Elmurodov Karimali Sadinovich1, Gulmurodov Muxtor Goyibovich2
1Karshi Branch of the Republican Research Center for Emergency Medicine, Uzbekistan
2Tashkent State Medical University, Uzbekistan
Correspondence to: Elmurodov Karimali Sadinovich, Karshi Branch of the Republican Research Center for Emergency Medicine, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
This study presents the results of a comprehensive analysis of 177 patients with necrotizing acute pancreatitis. The study aimed to improve surgical outcomes through the preferential use of minimally invasive techniques. Ultrasound-guided percutaneous drainage and videolaparoscopic interventions were used as primary treatment modalities for local complications. The implementation of minimally invasive approaches significantly reduced complication rates (23.1% vs. 37.3%) and mortality (6.6% vs. 11.6%) compared with conventional open surgery.
Keywords:
Acute necrotizing pancreatitis, Minimally invasive surgery, Pancreatic necrosis, Drainage, Complications
Cite this paper: Elmurodov Karimali Sadinovich, Gulmurodov Muxtor Goyibovich, A Differential Approach in the Surgery of Acute Pancreatitis and Its Complications, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2235-2238. doi: 10.5923/j.ajmms.20261605.05.
1. Introduction (Relevance)
Acute pancreatitis remains one of the most common urgent conditions in abdominal surgery. The incidence of severe and necrotizing forms has increased in recent years, particularly among patients with pancreatogenic shock and multiple organ failure. According to the Revised Atlanta Classification (2012), acute pancreatitis is categorized into mild, moderately severe, and severe forms, with local complications including acute necrotic collections (ANC) and walled-off necrosis (WON). Despite advances in treatment, mortality in severe necrotizing pancreatitis remains high [1-5].Minimally invasive approaches, including percutaneous drainage and step-up strategies, have become the standard of care. However, several issues remain unresolved, including optimal timing of intervention, indications for surgery, and management of infected necrosis [6-8].Aim of the Study. To improve the outcomes of surgical treatment in patients with local complications of acute necrotizing pancreatitis through the preferential use of minimally invasive techniques.
2. Material and Methods
The study is based on the results of a comprehensive study of 177 patients with pancreatic necrosis who were treated in the surgical departments of the Karshi branch of the Russian Scientific Center for Emer0gency Medicine from 2019 to 2024. All patients were divided into two groups. The main group consisted of 91 (51.4%) patients with pancreatic necrosis, Of these, 61 (67.1%) were men and 30 (32.9%) were women, and minimally invasive treatment methods were used in their treatment. The control group consisted of 86 (48.6%) patients, including 57 (66.3%) men and 20 (33.7%) women, who underwent traditional treatment methods.The age of patients with acute destructive pancreatitis in both study groups ranged from 22 to 82 years, with the majority of those of working age age from 21 to 59 years- 138 (77.9%) patients. There were 18 (19.7%) and 18 (20.9%) elderly patients in the first and second groups, respectively. There were 118 (66.6%) men and 59 (33.3%) women. The highest incidence rate among men and women was in the 20-49 age group, comprising 106 (59.8%) patients.All admitted patients were hospitalized in surgical departments on an emergency basis. A total of 81 (46.1%) patients were hospitalized within the first 24 hours of illness, 51 (28.4%) patients were admitted within the first three days, and 45 (25.3%) patients were hospitalized after three days.During the study, predisposing factors for the development of the disease were identified in the majority of cases from the anamnestic data - in 163 (92.1%) patients. However, in 14 (7.9%) patients, even with a thorough study of the anamnesis and a clinical examination involving modern research methods to establish the cause of the development of acute destructive pancreatitis And existing complications Not succeeded. At A study of the anamnesis revealed that the most common factor in the development of pancreatic necrosis was cholelithiasis, which was detected in 35 (38.5%) patients in the study group and in 37 (43.1%) patients in the control group. Nutritional disorders were identified as an etiological factor in the development of pathology in 20 (21.4%) patients in the study group and in 17 (19.7%) in the control group. Traumatic injuries to the pancreas (contusion) and gastrointestinal pathologies were somewhat less common causes of pancreatic necrosis. Most patients were found to have concomitant pathologies upon examination at the time of admission.
