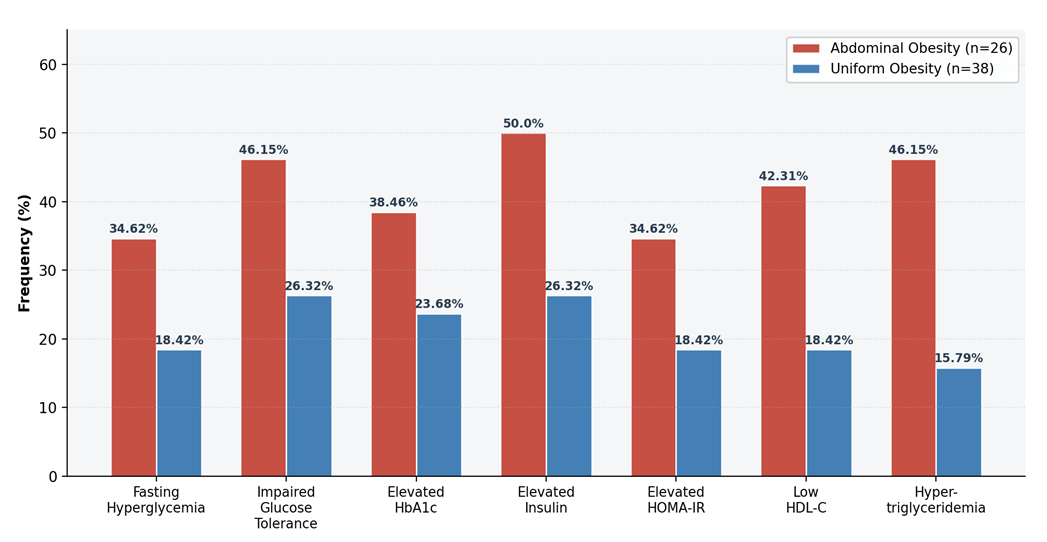 | Figure 1. Frequency of Carbohydrate and Lipid Metabolism Abnormalities by Obesity Type. Red bars: abdominal obesity (AO, n=26); blue bars: uniform obesity (UO, n=38). All between-group differences for hypertriglyceridaemia and low HDL-C: p < 0.05 |
3.3. Endothelial Function
- EDVD assessment revealed that endothelial dysfunction (EDVD < 10%) was present in 22 of 26 children (58.0%) with abdominal obesity - a statistically significantly higher prevalence than in uniform obesity (5 of 38 children; 19.2%; p < 0.001). Mean EDVD was 10.62 ± 0.89% in Group II, 12.36 ± 0.62% in Group I, and 14.78 ± 0.41% in controls. Despite the Group II mean remaining technically above the 10% threshold, it is notably close to the boundary, and the high frequency of individual values below this threshold is clinically significant. Figure 2 illustrates the prevalence of endothelial dysfunction by group.
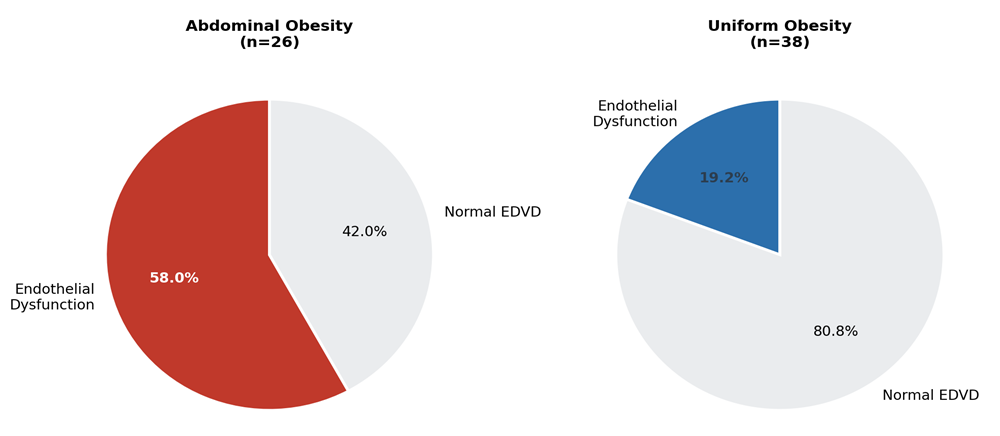 | Figure 2. Prevalence of Endothelial Dysfunction (EDVD < 10%) by Obesity Type. Left: abdominal obesity (58.0% affected); right: uniform obesity (19.2% affected). p < 0.001 for between-group comparison |
3.4. TMAO Levels and Correlations
- TMAO levels were significantly elevated in both obesity groups compared to controls, with the highest values in abdominal obesity (6.11 ± 0.13 mmol/L vs. 5.32 ± 0.11 mmol/L in uniform obesity vs. 3.37 ± 0.16 mmol/L in controls; all pairwise p < 0.01). Figures 3 and 4 provide graphical representations of TMAO and EDVD by group and the metabolic parameter panel with clinical reference thresholds. The correlation heatmap (Figure 5) summarises Pearson r values for TMAO and EDVD versus all anthropometric and metabolic indicators.
