Gafurova Feruza Akhrorovna1, Uteniyazova Dilbar Kojambergenovna2
1Center for the Development of Professional Qualifications of Medical Workers, Department of Obstetrics, Gynecology and Perinatal Medicine, Uzbekistan
2Karakalpakstan Medical Institute, Department of Obstetrics and Gynecology, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Background: Non-developing pregnancy (NDP) of the embryonic demise (ED) type is a clinically heterogeneous condition whose pathogenesis encompasses genetic, pathomorphological, infectious, and hemostatic mechanisms. The latent period between cessation of vital signs and clinical manifestation defines its distinctive diagnostic challenge. Objective: To analyze the clinical, hematological, hemostatic, and microbiological characteristics of NDP across three subtypes-anembryonic pregnancy type I (AN I), type II (AN II), and embryonic demise (ED)-and to contextualize findings within current evidence on genetic and pathomorphological mechanisms. Materials and Methods: 130 patients with verified NDP were prospectively studied at the Nukus branch of the Republican Specialized Scientific and Practical Medical Center Mother and Child Health. Detailed laboratory evaluation (complete blood count, hemostasis including D-dimer, vaginal microbiota) was performed in 61 patients stratified by NDP subtype. Results: Patients with ED presented at later gestational ages (67±13 days) versus AN I (56±13 days) and AN II (62±9 days). No significant between-group differences were found in CBC or standard coagulation parameters; however, D-dimer was significantly elevated in ED (0.459±0.512 μg/mL) versus AN I (0.291±0.210 μg/mL, p<0.05). Normocenosis predominated (64%), with nonspecific vulvovaginitis in 33%; Escherichia coli was most frequently isolated at diagnostically significant concentrations. Conclusions: The relative uniformity of routine laboratory parameters contrasts with specific hemostatic perturbations in ED. Chromosomal and pathomorphological investigations of products of conception are essential to fully elucidate NDP pathogenesis and guide targeted management.
Keywords:
Non-developing pregnancy, Embryonic demise, Anembryonia, Chromosomal abnormalities, D-dimer, Vaginal microbiota, Pathomorphology, Genetic analysis, First trimester, Chorionic villi
Cite this paper: Gafurova Feruza Akhrorovna, Uteniyazova Dilbar Kojambergenovna, Clinical and Laboratory Features of Non-Developing Pregnancy of the Embryonic Demise Type: Hematological, Hemostatic, Microbiological Characteristics with Genetic and Pathomorphological Perspectives, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2245-2251. doi: 10.5923/j.ajmms.20261605.07.
1. Introduction
Non-developing pregnancy (NDP), particularly in the form of embryonic demise, represents a persistent challenge in contemporary obstetrics and gynecology. It constitutes a substantial proportion of early reproductive losses: approximately 10–20% of clinically confirmed pregnancies end in first-trimester miscarriage, with a notable fraction attributed to missed abortion or embryonic demise [1,2].The pathogenesis of embryonic demise is complex and multifactorial, encompassing genetic, infectious, endocrine, immunological, and environmental influences. Among these, chromosomal abnormalities are recognized as the predominant cause, accounting for 50–68% of first-trimester losses [3,4]. A landmark 2023 Nature Medicine genomic study of 1,745 spontaneous pregnancy losses demonstrated that conventional karyotyping detects chromosomal abnormalities in approximately 50.4% of products of conception (POCs), while advanced genome-wide haplarithmisis reveals additional cryptic aberrations in a further 35.1% of cases, elevating the total genomic contribution to an estimated 67.8% [5].Beyond gross chromosomal imbalances, single-gene perturbations, confined placental mosaicism, uniparental disomy, and pathogenic copy number variants (CNVs) represent an expanding category of "hidden" genetic causes undetectable by standard karyotyping [6,7]. These findings underscore the critical need for chromosomal microarray analysis (CMA) and next-generation sequencing (NGS) in the systematic investigation of NDP.Pathomorphological examination of POCs provides complementary information essential for etiological classification. Chorionic villous changes characteristic of chromosomal abnormality (hydrops, stromal hypoplasia, polar trophoblast proliferation) contrast with the decidual vasculopathy, chronic intervillositis, and impaired trophoblast invasion more commonly observed in chromosomally normal losses, each category carrying distinct therapeutic implications for future pregnancies [8,9].Infectious factors, particularly endometrial chronic inflammation and ascending reproductive tract infections, may impair trophoblastic invasion and compromise early embryogenesis [10]. Cytomegalovirus has been identified as a contributing factor in approximately 7% of spontaneous abortions, with lymphoplasmacytic chronic villitis as the predominant histopathological finding [11].The Purpose of the Study: to analyze clinical and diagnostic features of non-developing pregnancy based on clinical data, ultrasound findings, laboratory parameters, and to discuss the genetic and pathomorphological aspects essential for elucidating its pathogenesis.