3. Results and Discussion
Treatment tactics for fluid accumulation in acute destructive pancreatitis. Presence of fluid accumulations in the patients we observed with acute pancreatitis was observed in 18 cases (19.7%). The size ranges were up to 3 cm, from 3 to 8 cm, and over 8 cm. The size of fluid collections in most patients with the necrotic form of acute pancreatitis (53%) exceeded 8 cm, while in 7 patients these collections were located in the tail of the pancreas, and in 11 patients they were localized in the omental bursa. Curved and radiopaque needles were used to perform puncture procedures. properties polyethylene drainages 9Ch And 12h " Pigtail " variant with the presence of a fixator. In 6 cases, patients, despite conservative therapy, experienced persistent pain. These manipulations were performed under ultrasound monitoring; in 5 patients, laparoscopic surgery was performed Omentobursostomy. In 10 cases, regression of fluid formations was observed after these procedures.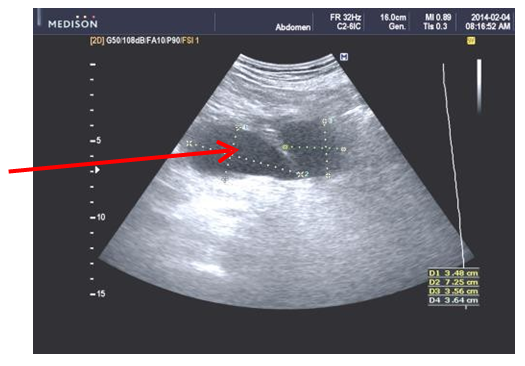 | Figure 1. Ultrasound. Accumulation of inflammatory exudate in the omental bursa cavity before conservative therapy |
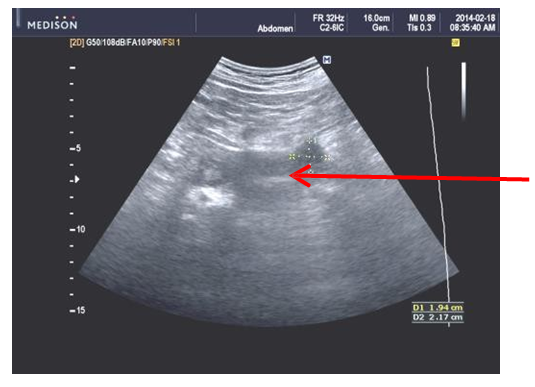 | Figure 2. Ultrasound. Against the background of conservative therapy, after 2 weeks |
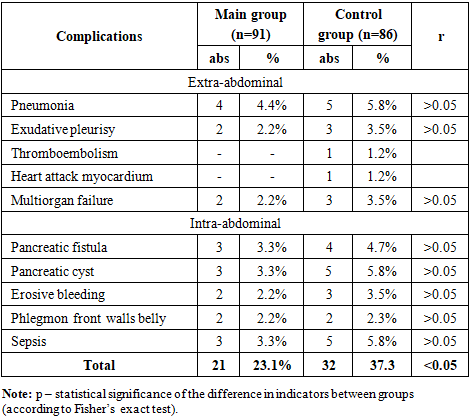
In 6 patients after ultrasound puncture drainage Two catheters were inserted for the purpose of performing flow-through irrigation. Regression was achieved in 5 patients. Mortality was noted in 1 patient with a purulent-septic complication; multiple organ failure developed in the late period. After laparoscopic drainage, regression of acute necrotic clusters, A V 1 case it was noted education External pancreatic fistula. Microbiological examination revealed a predominance of gram-negative flora (in 64% of cases). In 9 patients (9.9%), conservative therapy prevented the need for surgical intervention.Treatment tactics for sterile pancreatic necrosis. This study included 22 (24.2%) patients with a sterile form of acute pancreatitis and the formation of liquid clusters. Men was 10 women – 12. During intensive care, despite the indicated treatment tactics, an increase in the volume of fluid accumulation in the cavity of the lesser omentum over 6 cm in diameter was noted in 15 patients. As a result, a puncture was performed under ultrasound control followed by the imposition of a mini - omentobursostomy. Fluid was simultaneously collected for bacteriological examination. In 8 cases, patients with encapsulated sterile fluid accumulations or with the detection of fluid in the abdominal cavity showed signs indicating the need for laparoscopic treatment. The presence of limited fluid accumulations was noted in 22 (24.2%) patients, while in 15 of them, indications for puncture were established based on the size of the formation. In the treatment of aseptic accumulations, their puncture and drainage were used in 14 patients with subsequent omentobursostomy. In the course of further study, 8 patients showed regression of the disease after intensive complex anti-inflammatory therapy. In 14 patients, widespread damage to the pancreas and retroperitoneal space was noted. In 4 cases (4.4%) of patients with aseptic fluid accumulations in the omental bursa (omentobursitis), only puncture- drainage surgical interventions under ultrasound monitoring were performed. In addition, abdominal drainage was performed at the initial stages of therapy in 10 (10.9%) patients, in one case, a laparotomy was performed at a late stage of therapy, removal of sequestra and necrotic tissue with the imposition of omentobursostomy. The presence of acute aseptic fluid accumulations in the area of the omental bursa and retroperitoneal tissue was detected in 2 patients. Four (4.4%) patients with acute aseptic fluid accumulation in the retroperitoneal tissue initially underwent abdominal drainage due to enzymatic peritonitis. Fluid collection puncture under ultrasound monitoring was performed in four (4.4%) patients; one patient underwent laparotomy, removal of sequesters and necrotic tissue, and omentobursostomy. Purulent complications were observed in three (3.3%) cases. A fatal outcome was observed in one (1.1%) case due to prolonged sepsis. Lumbotomy and retroperitoneal tissue drainage were performed in five patients.Treatment tactics for infected pancreatic necrosis. This study included 31 (34.1%) patients with an infected form of pancreatic necrosis. All patients With infected pancreatic necrosis were used Staged differentiated surgical methods of therapy, which consisted of the following. Initially, puncture was performed under ultrasound monitoring; when selecting the catheter size, the viscosity and nature of the obtained puncture were taken into account, using standard " Pig" catheters. tail » 18-20 F, while choosing a large drainage diameter, creating additional multiple holes at the end of the drainage loop for complete sanitation with ozonated 0.9% saline solution heated to 38° With, installing drainage until complete cleaning, if possible, for 15-20 days on average. Puncture interventions under ultrasound control were performed on the 8-20th day from the onset of the disease in 4 (4.4%) patients, these are the periods in which, as a rule, the transformation of the sterile form of pancreatic necrosis into an infected one is observed. Combined performance of ultrasound puncture and drainage of the common bile duct was used in 3 (3.3%) patients. Laparotomy, necrsequestrectomy was performed on 16.1 ± 2.4 days on average from the onset of the disease with the progression of infected pancreatic necrosis after laparoscopic drainage of the omental bursa cavity was performed in 14 (15.4%) patients. In 4 (4.4%) patients, laparotomy in combination with lumbotomy was performed at the same time because of Spread of the purulent-septic process into the retroperitoneal space. Microbiological studies revealed a predominance of gram-negative flora in 54% of cases.Using drainage tubes installed in the abdominal cavity, omental bursa and retroperitoneal space, lavage was performed every day using antiprotease drugs (contrical, gordox, etc.) and NaCl solution in the amount of 1500 ml. During the initial study, the amylase level in the peritoneal fluid aspirated during surgery varied within the range of 2200-6100 U /l (normally this indicator is not exceeds 225 U /l), and in the fluid extracted from the omental bursa and retroperitoneal space, the amylase level was about 20 U /l (with a normal value below 5 U /l).Treatment tactics for pancreatogenic abscess. Pancreatogenic abscess V During the study, abscesses occurred in 7 (7.7%) patients in the main group. All patients underwent percutaneous drainage of the abscess cavity under ultrasound monitoring with drainage by inserting a silicone drainage tube. Microbiological examination of drainage discharge in all patients revealed antibiotic resistance among the identified microorganisms, such as Pseudomonas aeruginosa and Acinobacteria, at 16.6% (p> 0.05). And daily after surgery, under ultrasound monitoring and fistulographic control, the abscess cavity was irrigated using a 0.9% warm ozonized sodium chloride solution. In 2 patients with multiple chambers in the pancreatogenic abscess, it was necessary to insert additional drainage tubes. In two cases, percutaneous drainage was ineffective, as determined by clinical and laboratory tests and worsening endogenous intoxication. Laparotomy was performed. In two cases, pancreatogenic abscesses were detected in the subdiaphragmatic space on the left and right sides. As a result, posterior drainage was performed parallel to the 12th rib to provide extra-abdominal access to the lesion.Treatment tactics for patients with acute destructive pancreatitis complicated by retroperitoneal cellulitis. Retroperitoneal cellulitis was diagnosed in 6 patients (6.6%) in the surgical department. Minimally invasive ultrasound-guided procedures were performed in all patients. Drainage was carried out way Seldinger. At Microbiological testing revealed Pseudomonas aeruginosa and Acinobacteria to be 10.0% (p>0.05). During the treatment, improvement in the general condition was observed in all patients, but at this is a complete recovery was noted only in 3 (3.3%) cases. U Two patients showed a short-term improvement in their condition after minimally invasive interventions; due to repeated deterioration of their condition, an abdominal cavity was opened, sequesters were removed, an omentobursostomy was performed, and a drainage tube was installed in the retroperitoneal tissue according to Lauenstein-Clermont; a fatal outcome was recorded in one patient.An analysis of the immediate results of surgical interventions was conducted in all patients included in the study in both observed groups (Table 1). Summarizing the results of the studies, among the total number of observed extra-abdominal complications, a prevalence of complications was noted. with sides organs breathing And cardiovascular systems. U 4 (4.4%) of patients developed pneumonia during the first 7 days of hospital stay, which had an adverse effect on the course of the postoperative period.Table 1. Structure and comparative characteristics of postoperative complications in patients of the main and control groups