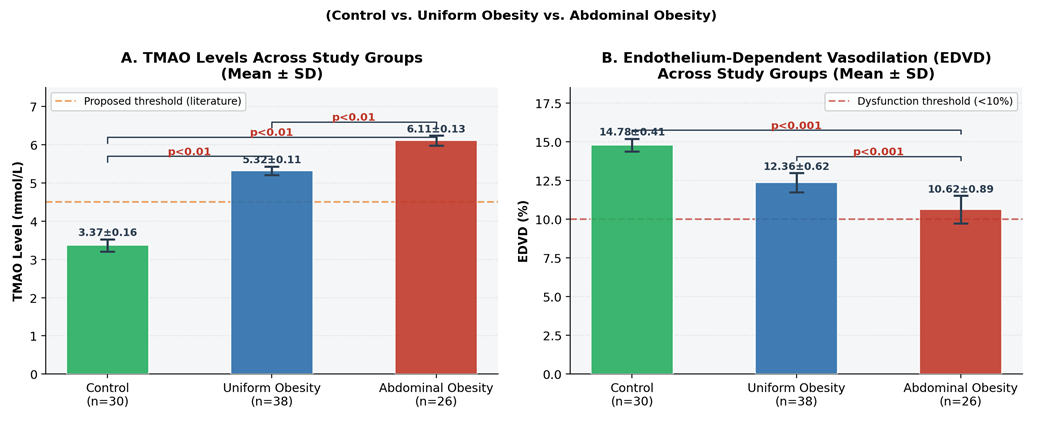 | Figure 3. TMAO Levels (A) and EDVD (B) by Study Group. Orange dashed line in A: proposed TMAO threshold from literature; red dashed line in B: EDVD dysfunction threshold (<10%). Bars: Mean ± SD. Significance brackets: p < 0.01 for TMAO; p < 0.001 for EDVD (pairwise comparisons shown) |
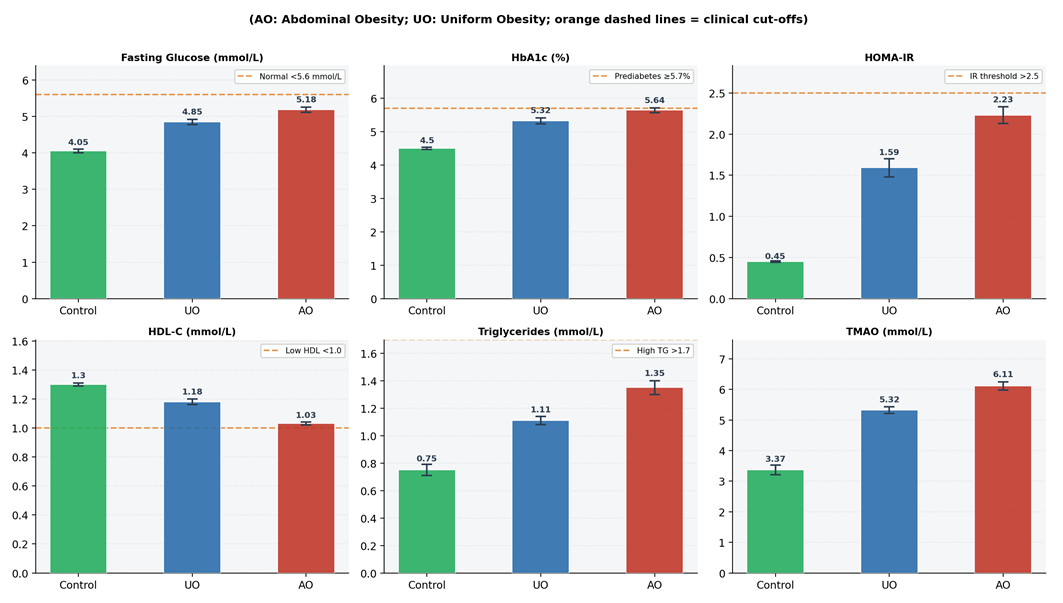 | Figure 4. Metabolic Parameters by Group with Clinical Reference Cut-offs. Orange dashed lines indicate relevant clinical thresholds: fasting glucose (5.6 mmol/L), HbA1c prediabetes threshold (5.7%), insulin resistance (HOMA-IR 2.5), low HDL-C (1.0 mmol/L), high triglycerides (1.7 mmol/L). Note that no participants exceeded ADA diabetes threshold for HbA1c |
|
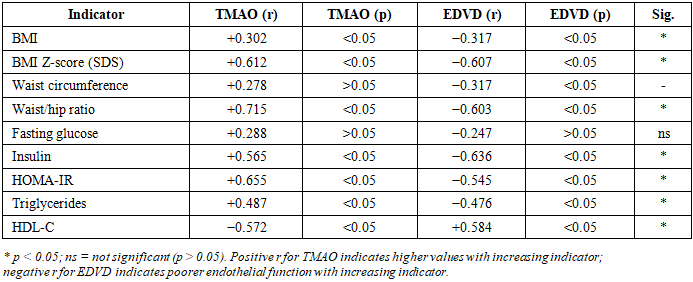
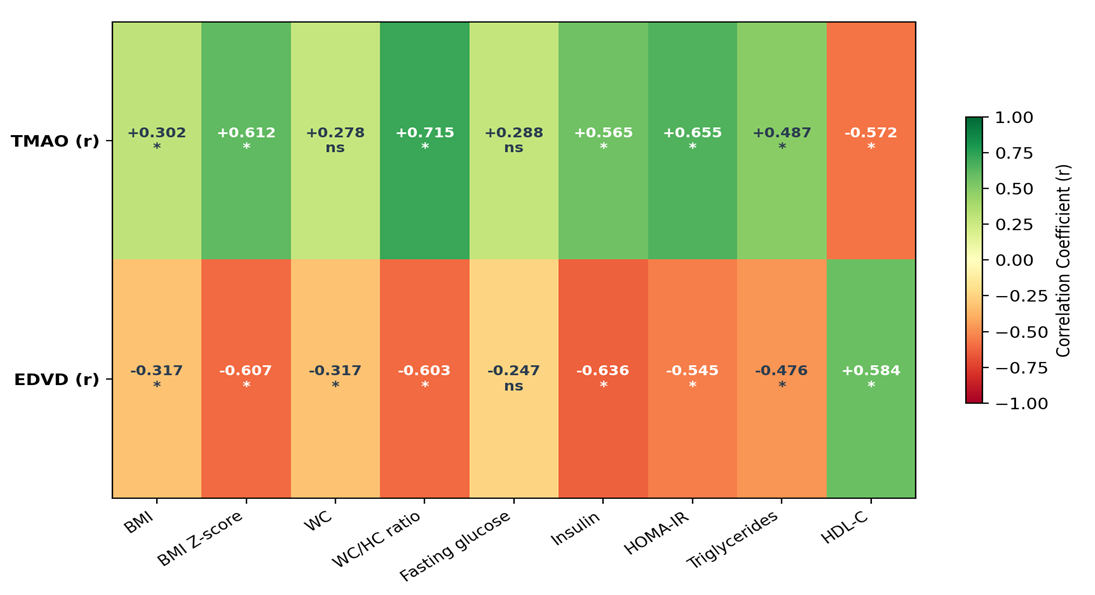 | Figure 5. Pearson Correlation Heatmap: TMAO and EDVD vs. Anthropometric and Metabolic Parameters. Colour scale: green = positive correlation; red = negative correlation; intensity proportional to |r|. * p < 0.05; ns = not significant |
4. Discussion
- The present cross-sectional study demonstrates that abdominal obesity in children and adolescents is associated with significantly greater endothelial dysfunction, higher TMAO levels, and a more severe cardiometabolic risk profile compared to uniform obesity. The frequency of endothelial dysfunction (EDVD < 10%) was 58.0% in the abdominal obesity group versus 19.2% in the uniform obesity group - a three-fold difference that is both statistically and clinically significant. These findings are consistent with the established mechanistic primacy of visceral adiposity in driving vascular and metabolic injury and extend this evidence to a paediatric Central Asian cohort with TMAO biomarker profiling. Table 5 provides a structured comparison of our results with key published studies.