2. Materials and Methods
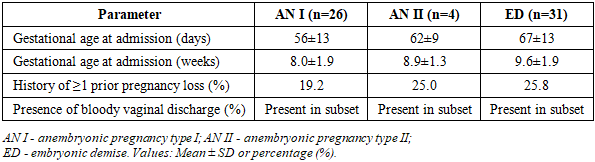
A total of 130 patients with a verified diagnosis of non-developing pregnancy were enrolled in the study. All patients received treatment in the Department of Gynecology of the Nukus branch of the Republican Specialized Scientific and Practical Medical Center "Mother and Child Health" of the Ministry of Health of the Republic of Uzbekistan. Detailed laboratory evaluation was performed in 61 patients stratified by NDP subtype: AN I (n=26), AN II (n=4), and ED (n=31).The clinical examination included anamnesis collection, assessment of somatic and gynecological morbidity, and evaluation of reproductive history. All patients underwent standard laboratory evaluation: complete blood count (CBC), biochemical analysis, hemostasis profile (APTT, prothrombin index, fibrinogen, thrombin time, INR, D-dimer), microscopic vaginal smear examination, bacteriological culture, and serum β-hCG determination. Ultrasound examination was performed at admission and at defined follow-up intervals.Statistical analysis employed methods of variation statistics. Quantitative variables are expressed as mean (M) ± standard deviation (SD). Group comparisons used Student's t-test for normally distributed data and chi-square (χ²) for categorical variables. Significance threshold: p ≤ 0.05. Data processing: Microsoft Excel 15.0 and Statistica 10.Table 1. General Characteristics of Patient Groups
 |
| |
|
3. Results
1. Gestational Age at HospitalizationThe shortest gestational age at admission was observed in AN I (56±13 days, ≈8.0±1.9 weeks), followed by AN II (62±9 days, ≈8.9±1.3 weeks), with the longest duration recorded in the ED group (67±13 days, ≈9.6±1.9 weeks). This progressive pattern confirms that patients with embryonic demise consistently present at later gestational stages compared with anembryonic subtypes, reflecting the biologically distinct latent period characteristic of ED (Figure 1).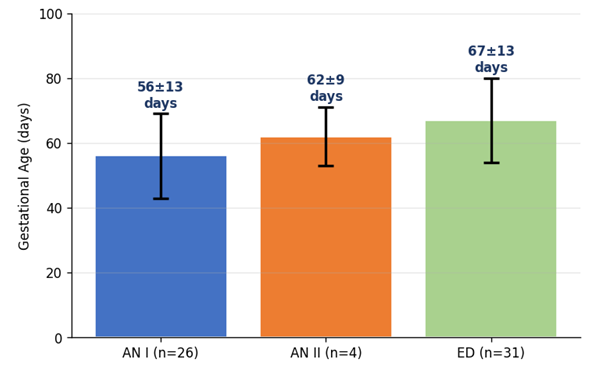 | Figure 1. Mean Gestational Age at Hospitalization by NDP Subtype (days, Mean ± SD) |
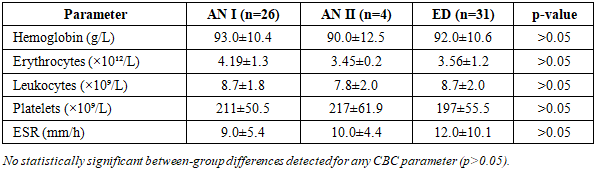
2. Complete Blood Count ParametersTable 2. Complete Blood Count Parameters by Non-Developing Pregnancy Subtype (Mean ± SD)
 |
| |
|
Complete blood count parameters were generally within physiological limits across all groups. Hemoglobin levels showed a mild non-significant reduction trend (AN I 93.0±10.4 g/L; AN II 90.0±12.5 g/L; ED 92.0±10.6 g/L). Leukocyte counts were comparable (8.7, 7.8, 8.7 ×10⁹/L), indicating absence of pronounced systemic inflammatory response. The ESR was numerically higher in ED (12±10.1 mm/h) versus AN I (9±5.4 mm/h), potentially reflecting subclinical inflammation, though not statistically significant (Figure 2).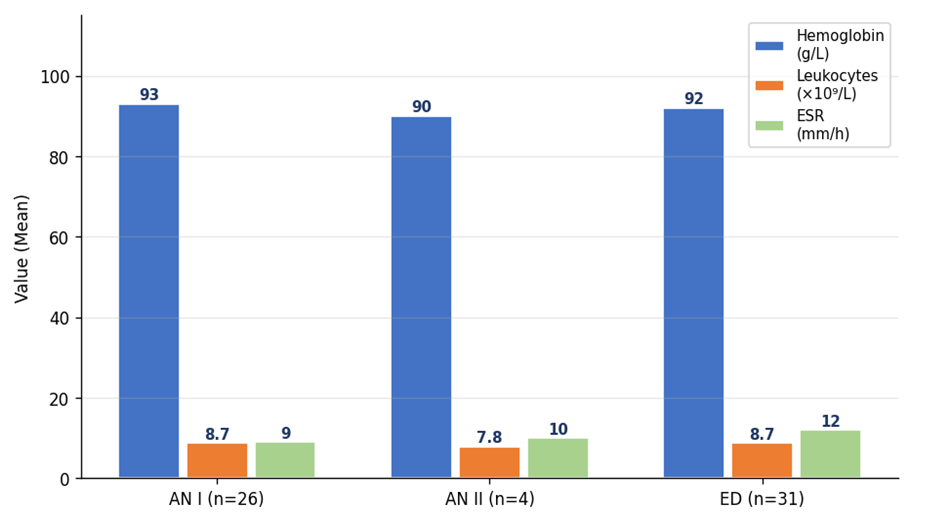 | Figure 2. Complete Blood Count Parameters by NDP Subtype (Mean ± SD). No significant intergroup differences |
