-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2213-2217
doi:10.5923/j.ajmms.20261605.01
Received: Mar. 26, 2026; Accepted: Apr. 20, 2026; Published: May 1, 2026

Prognostic Significance of Candida spp. Colonization in the Development of Oral Mucositis During Radiotherapy with Simultaneous Integrated Boost in Patients with Oral Cavity Cancer
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. J. Kahharov, N. O. Zaynutdinov
Tashkent State Medical University, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Radiation-induced oral mucositis (OM) remains a major dose-limiting toxicity in patients with head and neck cancer, significantly impairing treatment adherence and quality of life. Emerging evidence suggests that oral microbiota, particularly Candida spp., may influence mucosal toxicity. Objective: To evaluate the prognostic significance of oral Candida spp. colonization in the development, severity, and early onset of OM during radiotherapy with simultaneous integrated boost (SIB). Methods: A prospective cohort study included 152 patients undergoing IMRT/VMAT. Baseline oral swabs were analyzed using culture-based methods. OM severity was assessed weekly according to CTCAE v4.0. Early-onset OM (EOM) was defined as grade III-IV toxicity at ≤40 Gy. Multivariate logistic regression was performed to identify independent risk factors. Results: OM developed in 78.9% of patients, with grade III observed in 23.7%. Candida spp. colonization was not significantly associated with overall OM severity but was an independent predictor of EOM (OR=5.13; 95% CI: 1.23-21.4; p=0.04). Tumor localization (OR=1.29; p=0.05) and lymphocytopenia (OR=8.2; p=0.03) were independently associated with severe OM. Colonized patients developed OM earlier (38.3 vs. 45.6 Gy; Δ≈4 days). Conclusions: Baseline Candida spp. colonization is a clinically relevant predictor of early-onset severe OM rather than overall severity. Pre-treatment microbiological screening may enable risk-adapted preventive strategies, including antifungal prophylaxis.
Keywords: Oral mucositis, Radiotherapy, Head and neck cancer, Candida spp., Risk factors
Cite this paper: A. J. Kahharov, N. O. Zaynutdinov, Prognostic Significance of Candida spp. Colonization in the Development of Oral Mucositis During Radiotherapy with Simultaneous Integrated Boost in Patients with Oral Cavity Cancer, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2213-2217. doi: 10.5923/j.ajmms.20261605.01.
1. Introduction
- Malignant neoplasms of the head and neck remain a significant medical and social challenge in modern oncology due to increasing incidence, high disability rates, and reduced quality of life. Oral cavity cancer occupies a leading position within this group, characterized by aggressive behavior and a high risk of locoregional spread. Approximately 389,000 new cases of oral cavity cancer are diagnosed worldwide each year, accounting for about 2% of all malignancies and up to 40-45% of head and neck tumors [1].In countries of South and Central Asia, including Uzbekistan, the disease is often diagnosed at advanced stages (III-IV), necessitating combined treatment approaches involving surgery, radiotherapy, and chemoradiotherapy. Radiotherapy represents a key organ-preserving treatment modality; however, it is associated with early toxic complications affecting the oral mucosa.The most common dose-limiting toxicity is radiation-induced oral mucositis, which develops as a result of damage to rapidly proliferating epithelial cells under the воздействие of ionizing radiation and cytotoxic agents. The development of mucositis is accompanied by severe pain, dysphagia, nutritional impairment, and often leads to treatment interruptions, negatively affecting locoregional tumor control and patient survival [2]. Its incidence reaches up to 80% during radiotherapy and nearly 100% during chemoradiotherapy, with severe forms observed in up to 40% of patients [3].The severity of mucositis depends on dosimetric parameters, tumor localization, concomitant chemotherapy, oral health status, and hematological factors; however, reliable clinical predictors of its development remain insufficiently studied [4].Oral colonization by Candida spp., a common opportunistic infection, has gained particular importance. Fungal colonization may exacerbate inflammatory changes in the oral mucosa and aggravate the course of mucositis, while disruption of the epithelial barrier increases the risk of secondary infectious complications [5,6].Therefore, the aim of this prospective cohort study was to evaluate the role of oral Candida spp. colonization as a risk factor for the development of severe and early oral mucositis in patients undergoing radiotherapy for oral cavity cancer.
2. Materials and Methods
- The study protocol was approved by the local ethics committee of the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology of the Ministry of Health of the Republic of Uzbekistan. The study was conducted in accordance with the principles of the Declaration of Helsinki and the STROBE guidelines. Written informed consent was obtained from all participants.This study was designed as a prospective cohort study and included 152 patients undergoing radiotherapy using IMRT/VMAT techniques. Patients with histologically confirmed malignant tumors of the oral cavity referred for radical external beam radiotherapy between 2024 and 2025 were consecutively enrolled. Exclusion criteria included palliative treatment, clinical signs of oral candidiasis prior to therapy, neoadjuvant chemotherapy, and the presence of distant metastases.Before treatment initiation, all patients underwent a comprehensive clinical and dental examination, including assessment of the oral mucosa. Demographic characteristics, comorbidities, tumor localization and stage (according to TNM classification), as well as risk factors such as tobacco use, were recorded.To detect Candida spp. colonization, oral swabs were collected from the mucosal surface under sterile conditions, followed by microbiological culture on Sabouraud agar with incubation at 37°C for 48 hours (culture-based method). In addition, both stimulated and unstimulated salivary flow rates were evaluated. Baseline laboratory parameters included leukocyte, neutrophil, and lymphocyte counts.Radiotherapy was delivered using linear accelerators with conformal techniques (IMRT/VMAT) in a standard fractionation schedule of five fractions per week over 6-7 weeks. Treatment planning was performed in accordance with international guidelines, with daily image-guided radiotherapy (IGRT) verification of patient positioning.During treatment, patients were assessed weekly for radiation-induced mucosal toxicity. The severity of oral mucositis was graded according to the Common Terminology Criteria for Adverse Events (CTCAE), version 4.0. The occurrence of severe mucositis (grade III-IV) at a cumulative radiation dose ≤40 Gy was defined as early-onset mucositis (EOM).Statistical analysis was performed using IBM SPSS Statistics version 25.0. Quantitative data were presented as mean ± standard deviation or median with interquartile range. Group comparisons were conducted using the Mann-Whitney U test, Kruskal-Wallis test, analysis of variance (ANOVA), Pearson’s chi-square test, and Fisher’s exact test. Multivariate logistic regression analysis was used to identify independent risk factors for severe and early-onset mucositis. A p-value <0.05 was considered statistically significant.
3. Results
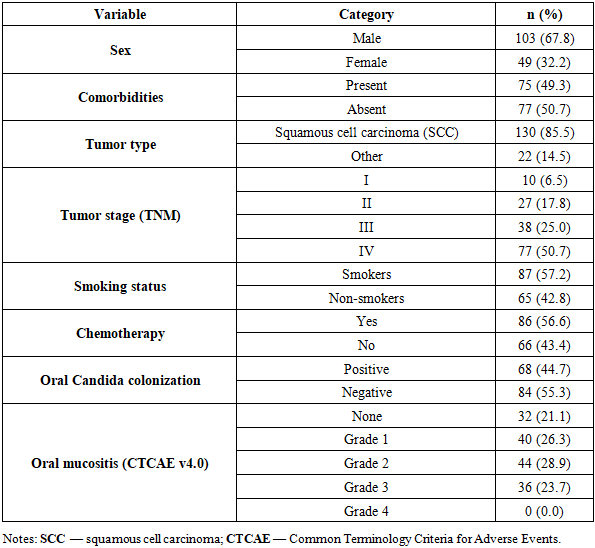
- A total of 163 patients were initially enrolled in the study. After application of the predefined exclusion criteria, 11 patients were excluded: 5 due to clinically evident oral candidiasis at baseline examination and 6 due to indications for palliative treatment. The final study cohort therefore comprised 152 patients (49 females and 103 males) with a mean age of 60.3 years (range 22-86 years).The majority of patients (75.7%) presented with locally advanced stage III-IV disease, reflecting the typical late-stage presentation of oral cavity cancer in routine clinical practice. Definitive chemoradiotherapy was administered to 93 patients (61.2%), whereas 59 patients (38.8%) received adjuvant radiotherapy following surgical treatment.Baseline clinical, demographic, and treatment-related characteristics are summarized in Table 1. As shown, squamous cell carcinoma was the predominant histological type (85.5%), and more than half of the patients (56.6%) received concomitant chemotherapy. Oral Candida spp. colonization prior to treatment was detected in 68 patients (44.7%), indicating a substantial prevalence of subclinical fungal carriage in this population.
|
|
|

4. Discussion
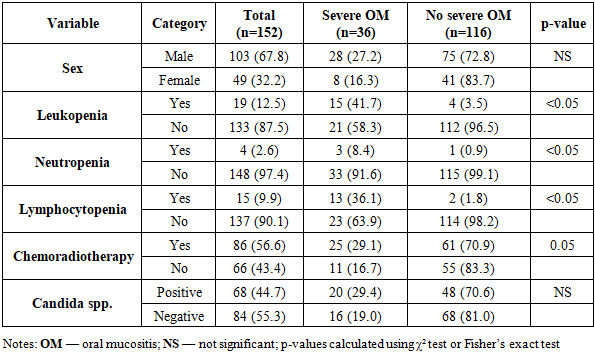
- Radiotherapy remains one of the main treatment modalities for malignant tumors of the oral cavity, providing locoregional control and improving patient survival. However, intensification of anticancer therapy is accompanied by an increased incidence of radiation-induced complications, among which oral mucositis (OM) is the most common and clinically significant, substantially affecting treatment tolerability and patients’ quality of life.OM is an inflammatory-destructive lesion of the oral mucosa that develops as a result of complex biological processes, including activation of inflammatory signaling pathways, impairment of microcirculation, and dysregulation of immune mechanisms [7,8]. Its development is influenced not only by the direct cytotoxic effects of therapy but also by the state of the oral microbiota, immune status, and individual patient characteristics [9].In the present study, the role of Candida spp. colonization in the development of OM was evaluated. Importantly, our findings provide evidence that fungal colonization does not significantly influence the overall severity of mucositis but plays a critical role in the temporal dynamics of its development, particularly by accelerating the onset of severe toxicity (OR = 5.13; p = 0.04). This distinction is clinically relevant, as early-onset mucositis is associated with more pronounced pain, increased need for supportive care, and a higher risk of treatment interruptions [10].These findings are consistent with emerging concepts of mucositis as a multifactorial biological process, in which microbial dysbiosis interacts with radiation-induced epithelial injury and immune dysregulation. Mechanistically, Candida spp. may contribute to mucosal damage through several pathways, including the secretion of proteolytic enzymes that disrupt epithelial integrity, activation of NF-κB-mediated inflammatory signaling, induction of pro-inflammatory cytokines (such as IL-1β and TNF-α), and synergistic interactions with bacterial microbiota, particularly through biofilm formation [11].Radiotherapy further enhances fungal pathogenicity by compromising mucosal integrity, reducing salivary flow, inducing local hypoxia, and altering the composition of oral secretions [6,13]. These changes create a favorable microenvironment for fungal overgrowth and amplify the inflammatory response.Importantly, the present results support the concept of microbiome-driven modulation of radiation toxicity, which is increasingly recognized in recent MASCC/ISOO frameworks. From a clinical perspective, early-onset mucositis represents a critical condition, as it increases analgesic requirements, compromises nutritional intake, and frequently leads to interruptions in anticancer treatment. Therefore, identification of Candida spp. colonization prior to therapy may serve as a predictive biomarker for early toxicity and enable the implementation of personalized supportive strategies, including targeted antifungal interventions.Additionally, tumor localization and lymphocytopenia were confirmed as independent risk factors for severe OM. The higher incidence of complications in certain anatomical sites is likely related to larger irradiation volumes and dose distribution patterns, whereas lymphocytopenia may contribute to impaired immune regulation of inflammatory responses [14].The strengths of this study include its prospective design and the relative homogeneity of the treatment protocol. However, several limitations should be acknowledged, including the single-center design and the absence of comprehensive oral microbiome analysis, which may limit the generalizability and mechanistic interpretation of the findings.
5. Conclusions
- 1. Oral mucositis remains a highly prevalent complication (78.9%) during radiotherapy. 2. Candida spp. colonization is not associated with overall severity, but is a strong predictor of early-onset severe mucositis. 3. Tumor localization and lymphocytopenia are independent risk factors for severe OM. 4. Pre-treatment oral microbiological screening may improve risk stratification and support personalized preventive strategies, including antifungal interventions.