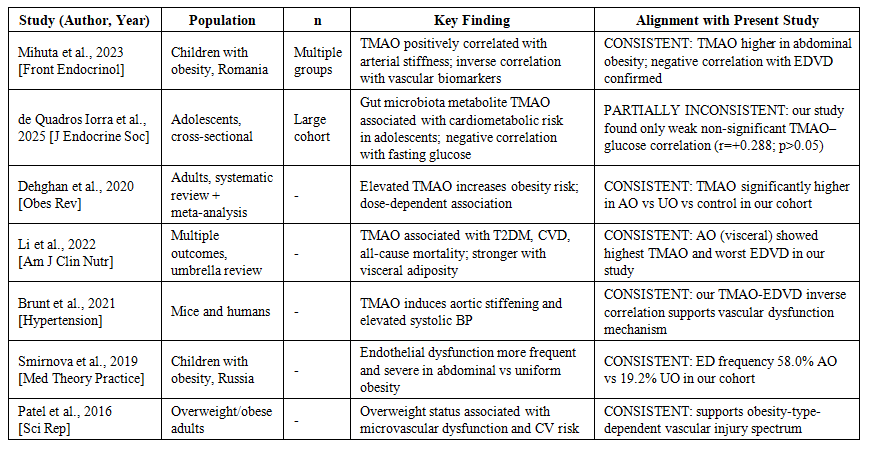 | Table 5. Comparison of present study findings with published literature on TMAO, endothelial function, and obesity in children and adults |
5. Conclusions
- Abdominal obesity in children is associated with significantly higher rates of endothelial dysfunction (58.0% vs. 19.2%; p < 0.001) and markedly elevated TMAO levels (6.11 ± 0.13 vs. 5.32 ± 0.11 mmol/L; p < 0.01) compared to uniform obesity, confirming that obesity type is a critical determinant of vascular and metabolic risk in the paediatric population. Mean HbA1c in the abdominal obesity group (5.64 ± 0.07%) falls within the ADA-defined prediabetes zone, while no participants reached the diabetes diagnostic threshold, highlighting a clinically important pre-diabetic risk window. TMAO correlates strongly with WC/HC ratio (r = +0.715), BMI SDS (r = +0.612), HOMA-IR (r = +0.655), and inversely with EDVD (r = −0.607) and HDL-C (r = −0.572), supporting its role as a clinically meaningful integrative biomarker of cardiometabolic risk in obese children.From a clinical practice perspective, these findings support: (1) systematic obesity-type differentiation (abdominal vs. uniform) in paediatric obesity clinics using WC/HC ratio; (2) early TMAO biomarker measurement as part of cardiovascular risk profiling in children with abdominal obesity; (3) application of ADA-defined HbA1c cut-offs to identify children at highest glycaemic risk; and (4) integration of dietary counselling targeting TMAO-generating food sources as a component of prevention strategies.Priorities for future research are: (1) inclusion of DXA or BIA body composition assessment (percentage body fat and skeletal muscle mass) to improve adiposity characterisation beyond BMI and WC/HC; (2) prospective longitudinal design to determine whether elevated childhood TMAO predicts adult cardiovascular events; (3) supplementary endothelial biomarkers (ADMA, endothelin-1, VCAM-1) alongside functional EDVD testing; (4) gut microbiome profiling to identify the microbial drivers of TMAO elevation in paediatric abdominal obesity; and (5) randomised dietary intervention trials evaluating the impact of TMAO-reducing dietary modifications on endothelial function and cardiometabolic risk in obese children.
Ethics Approval
- Local Bioethics Committee, SamSMU. Informed consent obtained from all participants and legal guardians.