-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2239-2244
doi:10.5923/j.ajmms.20261605.06
Received: Mar. 18, 2026; Accepted: Apr. 9, 2026; Published: May 9, 2026

Modern Aspects of Single-Stage Surgical Treatment of Cholecystocholedocholithiasis Using the Modified Laparoendoscopic Rendezvous Technique
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbduraxmonov Eshonkul Movutovich, Babajanov Axmadjon Sultanbayevich
Central Hospital of the Samarkand City Health Department, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Cholecystocholedocholithiasis represents one of the most clinically challenging conditions in both urgent and elective biliary surgery, as simultaneous pathology of the gallbladder and common bile duct requires effective and safe surgical management strategies. Traditional multi-stage approaches are associated with prolonged treatment, repeated hospitalizations, and increased risk of interstage complications. Objectives: This study was conducted to evaluate the short-term surgical outcomes of patients with cholecystocholedocholithiasis treated using a modified single-stage hybrid laparoendoscopic rendezvous technique combining laparoscopic cholecystectomy with intraoperative endoscopic papillosphincterotomy and choledocholithoextraction. Methods: A single-center retrospective observational study was conducted at the Central Hospital of the Samarkand City Health Department over a six-year period (January 2018-December 2023). A total of 55 patients with calculous cholecystitis and an average risk of cholangiolithiasis who underwent hybrid laparoendoscopic rendezvous were included. Operative duration, intraoperative and postoperative complications (classified by Clavien-Dindo), rate of complete bile duct sanitation, ICU admissions, and length of hospital stay were assessed. Quantitative data were reported as median and interquartile range (IQR). The Mann-Whitney U test was used for group comparisons. Results: The median total operative duration was 120.0 min (IQR 90.0-120.0) and the endoscopic stage lasted 15.0 min (IQR 10.0-20.0). Operative time was significantly longer in acute versus chronic cholecystitis (120.0 vs. 90.0 min; p = 0.035). No intraoperative complications were recorded. Postoperative complications occurred in 7 patients (12.7%), including EPST-associated pancreatitis in 2 (3.6%) and abdominal bleeding in 2 (3.6%). Hyperamylasemia without clinical pancreatitis was observed in 7 patients (12.7%). Complete bile duct sanitation was achieved in 47 patients (85.7%) in a single stage. Median hospital stay was 7.0 days (IQR 6.0-8.0), increasing to 13.0 days (IQR 11.5-14.0) in patients with complications (p = 0.003). No mortality was recorded. Conclusions: The modified laparoendoscopic rendezvous technique is an effective and safe single-stage approach for cholecystocholedocholithiasis in patients with average-risk cholangiolithiasis, providing high rates of complete biliary sanitation, low complication rates, and no mortality.
Keywords: Cholecystocholedocholithiasis, Laparoscopic cholecystectomy, Laparoendoscopic rendezvous, Endoscopic papillosphincterotomy, Common bile duct stones
Cite this paper: Abduraxmonov Eshonkul Movutovich, Babajanov Axmadjon Sultanbayevich, Modern Aspects of Single-Stage Surgical Treatment of Cholecystocholedocholithiasis Using the Modified Laparoendoscopic Rendezvous Technique, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2239-2244. doi: 10.5923/j.ajmms.20261605.06.
Article Outline
1. Introduction
- Gallstone disease and its complicated forms associated with choledocholithiasis remain among the most clinically significant conditions in the spectrum of urgent and elective abdominal surgery worldwide. [1,2] The concomitant presence of stones in the common bile duct (CBD) among patients with calculous cholecystitis is associated with a substantial risk of developing mechanical jaundice, ascending cholangitis, acute biliary pancreatitis, and other life-threatening complications. [3] The reported prevalence of choledocholithiasis in patients undergoing cholecystectomy ranges from 10% to 20%, with higher rates observed in older age groups and emergency presentations. [4] Given these epidemiological data, timely diagnosis and rational selection of surgical tactics are of fundamental importance for improving patient outcomes. [1,5]The traditional multi-stage management strategy - comprising sequential endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy for bile duct clearance followed by laparoscopic cholecystectomy - remains the most widely practiced approach in routine clinical settings. [3] However, this sequential model carries inherent limitations, including prolonged total treatment duration, repeated anesthesia exposure, multiple hospitalizations, elevated aggregate treatment costs, and an estimated 5-10% risk of interstage complications such as cholangitis, biliary pancreatitis, and recurrent stone migration. [4,5] These disadvantages have fueled growing interest in single-stage alternatives that consolidate both interventions within one anesthetic episode. [2,3] Among these, the laparoendoscopic rendezvous (LERV) technique - which employs anterograde guidewire placement through the cystic duct to facilitate selective CBD cannulation - has demonstrated promising results in terms of reducing post-ERCP pancreatitis risk and overall treatment burden. [4,5]The LERV technique offers particular theoretical advantages due to its anterograde guidewire delivery through the cystic duct and the major duodenal papilla, which facilitates highly selective cannulation of the biliary system without retrograde instrumentation of the papilla. [5] This maneuver is postulated to minimize trauma to the sphincter of Oddi and to significantly reduce the risk of post-manipulation pancreatitis compared with conventional ERCP. [2,4] Despite accumulating evidence supporting its efficacy, the outcomes of a modified single-stage laparoendoscopic approach specifically applied to patients with an intermediate risk profile for cholangiolithiasis - representing a clinically significant and frequently encountered patient population - warrant further systematic analysis within a specialized institutional context. [1,3,5]The present study was aimed at examining the short-term surgical results of the modified single-stage laparoendoscopic rendezvous technique - incorporating laparoscopic cholecystectomy with intraoperative endoscopic papillosphincterotomy and choledocholithoextraction - as it was applied to patients with calculous cholecystitis and an average risk of cholangiolithiasis at a single tertiary-level institution.
2. Materials and Methods
2.1. Study Design and Participants
- A single-center retrospective observational cohort study was conducted at the Central Hospital of the Samarkand City Health Department (Samarkand, Uzbekistan). The study period spanned six years, from January 2018 to December 2023. All consecutive patients who underwent the modified hybrid laparoendoscopic rendezvous technique for cholecystocholedocholithiasis during this period were included. The sample was defined by full census inclusion of all eligible patients treated with this technique over the study period, yielding a final cohort of 55 patients. No formal a priori sample size calculation was performed, as this was a retrospective observational study with no comparator arm.Inclusion criteria were: (1) confirmed calculous cholecystitis (acute or chronic); (2) choledocholithiasis with an average risk of cholangiolithiasis based on preoperative clinical, biochemical, and imaging criteria; (3) surgical treatment using the single-stage modified laparoendoscopic rendezvous technique; and (4) complete medical record availability. Exclusion criteria were: (1) prior biliary surgery or sphincterotomy; (2) high-risk cholangiolithiasis requiring emergency decompression; (3) anatomical contraindications to laparoscopic approach; and (4) incomplete clinical documentation.
2.2. Data Collection Instruments
- Data were extracted from institutional medical records including operative reports, anesthesia charts, nursing observation records, and discharge summaries. The primary outcomes assessed were: total operative duration (minutes), duration of the endoscopic stage (minutes), rate of complete single-stage biliary tract sanitation, and incidence of intraoperative and postoperative complications. Complications were classified using the Clavien-Dindo classification system, a validated and internationally accepted ordinal scale for surgical morbidity grading ranging from Grade I (minor deviation from normal postoperative course) to Grade V (death). Severity of illness in ICU patients was assessed using the Sequential Organ Failure Assessment (SOFA) score (range 0-24; higher scores indicate greater organ dysfunction) and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score (range 0-71; higher scores correlate with increased risk of mortality). Length of hospital stay (LOS) was recorded in bed-days.
2.3. Procedures
- All patients underwent standard preoperative evaluation by a surgical team, anesthesiologist, and internist. Patients admitted on an emergency basis received preoperative preparation including intravenous fluid resuscitation, antispasmodic agents, and anti-inflammatory therapy. Venous thromboembolism prophylaxis was administered universally in the form of elastic compression stockings and low-molecular-weight or unfractionated heparin, in accordance with current clinical guidelines. The modified hybrid laparoendoscopic rendezvous procedure was performed under general anesthesia with the patient in the supine position. The laparoscopic stage consisted of standard four-trocar cholecystectomy with cystic duct dissection and anterograde guidewire passage through the cystic duct and major duodenal papilla. The endoscopic stage - performed simultaneously in the same operating theatre under active pneumoperitoneum and without fluoroscopic guidance - comprised endoscopic papillosphincterotomy (EPST) and choledocholithoextraction over the pre-placed guidewire. Questionnaire-based data were not applicable to this study. Retrospective data extraction was performed by the investigative team directly from medical records, with dual verification to ensure accuracy.
2.4. Ethical Considerations
- The study was conducted in accordance with the principles of the Declaration of Helsinki and applicable institutional regulations. Ethical approval was obtained from the Ethics Committee of the Central Hospital of the Samarkand City Health Department. Given the retrospective observational nature of the study, a waiver of individual informed consent was granted by the ethics committee; patient data were anonymized and de-identified prior to analysis to ensure confidentiality. Participation in data collection was voluntary, and no patients were subjected to additional procedures beyond their standard clinical care. No identifying personal information was used in the analysis or reporting.
2.5. Data Analysis
- Statistical analysis was performed using standard statistical software. Quantitative data that did not follow a normal distribution - as assessed by the Shapiro-Wilk test - were reported as median and interquartile range (IQR). The Mann-Whitney U test was selected for comparison of independent continuous variables between two groups (e.g., acute versus chronic cholecystitis), as it is the appropriate non-parametric alternative to the independent samples t-test when data do not meet normality assumptions. Categorical variables were expressed as absolute frequencies and percentages. Differences were considered statistically significant at a two-tailed p-value of less than 0.05 (p < 0.05).
3. Results
3.1. Demographic and Clinical Characteristics
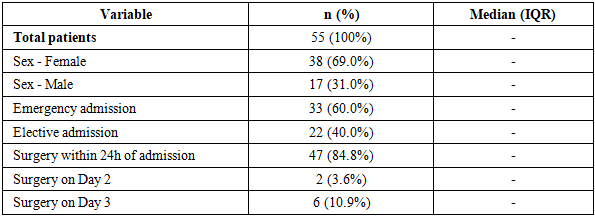
- The study cohort comprised 55 patients with a female predominance of 38 women (69.0%) and 17 men (31.0%). Of the total, 33 patients (60.0%) were admitted on an emergency basis, while 22 (40.0%) underwent planned (elective) hospitalization. The majority of patients - 47 (84.8%) - proceeded to surgery within the first 24 hours of hospital admission. Two patients (3.6%) underwent surgery on the second day following an unsuccessful attempt at transpapillary intervention on the first day, and six patients (10.9%) were operated on the third day due to the need for additional preoperative diagnostic workup. The demographic and admission characteristics of the study population are summarized in Table 1.
|
3.2. Operative Duration
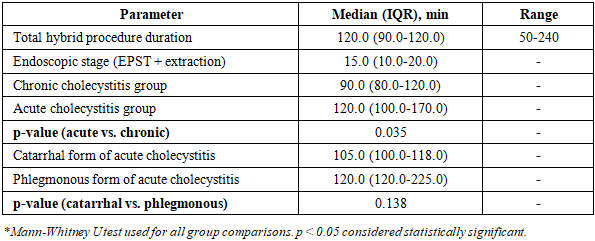
- The total operative duration of the hybrid laparoendoscopic procedure ranged from 50 to 240 minutes across the study cohort. The median total operative time was 120.0 min (IQR 90.0-120.0). The median duration of the endoscopic stage - comprising EPST and choledocholithoextraction performed under non-standard conditions (supine patient position, pneumoperitoneum, absence of fluoroscopic guidance) - was 15.0 min (IQR 10.0-20.0). Comparative analysis between groups stratified by the morphological state of the gallbladder wall revealed that operative time was statistically significantly longer in patients with acute calculous cholecystitis compared to those with chronic inflammatory changes: 120.0 min (IQR 100.0-170.0) versus 90.0 min (IQR 80.0-120.0), respectively (p = 0.035). Within the acute cholecystitis subgroup, further stratification by inflammatory severity demonstrated no statistically significant difference in operative duration between the catarrhal form - 105.0 min (IQR 100.0-118.0) - and the phlegmonous form - 120.0 min (IQR 120.0-225.0) - (p = 0.138). These findings are presented in Table 2.
|
3.3. Intraoperative and Postoperative Complications
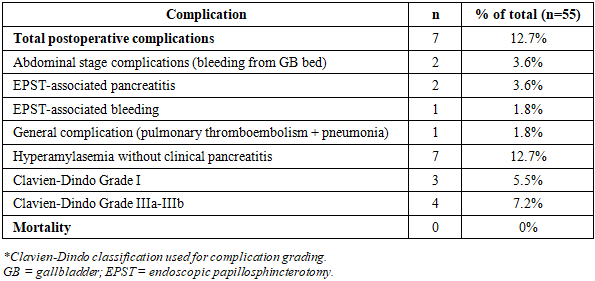
- No intraoperative complications were recorded in any of the 55 patients. Specifically, no instances of intraoperative bleeding, calculus basket impaction, retroduodenal perforation, or other technical adverse events were observed during either the laparoscopic or endoscopic stage of the procedure. Postoperative complications of any type occurred in 7 patients (12.7%). Complications attributable to the abdominal stage - early postoperative hemorrhage from the gallbladder bed - were observed in 2 patients (3.6%); one of these required re-video laparoscopy with hemostasis and abdominal drainage. No instances of cystic duct stump leakage or infectious abdominal complications were identified. EPST-associated complications were documented in 3 patients (5.45%): post-ERCP pancreatitis in 2 patients (3.6%) and papillosphincterotomy site bleeding in 1 patient (1.8%), successfully managed by argon plasma coagulation during emergency duodenoscopy. One general postoperative complication (1.8%) was recorded - pulmonary thromboembolism with subsequent polysegmental pneumonia - resolved with antibiotic and anticoagulant therapy. Asymptomatic hyperamylasemia without clinical or imaging signs of acute pancreatitis was observed in 7 additional patients (12.7%), with a median amylase level of 445.0 U/L (range 113-1372 U/L), normalizing within 24 hours. By Clavien-Dindo classification, Grade I complications occurred in 3 cases (5.5%) and Grade IIIa-IIIb complications in 4 cases (7.2%). No mortality was recorded. These findings are presented in Table 3.
|
3.4. Biliary Sanitation Rate and Length of Hospital Stay
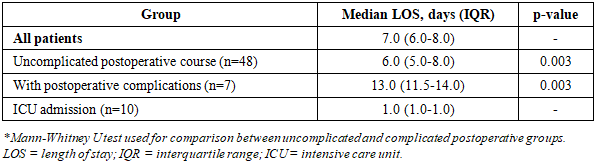
- Complete single-stage biliary tract sanitation - defined as successful laparoscopic cholecystectomy combined with full clearance of the common bile duct in one operative session - was achieved in 47 patients (85.7%). In the remaining 8 patients (14.3%), complete sanitation was not accomplished at the initial procedure: 6 patients (10.9%) required a repeat endoscopic intervention on the second postoperative day, while 2 patients (3.6%) ultimately required three separate stages of biliary tract management. These repeat interventions were not associated with additional complications or a clinically significant prolongation of hospital stay. Ten patients (18.2%) required postoperative ICU admission, primarily for monitoring purposes related to the learning curve and duration of the novel technique. The median ICU stay was 1.0 day (IQR 1.0-1.0). Severity scores among ICU patients were low: SOFA 3.0 points (IQR 1.25-4.0) and APACHE II 9.0 points (IQR 8.0-12.25), indicating low-severity illness and a favorable predicted outcome. The median total length of hospital stay was 7.0 bed-days (IQR 6.0-8.0), ranging from 4 to 14 days. Patients with an uncomplicated postoperative course (n = 48, 87.3%) had a median LOS of 6.0 days (IQR 5.0-8.0). Patients who developed postoperative complications (n = 7, 12.7%) had a significantly prolonged median LOS of 13.0 days (IQR 11.5-14.0), representing a 2.2-fold increase compared to the uncomplicated group (p = 0.003). Length of stay data are presented in Table 4.
|
4. Discussion
- The present retrospective study was aimed at evaluating the short-term surgical outcomes of the modified single-stage laparoendoscopic rendezvous technique in patients with cholecystocholedocholithiasis at average risk for cholangiolithiasis, and the results demonstrate a favorable combination of procedural efficacy, patient safety, and clinical utility. The median operative duration of 120 minutes - performed simultaneously incorporating both laparoscopic cholecystectomy and intraoperative EPST with choledocholithoextraction - appears reasonable for a combined hybrid intervention, particularly given the requirement for coordinated multidisciplinary involvement. The brief endoscopic stage of only 15 minutes, despite being conducted under technically demanding non-standard conditions (supine patient, active pneumoperitoneum, no fluoroscopy), underscores the technical reproducibility achievable by a trained and experienced multidisciplinary team.The observed statistically significant prolongation of operative duration in acute versus chronic calculous cholecystitis (p = 0.035) aligns with established surgical principles, as acute inflammation is expected to produce greater tissue edema, adhesion formation, and anatomical distortion - particularly within the hepatoduodenal ligament - thereby increasing dissection time. This finding is consistent with those of Sayed et al., [4] who similarly reported longer operative times in the setting of acute cholecystitis when comparing single-stage ERCP-first and cholecystectomy-first rendezvous approaches. Importantly, the absence of a statistically significant difference between the catarrhal and phlegmonous subtypes of acute cholecystitis (p = 0.138) suggests that the acute inflammatory state per se - rather than its histological severity - is the decisive determinant of operative complexity. This nuance is not uniformly acknowledged in the existing literature but may carry important preoperative planning implications. A comparable observation was noted by Gerosa et al., [2] who found that operative complexity in single-stage cholecystocholedocholithiasis management was largely independent of the degree of gallbladder wall inflammation.The complete absence of intraoperative complications across all 55 procedures is a particularly significant finding, corroborating the technical safety of the modified rendezvous technique in appropriately selected patients treated at a specialized center. The overall postoperative complication rate of 12.7%, with EPST-associated pancreatitis occurring in only 3.6% of patients - despite 82.9% carrying at least one established risk factor for post-ERCP pancreatitis - is notably lower than rates reported for conventional retrograde ERCP, which typically range from 5% to 15% in comparable populations. [1,5] This favorable pancreatitis rate is likely attributable to the fundamental mechanistic advantage of the rendezvous approach: anterograde guidewire delivery through the cystic duct eliminates the need for repeated blind retrograde cannulation attempts of the major duodenal papilla, thereby minimizing papillary trauma and pancreatic ductal instrumentation. These findings are consistent with those of Koiava et al., [5] who similarly reported low rates of EPST-associated pancreatitis in their single-center rendezvous series. The 85.7% single-stage complete biliary sanitation rate observed in the present cohort is consistent with published outcomes for hybrid laparoendoscopic techniques, which generally report primary success rates of 80-90% in the literature. [1,3] Lv et al. [3] reported comparable sanitation rates using a hybrid operating room-based model, while Tai and Zhang's [1] meta-analysis confirmed that single-stage strategies achieve biliary clearance rates non-inferior to sequential multi-stage approaches. The need for repeat endoscopic interventions in 14.3% of patients did not result in additional complications or substantially prolong hospitalization, supporting the safety of staged completion in cases where primary clearance was incomplete.This study has several limitations that warrant acknowledgment. First, the retrospective single-center design limits the generalizability of the findings and precludes causal inferences. Second, the absence of a concurrent control group receiving two-stage treatment prevents direct comparative efficacy evaluation within this dataset. Third, the relatively modest sample size of 55 patients - appropriate for a specialized single-center series - may limit statistical power for subgroup analyses. Fourth, long-term outcomes, including late biliary complications, symptom recurrence, and quality of life, were not assessed. Strengths of this study include the six-year consecutive cohort design minimizing selection bias, the consistent application of a standardized modified technique throughout the study period, and the use of validated classification systems (Clavien-Dindo, SOFA, APACHE II) for outcome reporting. Future research should include prospective randomized controlled trials comparing the modified rendezvous technique with conventional sequential ERCP-first approaches, assessment of long-term outcomes, and economic analyses to quantify the cost-effectiveness of single-stage management in the context of healthcare systems across different resource settings.
5. Conclusions
- The modified single-stage laparoendoscopic rendezvous technique demonstrated high efficacy and an acceptable safety profile in patients with cholecystocholedocholithiasis at average risk for cholangiolithiasis. Complete single-stage biliary tract sanitation was achieved in 85.7% of patients, with a median operative time of 120.0 minutes and a low postoperative complication rate of 12.7%. The operative duration was significantly prolonged in acute calculous cholecystitis compared to chronic inflammation (p = 0.035), while no intraoperative complications and zero mortality were recorded. The median length of hospital stay was 7.0 days, increasing significantly in patients who developed postoperative complications (p = 0.003).From a health policy perspective, the adoption of single-stage hybrid laparoendoscopic techniques for the management of cholecystocholedocholithiasis has the potential to substantially reduce the overall burden on healthcare systems by eliminating the need for multiple separate hospital admissions, reducing the cumulative anesthesia exposure per patient, and shortening the total duration of treatment. In settings where biliary surgical expertise and advanced endoscopic capabilities coexist within the same institution, institutional protocols should consider formalizing single-stage rendezvous-based pathways as a standard of care for patients with average-risk cholangiolithiasis, in alignment with evidence-based benchmarks for minimally invasive biliary surgery.Based on the findings of this study, it is recommended that: (1) specialized surgical centers with appropriate multidisciplinary expertise consider integrating the modified laparoendoscopic rendezvous technique into their standard biliary surgery protocols for patients with cholecystocholedocholithiasis and average-risk cholangiolithiasis; (2) prospective multicenter trials be conducted to validate these results across diverse institutional and patient population contexts; (3) structured training programs be established to ensure reproducibility of the technique and to facilitate safe adoption in centers with nascent laparoendoscopic experience; and (4) cost-effectiveness analyses be incorporated into future evaluations to support evidence-based resource allocation and health policy decision-making.
ACKNOWLEDGEMENTS
- The authors express their sincere gratitude to the surgical, anesthesiology, and endoscopy teams of the Central Hospital of the Samarkand City Health Department for their dedication and collaborative efforts in implementing the modified laparoendoscopic rendezvous technique throughout the study period. The authors also acknowledge the medical records personnel for their assistance with data retrieval.
Financial Support and Sponsorship
- This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. No external financial support or sponsorship was provided for this study.
Authors' Contributions
- Abduraxmonov Eshonkul Movutovich: Conceptualization, study design, surgical procedures, data collection, manuscript drafting, and final approval of the submitted version.Babajanov Axmadjon Sultanbayevich: Surgical procedures, data verification, critical revision of the manuscript for important intellectual content, and final approval of the submitted version.All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
- The authors declare no conflicts of interest. Neither author has any financial relationships with commercial entities that could be construed as potential conflicts relevant to this study.