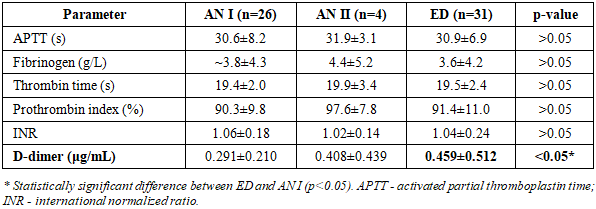
3. Hemostasis ParametersTable 3. Hemostasis Parameters by Non-Developing Pregnancy Subtype (Mean ± SD)
 |
| |
|
Most coagulation parameters were comparable across groups. The critical finding was a progressive increase in D-dimer from AN I (0.291±0.210 μg/mL) through AN II (0.408±0.439 μg/mL) to ED (0.459±0.512 μg/mL), with a statistically significant difference between ED and AN I (p<0.05). This suggests more pronounced coagulation system activation in embryonic demise, potentially reflecting placental tissue injury, local hypoxia, or subclinical coagulopathy (Figure 3).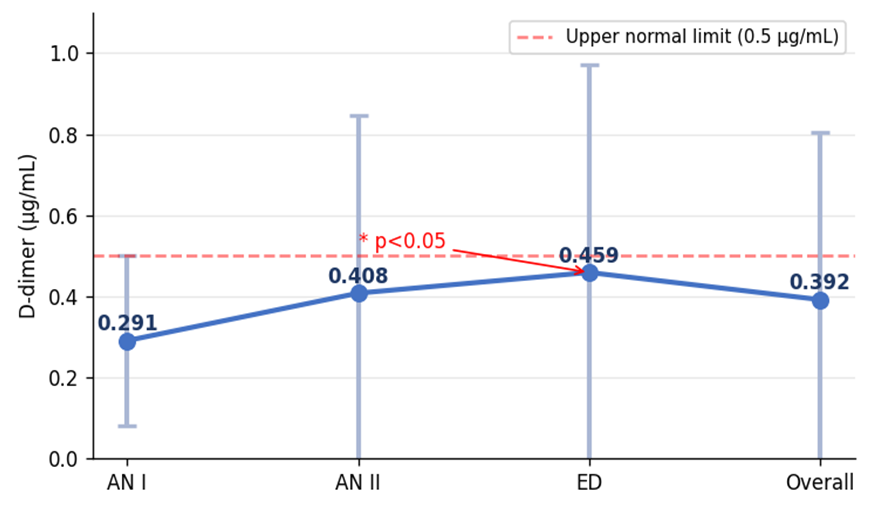 | Figure 3. D-dimer Levels Across NDP Subtypes (μg/mL, Mean ± SD). * p<0.05 ED vs AN I |
4. Vaginal Microbiota and Bacteriological FindingsTable 4. Vaginal Microbiota Distribution by Non-Developing Pregnancy Subtype (n=61)
 |
| |
|
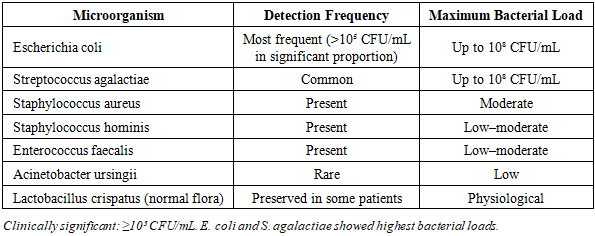
Table 5. Most Frequently Isolated Microorganisms (Bacteriological Culture, n=61)
 |
| |
|
Normocenosis predominated (64%, n=39). Approximately one-third of patients (33%, n=20) exhibited nonspecific vulvovaginitis, while candidiasis was rare (3%, n=2). E. coli was the most frequently isolated pathogen at clinically significant concentrations (>10⁵ CFU/mL). These microbiological findings implicate ascending infectious-inflammatory factors in the pathogenesis of NDP, particularly in the context of impaired endometrial receptivity and trophoblast function (Figure 4).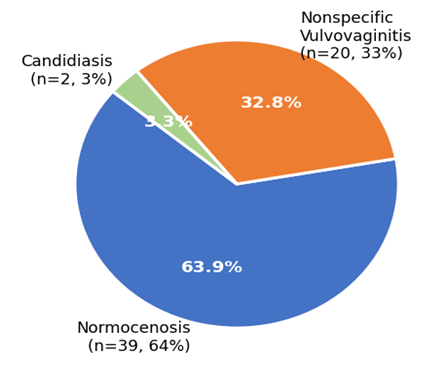 | Figure 4. Vaginal Microbiota Distribution Among NDP Patients (n=61) |
5. Pathogenetic Aspects: Genetic and Pathomorphological Evidence5.1. Genetic Mechanisms: Current EvidenceFull characterization of NDP pathogenesis requires genetic investigation of products of conception that goes beyond standard clinical laboratory evaluation. Chromosomal abnormalities represent the dominant etiological factor in first-trimester pregnancy loss, detected in 50–68% of cases depending on the analytical method [3,4,5]. Figure 5 illustrates the distribution of chromosomal abnormality types in first-trimester losses.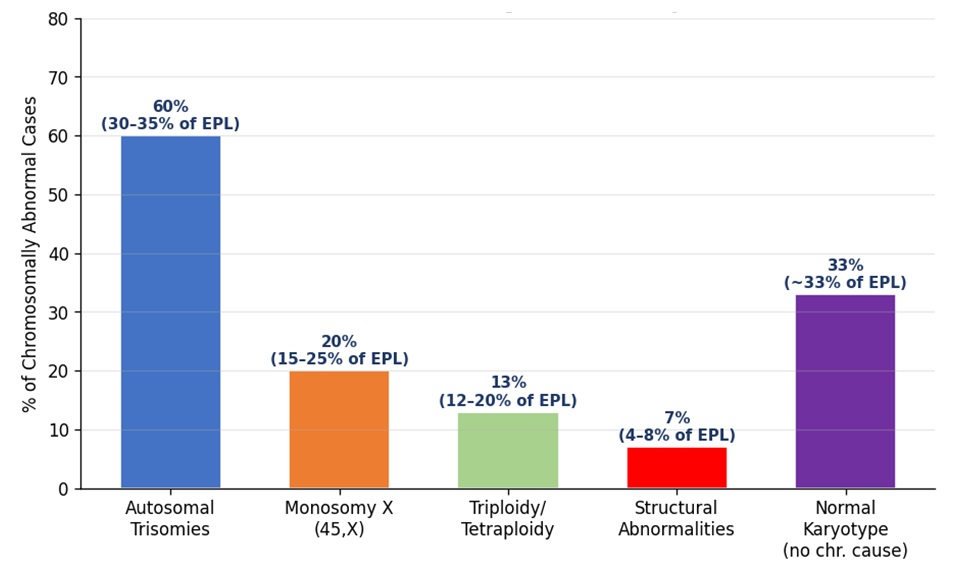 | Figure 5. Chromosomal Abnormality Spectrum in First-Trimester Pregnancy Loss (Literature Data [3,4,5]). Values expressed as percentage among chromosomally abnormal products of conception |
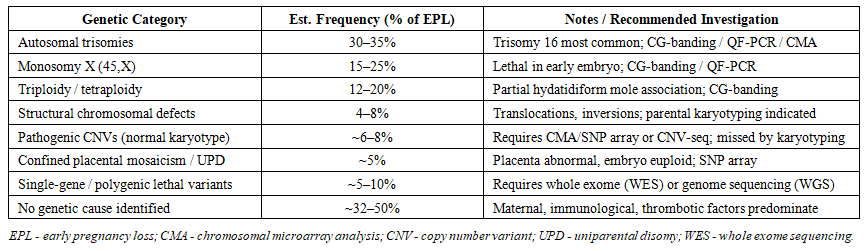 | Table 6. Classification of Genetic Causes of Non-Developing Pregnancy and Recommended Diagnostic Methods |
Essers et al. (Nature Medicine, 2023) demonstrated through genome-wide haplarithmisis that advanced molecular analysis identifies chromosomal aberrations in an additional 35.1% of losses with normal conventional karyotypes, raising the estimated total genomic contribution to approximately 67.8% [5]. This has major implications: a significant proportion of NDP cases currently classified as "idiopathic" may harbor cryptic chromosomal imbalances detectable only by CMA or NGS. A 2024 study of 7,118 miscarriages confirmed the strong maternal age effect: the chromosomal abnormality rate increases by 0.704% per year from ages 23–37 and accelerates to 2.095% per year after age 37 [12].Recommended genetic investigations in NDP (in order of clinical priority):• Conventional G-banding karyotyping of chorionic villi (products of conception) - first-line method• QF-PCR for rapid aneuploid detection (chromosomes 13, 18, 21, X, Y)• Chromosomal microarray analysis (CMA/SNP array) - superior sensitivity for CNVs, mosaicism, UPD• CNV sequencing (CNV-seq) - cost-effective high-resolution alternative to CMA• Parental karyotyping - indicated in recurrent NDP (≥2 consecutive losses)• Whole exome sequencing (WES) - in cases with fetal structural anomalies or recurrent chromosomally normal losses5.2. Pathomorphological Aspects of Non-Developing PregnancyHistopathological examination of POCs from first-trimester NDP provides direct morphological evidence of pathogenetic mechanisms and complements genetic analysis. A systematic histopathological classification of first-trimester miscarriage products distinguishes seven main categories: changes suggesting aneuploidy, embryo anomalies, maternal causes (decidual vasculopathy, impaired trophoblast invasion), multifactorial pathology, hydatidiform mole, ectopic pregnancy, and non-classifiable [8].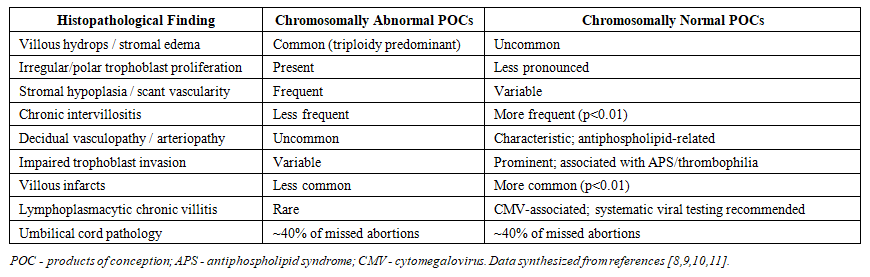 | Table 7. Key Pathomorphological Findings in Products of Conception from First-Trimester Non-Developing Pregnancy |
The distinction between chromosomally driven villous changes and decidual vasculopathy in chromosomally normal losses is clinically critical. The latter category-characterized by impaired trophoblast invasion, decidual arteriopathy, and fibrinoid deposition-is typically associated with antiphospholipid syndrome or other thrombophilic states, and warrants specific investigation (antiphospholipid antibody panel, thrombophilia screening) and prophylactic anticoagulation in subsequent pregnancies [9].In the context of the present study, the significantly elevated D-dimer in ED (0.459±0.512 μg/mL vs. 0.291±0.210 μg/mL in AN I, p<0.05) is pathomorphologically consistent with tissue factor release from necrotic placental tissue and hyperfibrinolysis, correlating with decidual vasculopathy and fibrin deposition documented in chromosomally normal missed abortions. This hemostatic signature may serve as a clinical indicator of underlying thrombotic pathology warranting targeted pathomorphological and immunological investigation.A major Swedish study (Emmer et al., 2024) of 794 missed abortions (gestational weeks 11–21) demonstrated that cord pathology was present in approximately 40% of cases regardless of gestational age, identifying umbilical cord complications as an underrecognized yet frequent etiopathogenetic link to fetal demise [10]. Fetal growth restriction and placental pathology were more prevalent in second-trimester losses, while fetal malformations dominated in early cases-highlighting the value of systematic fetal and placental pathological examination for all NDP cases.Recommended pathomorphological investigations in NDP:• Routine histopathological examination of all products of conception: villous morphology, decidual vasculopathy, trophoblast invasion assessment• Immunohistochemistry for p57KIP2 (to exclude complete hydatidiform mole) when villous hydrops is present• Viral testing (CMV PCR/IHC) in cases with chronic villitis pattern• Combined villous and decidual analysis: helps distinguish chromosomal from maternal (thrombotic/immunological) etiology• Correlation with cytogenetic/CMA results: integrated morphogenetic-cytogenetic diagnosis maximizes etiological yield and guides recurrence risk counseling
4. Discussion
The present study confirms the clinical heterogeneity of NDP and the diagnostic importance of subtype stratification. The consistently later gestational age at admission in the ED group (67±13 days) reflects the inherent biology of embryonic demise-an embryo develops to a defined stage before vital arrest, creating a prolonged, clinically silent retention period that delays diagnosis relative to anembryonic subtypes [1].The absence of statistically significant differences in most routine laboratory parameters across groups underscores the limited discriminatory power of standard CBC and coagulation screening for NDP subtype differentiation. The single exception-D-dimer elevation in ED (p<0.05)-merits prospective validation. Elevated D-dimer in this context may reflect coagulation activation triggered by tissue thromboplastin released from retained necrotic embryonic and placental tissue, local microvascular thrombosis, or subclinical coagulopathy. This finding is pathomorphologically consistent with evidence of decidual vasculopathy and fibrin deposition more prevalent in chromosomally normal missed abortions [8,9].The microbiological profile-normocenosis in 64% but nonspecific vulvovaginitis in 33%, with clinically significant E. coli isolation-underscores the potential infectious-inflammatory contribution to NDP pathogenesis. High-load E. coli and Streptococcus agalactiae contamination