 |
| |
|
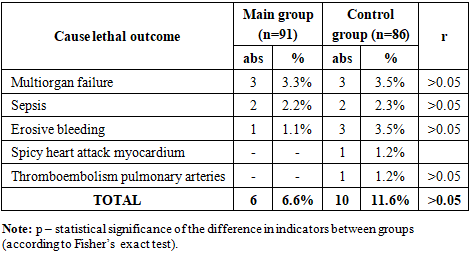
2.2% of patients developed inflammation Pleural effusion with fluid accumulation. Three of these patients required removal of this fluid by puncture or drainage. Furthermore, two patients experienced dysfunction of multiple organs simultaneously (Table 2). It is worth noting that the presence of serious concomitant respiratory and cardiovascular diseases, as well as advanced age, were unfavorable factors for the course of the underlying pathology.Table 2. Structure and comparative characteristics of mortality in patients of the main and control groups
 |
| |
|
It was found that among the causes of death, the prevalence of cases of arrosive bleeding was noted - in 4 (2.6%) patients.The results of the study showed that with the use of improved treatment methods, the rate of positive results increases, O how testifies decrease frequencies development inside and extra-abdominal complications in the main group of patients up to 23.1%, while this figure in the control group was 37.3%. (p< 0.05) The fatality rate in these groups was 6.6% and 11.6%, respectively.Thus, according to the results we obtained in patients with pancreatic necrosis, thanks to the use of improved methods of diagnosis and treatment based on monitoring the indicators of general clinical and microbiological studies, the results of assessing the severity of the patient, as well as thanks to the improvement of methods surgical treatment, an improvement in the effectiveness of therapy was noted at all its stages.Discussion. The results confirm the effectiveness of minimally invasive strategies in the management of necrotizing pancreatitis. Compared with traditional open surgery, minimally invasive approaches: - reduce surgical trauma; - lower complication rates; - improve survival. These findings are consistent with current international guidelines recommending a step-up approach as the standard treatment strategy. However, the retrospective design and lack of randomization may introduce selection bias, which should be considered when interpreting the results.Ethical Considerations. The study was conducted in accordance with ethical standards. Approval was obtained from the institutional ethics committee, and all patients provided informed consent for treatment.
4. Conclusions
1. Minimally invasive interventions should be considered the first-line treatment for local complications of necrotizing pancreatitis.2. The step-up approach significantly reduces morbidity and mortality compared to open surgery.3. Individualized treatment strategies improve clinical outcomes.
References
| [1] | Rizaev E. A., Kurbanyiazov Z. B., Abdurakhmanov D. Sh. Differentiated approach to surgical treatment of severe acute pancreatitis with prediction of treatment results. UZbek Journal of Case Reports, 2024; 4(3): 6-11. |
| [2] | Khaidarov N. B., Rakhmanov K. E., Suvonov Sh. Sh., Mukhiddinov T. Zh. Differentiated surgical tactics in acute destructive pancreatitis: the effectiveness of minimally invasive interventions and the impact on outcomes. Biology of the tibbiyot Muammolari 2024; (157): 211-214. |
| [3] | Matteucci M., Ranucci M. C. Minimally invasive approach versus open approach in the management of necrotizing acute pancreatitis: A systematic review and meta-analysis. Annals of Hepato-Biliary-Pancreatic Surgery, 2025; 29(3). |
| [4] | Reyes Correa B., Padilla Quintana J., Goya Pacheco A. Surgical Update on the Management of Necrotizing Pancreatitis: Step-Up Approach. In: IntechOpen, 2025. |
| [5] | N. Alzerwi. Surgical management of acute pancreatitis: Historical perspectives, challenges, and current management approaches. |
| [6] | Beij A, Verdonk RC, van Santvoort HC, de‐Madaria E, Voermans RP. Acute Pancreatitis: An Update of Evidence‐Based Management and Recent Trends in Treatment Strategies. United European gastroenterology journal. 2025 Feb; 13(1): 97-106. |
| [7] | Mittal N, Oza VM, Muniraj T, Kothari TH. Diagnosis and management of acute pancreatitis. Diagnostics. 2025 Jan 23; 15(3): 258. |
| [8] | Li R, Luo P, Guo Y, He Y, Wang C. Clinical features, treatment, and prognosis of SGLT2 inhibitors induced acute pancreatitis. Expert opinion on drug safety. 2025 Nov 2; 24(11): 1253-7. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML