-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2031-2036
doi:10.5923/j.ajmms.20261604.96
Received: Apr. 4, 2026; Accepted: Apr. 22, 2026; Published: Apr. 25, 2026

EQ-5D-5L and VascuQoL-6 in Assessing the Quality of Life of Patients with Critical Lower Limb Ischemia After Endovascular Treatment
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMaksud Muminovich Shermatov, Mirjamol Mirumarovich Zufarov
Republican Specialized Scientific and Practical Medical Center of Surgery named after academician V.Vakhidov, Tashkent, Uzbekistan
Correspondence to: Maksud Muminovich Shermatov, Republican Specialized Scientific and Practical Medical Center of Surgery named after academician V.Vakhidov, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

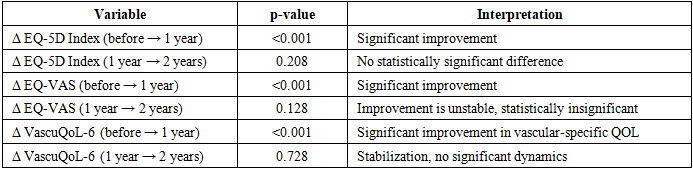
Objective. To evaluate the dynamics of quality of life (QoL) in patients with critical lower limb ischemia (CLLI) after X-ray endovascular interventions and to identify clinical predictors that determine long-term results. Material and methods. The study included 84 patients with CLLI, all of whom underwent endovascular procedures (balloon angioplasty, stenting, combined interventions). The average age was 67.1±9.5 years; male — 65.5%. The universal EQ-5D-5L scale and the vascular-specific VascuQoL-6 scale were used to assess QOL. The assessment was carried out before the intervention, as well as 6 months, 1 year, 2 years and 3 years after treatment. Clinical outcomes were compared with medical records and included amputations, repeat revascularizations and patient mobility. Statistical analysis included parametric and nonparametric statistics methods, logistic regression to determine the factors associated with low QoL. Results. A statistically significant improvement in QoL was found during the first year after the intervention: EQ-5D-5L increased from 0.48 to 0.77 (p<0.001), VascuQoL-6 - from 2.8 to 5.0 (p<0.001). Subsequently, stabilization of the indicators was noted without a significant increase (p>0.1). By the 3rd year of observation, the differences in EQ-5D-5L between the main group and the comparison group remained (0.76 versus 0.60). Comparison of the subgroups with and without amputation after 2 years did not reveal statistically significant differences (p>0.3), indicating the leading role of functional status and rehabilitation. Multivariate analysis showed that independent predictors of decreased QoL were older age (p<0.001), non-ambulatory status (p<0.001) and severe pain syndrome (p<0.001), while intensive rehabilitation, high quality of revascularization and psychosocial support had a significant positive effect (p<0.001). Conclusion. Endovascular revascularization in patients with CLI provides a significant improvement in QoL during the first year after the intervention with subsequent stabilization of the effect. Long-term QoL indicators are determined not so much by the fact of amputation as by the functional status, quality of vascular reconstruction, pain level and the effectiveness of rehabilitation. The obtained results substantiate the need for a multidisciplinary approach with an emphasis on pain control, restoration of mobility and social adaptation. Our results recommend considering quality of life assessment (EQ-5D-5L and VascuQoL-6) as a mandatory component of monitoring the effectiveness of CLI treatment in clinical practice.
Keywords: Critical lower limb ischemia, Quality of life, EQ-5D-5L, VascuQoL-6, Endovascular revascularization, Predictors, Rehabilitation
Cite this paper: Maksud Muminovich Shermatov, Mirjamol Mirumarovich Zufarov, EQ-5D-5L and VascuQoL-6 in Assessing the Quality of Life of Patients with Critical Lower Limb Ischemia After Endovascular Treatment, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2031-2036. doi: 10.5923/j.ajmms.20261604.96.
Article Outline
1. Introduction
- Critical limb-threatening ischemia (CLTI) represents the most severe form of peripheral artery disease (PAD), associated with high mortality, amputation risk, and a profound decline in quality of life (QoL); terminology and the prioritization of QoL assessment were established in the Global Vascular Guidelines (GVG, 2019) [1]. For quantitative evaluation of QoL in CLTI, both generic and vascular-specific PROMs are utilized.Among validated instruments, the most widely applied are EQ-5D-5L (generic, suitable for utility calculation) and VascuQoL-6/25 (vascular-specific, with established responsiveness to clinical change and defined MID/SCB thresholds) [2–4]. These instruments demonstrate acceptable validity and responsiveness in PAD/CLTI patients, ensuring both cross-group comparability (EQ-5D-5L) and symptom-specific sensitivity (VascuQoL-6).Pooled evidence from a meta-analysis (EJVES, 2022) indicates moderate improvement in QoL following revascularization in CLTI, with low-to-moderate certainty of evidence and comparable trajectories after open and endovascular interventions; after Major lower extremity amputation (MLEA) or conservative management, QoL is generally maintained at baseline levels [5]. Randomized data from BEST-CLI (Circulation, 2024) demonstrated a sustained improvement in HRQoL across major scales following revascularization in CLTI patients [6].Predictors of low preoperative HRQoL in BEST-CLI patients included lack of independent ambulation, smoking, opioid use, and female sex, confirmed by multivariable analyses across several instruments (VascuQoL, EQ-5D, SF-12) [7]. These findings support the inclusion of functional status and behavioral factors in the design of QoL studies in CLTI.For purposes of comparability with clinical outcomes and cost-effectiveness assessment, a combined strategy of EQ-5D-5L (utility, comparability) plus VascuQoL-6 (vascular-specific sensitivity) is advisable; this approach is consistent with evidence on the high suitability of EQ-5D in PAD patients and the validated responsiveness of VascuQoL-6 [2,3,8,9]. ObjectiveTo evaluate the dynamics of QOL in patients with CLLI after X-ray endovascular interventions and to identify clinical predictors that determine long-term results.
2. Material and Methods
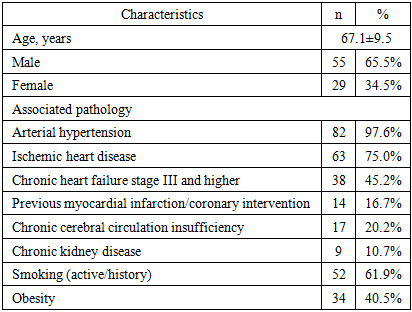
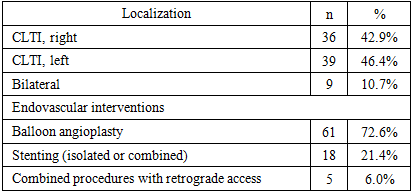
- A prospective cohort study was conducted with a follow-up period of three years, including multiple assessment time points: baseline (prior to intervention), 6 months, 1 year, 2 years, and 3 years after treatment.The study enrolled 84 patients with a confirmed diagnosis of CLTI according to the Global Vascular Guidelines (GVG, 2019) [1]. Exclusion criteria included individuals with end-stage comorbidities and patients unable to complete questionnaires.For comprehensive evaluation of QoL, a combination of EQ-5D-5L and VascuQoL-6 was employed. This approach allowed for simultaneous assessment of global and disease-specific domains with minimal burden on patients.In addition to questionnaire-based assessment, clinical events were recorded: amputations (presence, level-major/minor, and timing); repeat revascularizations (intervention type—angioplasty or bypass, and interval); and mobility (independent ambulation, use of assistive devices). Data sources included medical records, operative logs, and standardized questionnaires.The mean age was 67.1±9.5 years (range 42–86 years, median 67 years). The cohort consisted of 55 men (65.5%) and 29 women (34.5%). The majority were elderly patients (60–74 years, 62%), followed by senile patients (≥75 years, 19%), while younger individuals (<60 years) were less frequent (19%).Multimorbidity was characteristic of the entire cohort. Arterial hypertension was present in 82 patients (97.6%). Coronary artery disease was diagnosed in 63 patients (75.0%), and chronic heart failure (stage III or higher) in 38 (45.2%). A history of myocardial infarction or coronary intervention (PCI/CABG) was noted in 14 patients (16.7%).
|
|
3. Results
- The results demonstrate a positive trend in QoL at all follow-up stages (Fig. 1). According to EQ-5D-5L, scores increased from 0.48 at baseline to 0.76 at 3 years. According to VascuQoL-6, values rose from 2.8 to 4.0.
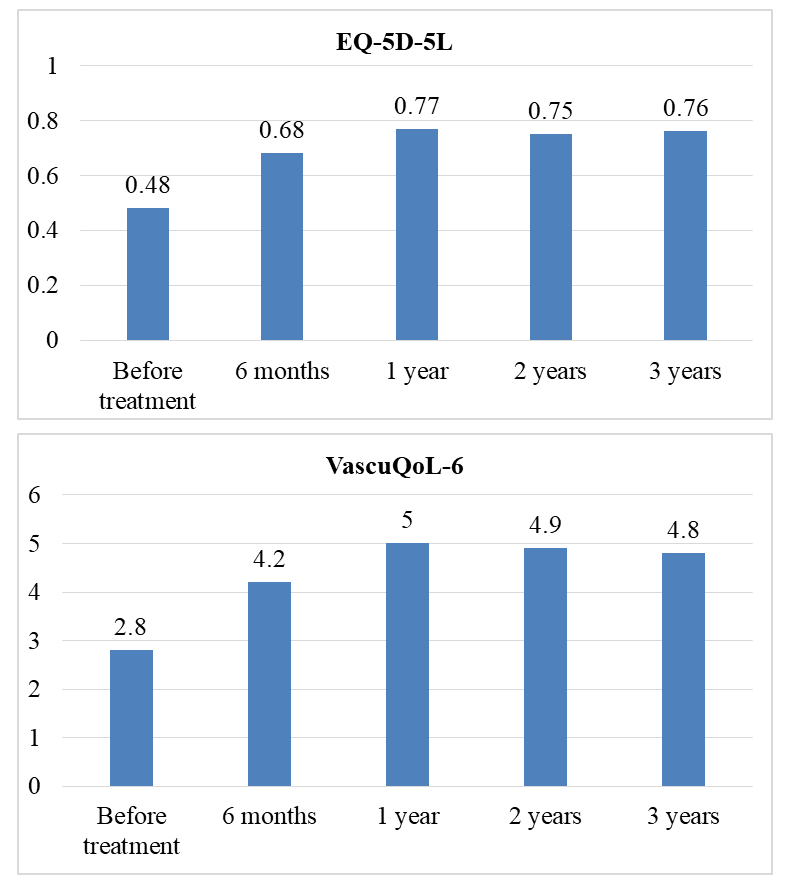 | Figure 1. Dynamics of EQ-5D-5L and VascuQoL over time |
|

|
|
4. Discussion
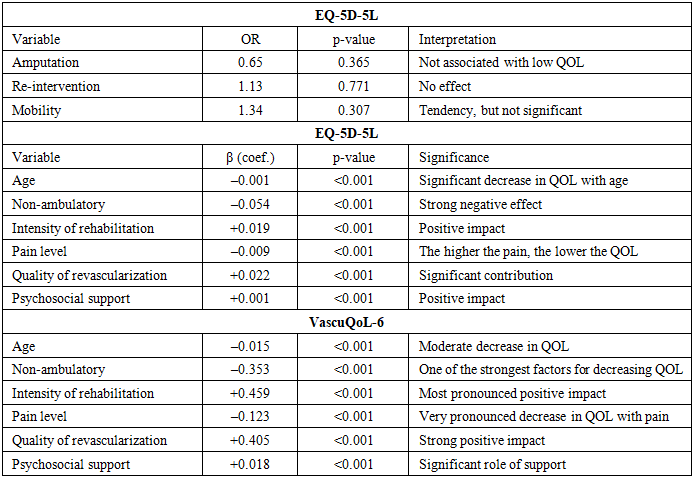
- Thus, in the long-term postoperative period, QoL in patients with CLTI is determined not so much by the fact of amputation, but rather by functional status (mobility), the quality of vascular reconstruction, the intensity of rehabilitation, pain level, and social adaptation. Age and the presence of hypertension are also significant, although less modifiable, predictors. These findings confirm the clinical importance of a strategy that emphasizes multidisciplinary rehabilitation, effective pain management, and optimization of vascular restoration in improving QoL. The study results demonstrate a significant and sustained improvement in QoL among patients with CLTI following endovascular revascularization, which is consistent with findings from large randomized and prospective trials. According to BEST-CLI (2024), patients with chronic limb-threatening ischemia (CLTI) who underwent revascularization (either endovascular or bypass) exhibited statistically significant improvements in HRQoL measured by VascuQoL, EQ-5D, SF-12, and other scales-independent of the intervention type [6].A meta-analysis by Shan LL et al. (2022) confirmed similar trends: revascularization substantially improved both general and disease-specific QoL in patients with CLTI [5]. This further strengthens the rationale for endovascular procedures as not only limb-saving but also transformative for patient experience.Our data demonstrate stable QoL dynamics regardless of amputation status, particularly during the 1-2-year period—are in line with findings from Peters et al. (2020), where even elderly patients with limited life expectancy or without further treatment options maintained relatively stable QoL until the end of follow-up [10]. This highlights the critical role of adaptation, restoration of mobility, and pain control.In the study by Paius et al. (2023), interventions delivered within a multidisciplinary framework (vascular surgeon + rehabilitation specialist + psychologist) were shown to produce substantial improvements in HRQoL among CLTI patients [11]. Our results, confirming the positive impact of intensive rehabilitation and psychosocial support on long-term QoL, further validate the effectiveness of such approaches.In the long-term period, the main predictors of reduced QoL were identified as older age, inability to ambulate independently, and severe pain. Conversely, intensive rehabilitation, high-quality revascularization, and psychosocial support emerged as independent factors associated with improved QoL.These findings are concordant with the literature: in BEST-CLI (Powell et al., 2022), predictors of low QoL included female sex, smoking, and impaired mobility—underscoring that interventional treatment should be accompanied by strategies focused on mobility restoration and pain reduction [7].Our study has clear strengths, including the combined use of EQ-5D-5L and VascuQoL-6, its prospective design, and long follow-up period. Nevertheless, limitations include the lack of randomization and the absence of a non-intervention control group, which reduce the level of evidence. Moreover, the presence of amputations and repeat interventions may have exerted non-global influences on QoL perception, requiring further in-depth analysis.Future steps should involve the inclusion of comparative cohorts and the application of more advanced tools for psycho-emotional assessment (e.g., SF-36, Beck Depression Inventory), which would allow deeper exploration of the mechanisms through which interventions impact quality of life.
5. Practical Significance and Recommendations
- Our findings recommend considering QoL assessment (EQ-5D-5L and VascuQoL-6) as a mandatory component of monitoring treatment effectiveness in CLTI clinical practice. The combination of a generic and a disease-specific instrument enables objective evaluation of intervention outcomes and allows for reliable tracking of dynamics throughout long-term follow-up.Given the identified predictors, optimization of vascular reconstruction, intensive rehabilitation measures, adequate pain control, and the provision of psychosocial support should be regarded as priority strategies in the management of CLTI patients. These measures have not only clinical relevance but also proven significance in improving the long-term QoL of patients.
6. Conclusions
- Endovascular revascularization in patients with CLI provides a significant improvement in QoL during the first year after the intervention with subsequent stabilization of the effect. Long-term QOL indicators are determined not so much by the fact of amputation as by the functional status, quality of vascular reconstruction, pain level and the effectiveness of rehabilitation. The obtained results substantiate the need for a multidisciplinary approach with an emphasis on pain control, restoration of mobility and social adaptation.