of the reproductive tract may compromise endometrial receptivity and impair trophoblast invasion through activation of Toll-like receptor-mediated inflammatory cascades. These findings are consistent with evidence that CMV and bacterial pathogens contribute to pregnancy loss through chronic villitis and impaired early placentation [11].Critically, the present study's clinical and laboratory data represent only the clinically observable surface of NDP pathogenesis. Chromosomal and submicroscopic genomic abnormalities-collectively accounting for 50–68% of first-trimester losses [5]-cannot be inferred from blood tests or ultrasound and mandate dedicated POC genetic analysis. The integration of routine CMA or CNV-seq alongside conventional karyotyping substantially increases the etiological yield and should be considered standard of care, particularly in centers managing patients with recurrent NDP. Complementary pathomorphological examination of POCs provides the morphological correlate of these genetic findings and identifies the subset of chromosomally normal losses attributable to thrombotic or immunological maternal factors, where specific targeted therapy in future pregnancies can meaningfully reduce recurrence risk.
5. Conclusions
The analysis of clinical and laboratory features of non-developing pregnancy of the embryonic demise type demonstrates the following:• Patients with ED are consistently hospitalized at later gestational ages (67±13 days) compared with AN I (56±13 days) and AN II (62±9 days), reflecting the prolonged silent retention period characteristic of embryonic demise.• No statistically significant differences were found in CBC or standard coagulation parameters across subtypes; however, D-dimer was significantly elevated in ED versus AN I (0.459 vs. 0.291 μg/mL, p<0.05), suggesting subtype-specific hemostatic dysregulation with potential pathomorphological correlates.• Vaginal microbiota analysis revealed normocenosis in 64% of patients, with nonspecific vulvovaginitis in 33% and candidiasis in 3%. E. coli was most frequently isolated at diagnostically significant concentrations (>10⁵ CFU/mL), implicating infectious factors in NDP pathogenesis.• Routine clinical-laboratory evaluation, while essential for initial patient management, is insufficient to characterize NDP pathogenesis fully. Chromosomal abnormalities-detectable only by dedicated cytogenetic/molecular analysis of products of conception-account for 50–68% of first-trimester losses.• Systematic genetic investigation (karyotyping, CMA, CNV-seq) of POCs and histopathological examination of chorionic villi and decidua are essential components of a complete diagnostic workup for NDP and should be standardized in clinical practice, particularly for recurrent cases.
References
| [1] | Acuña J., Rukh S., Adhikari S. Point-of-care ultrasound identification of yolk stalk sign in a case of failed first trimester pregnancy. World J Emerg Med. 2018; 9(2): 149-151. |
| [2] | Di Pietro C., Cicinelli E., Guglielmino M.R. et al. Altered transcriptional regulation of cytokines, growth factors, and apoptotic proteins in the endometrium of infertile women with chronic endometritis. Am J Reprod Immunol. 2013; 69(5): 509-517. |
| [3] | Anembryonic Pregnancy. StatPearls. National Library of Medicine. Updated November 6, 2023. https://www.ncbi.nlm.nih.gov/books/NBK499938/. |
| [4] | Bozhinovski G. et al. Chromosomal Abnormalities in Early Pregnancy Losses: A Study of 900 Samples. Balkan J Med Genet. 2024; 26(2): 11-20. DOI: 10.2478/bjmg-2023-0014. |
| [5] | Essers R. et al. Prevalence of chromosomal alterations in first-trimester spontaneous pregnancy loss. Nature Medicine. 2023; 29(12): 3233-3242. DOI: 10.1038/s41591-023-02645-5. |
| [6] | Kapfhamer J.D. et al. Difference between mean gestational sac diameter and crown-rump length as a marker of first-trimester pregnancy loss after IVF. Fertil Steril. 2018; 109(1): 130-136. |
| [7] | Wan J. et al. Patterns of Cytogenomic Findings from a Case Series of Recurrent Pregnancy Loss Provide Insight into the Extent of Genetic Defects Causing Miscarriages. Am J Perinatol. 2024. DOI: 10.1055/a-2277-7867. |
| [8] | Turco M.Y. et al. First-trimester miscarriage: A histopathological classification proposal. Heliyon. 2021; 7(3): e06395. DOI: 10.1016/j.heliyon.2021.e06395. |
| [9] | Kramer R.L. et al. Placental and decidual histology in spontaneous abortion: detailed description and correlations with chromosome number. Obstet Gynecol. 1997. |
| [10] | Emmer R., Ajne G., Papadogiannakis N. Missed abortion in the 11–21-week period: Fetal autopsy and placental histopathological analysis of 794 cases. Eur J Obstet Gynecol Reprod Biol. 2024. DOI: 10.1016/j.ejogrb.2024.02.054. |
| [11] | Donaldson N. et al. Intrauterine Fetal Demise, Spontaneous Abortion and Congenital Cytomegalovirus: A Systematic Review. Viruses. 2024; 16(10): 1552. DOI: 10.3390/v16101552. |
| [12] | Nikitina T.V. et al. Chromosomal Abnormalities in Miscarriages and Maternal Age: New Insights from the Study of 7118 Cases. Cells. 2024; 14(1): 8. DOI: 10.3390/cells14010008. |
| [13] | NICE guideline [NG126]. Ectopic pregnancy and miscarriage: diagnosis and initial management. Published 17 April 2019. https://www.nice.org.uk/guidance/ng126. |
| [14] | Murugan V.A. et al. Role of ultrasound in the evaluation of first-trimester pregnancies in the acute setting. Ultrasonography. 2020; 39(2): 178-189. |
| [15] | Uteniyazova D.K., Gafurova F.A. Clinical and laboratory features of non-developing pregnancy of the anembryonic type in the first trimester. Bulletin of Fundamental and Clinical Medicine. 2026; 3(23): 498-502. DOI: 10.5281/zenodo.19180026. |
| [16] | Uteniyazova D.K., Gafurova F.A. Study of data on the frequency of gynecological diseases and reproductively significant infections in the history of women with non-developing pregnancy. Bulletin of Fundamental and Clinical Medicine. 2026; 3(23): 478-481. DOI: 10.5281/zenodo.19139373. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML