-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2019-2021
doi:10.5923/j.ajmms.20261604.93
Received: Mar. 23, 2026; Accepted: Apr. 12, 2026; Published: Apr. 25, 2026

Visual Function and Refraction in Pterygium Before and After Xenoplasty
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMuxamadiev Raxmon Omonovich1, Ochilova Nafisa Nomozovna2
1Professor, Department of Otorhinolaryngology, Ophthalmology, Oncology and Medical Radiology, Termez Branch of Tashkent State Medical University, Uzbekistan
2Doctor-Ophthalmologist at the "NAFIS" Eye Clinic, Samarkand, Uzbekistan
Correspondence to: Muxamadiev Raxmon Omonovich, Professor, Department of Otorhinolaryngology, Ophthalmology, Oncology and Medical Radiology, Termez Branch of Tashkent State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective. In recent years, the number of patients with pterygium has been growing in the Republic of Uzbekistan, especially in the southern regions. The purpose and objectives of the study To evaluate visual functions in pterygium at different stages of development before and after xenoplasty. To determine the functional states of the eye at different degrees of pterygium development. Material and Methods. The study was conducted in 34 cases with grades I and U of pterygium development before and after xenoplasty. Results and Discussion. As the pterygium grew towards the optic part of the cornea, astigmatism increased and a decrease in visual functions was noted. Due to destructive changes and fibrovascular tissue at the site of growth, the sphericity of the cornea was disrupted, which in turn caused astigmatism, reducing visual acuity.
Keywords: Pterygium, Xenoplasty, Refraction, Astigmatism, Visual acuity
Cite this paper: Muxamadiev Raxmon Omonovich, Ochilova Nafisa Nomozovna, Visual Function and Refraction in Pterygium Before and After Xenoplasty, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2019-2021. doi: 10.5923/j.ajmms.20261604.93.
1. Introduction
- In recent years, in the Republic of Uzbekistan, particularly in the southern regions, the number of patients with pterygium has been increasing. Due to the desiccation of the Aral Sea and the frequent occurrence of dust storms, constant exposure to solar radiation provokes the growth of pterygium and aggravates its course, often leading to visual impairment [5].According to various sources, the incidence of pterygium ranks fifth among eye diseases in countries with hot climates. When the pterygium extends to the optical zone of the cornea, visual functions decrease sharply due to astigmatism and dystrophic changes in the deeper layers of the cornea [4].Therefore, the problem of pterygium remains highly relevant and continues to stimulate further in-depth research [1]. With the progression of pterygium, the main complications, apart from cosmetic defects, include impairment of visual functions and, in severe cases, a marked reduction in visual acuity. For this reason, a detailed assessment of visual functions is considered one of the key criteria in determining whether surgical or conservative treatment should be selected for pterygium [6,7,8].From 1950 to 2008, continuous scientific studies have been conducted to investigate the problem of pterygium. This is evidenced by the research carried out by regional scientists and neighbouring researchers, including Bushueva N.N. in the Kurgan-Tyube region of Tajikistan, Ismailov B.I. (1978), Saliev M.S. (1969) in the Samarkand region of Uzbekistan, Karanov K.S. (1976) in Turkmenistan, and Medvedev M.A. (1998) in Kyrgyzstan. Their studies were mainly aimed at investigating the aetiology and pathogenesis of pterygium as well as preventing its recurrence. One of the most recent works by Bilolov E.N. (2008, Uzbekistan) was devoted to analysing the biochemical composition of tear fluid in pterygium and the histological structure of excised pterygium tissue [1].Aim of the StudyTo evaluate visual functions in patients with pterygium at different stages of development before and after xenoplasty.Research ObjectivesTo determine the functional condition of the eye at different stages of pterygium development.
2. Materials and Methods
- The study included 34 cases of pterygium with varying degrees of progression. The age of the patients ranged from 32 to 54 years. Among them, 15 were men and 19 were women.All examined cases were divided into three groups:• Grade II pterygium – 10 cases;• Grade III pterygium – 11 eyes;• Grade IV–V pterygium – 13 cases.All patients underwent biomicroscopy. A detailed examination of the nasal segment of the cornea, the limbus, and the bulbar conjunctiva was performed. Particular attention was paid to the configuration of the pterygium head, the presence and severity of the avascular zone within the head of the pterygium, its localisation, and the degree of pterygium growth towards the pupillary margin of the cornea.Refraction was also assessed in all patients. Emmetropia was observed in 3 patients (5 eyes). Hypermetropic astigmatism ranging from 1.5 to 3.0 dioptres was detected in 21 patients.
3. Results and Discussion
- In all 34 cases of pterygium with stage II–V progression, astigmatism of varying degrees was detected, predominantly of hypermetropic and mixed types. As the pterygium progressed and astigmatism developed, accompanied by dystrophic changes in the layers of the cornea, a decrease in visual acuity was observed, ranging from 0.04 to 0.7.
 | Table 1. Refraction Before and After Xenoplasty |
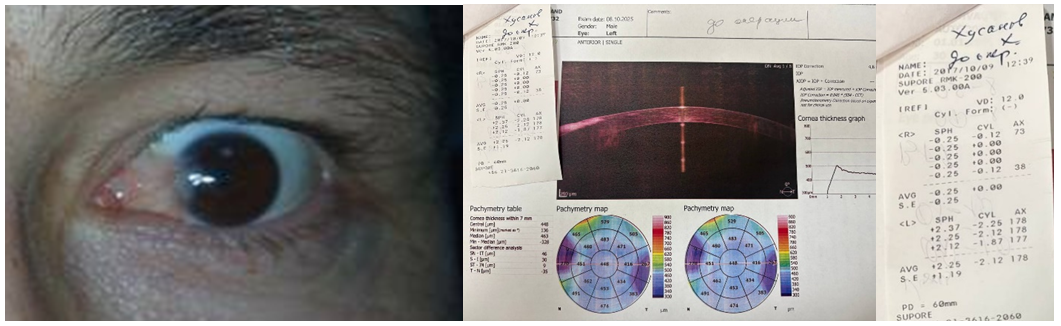 | Figure 1. A. Grade III pterygium before surgery. B. Refraction showing astigmatism of +2.0 D before surgery; uncorrected visual acuity 0.5 |
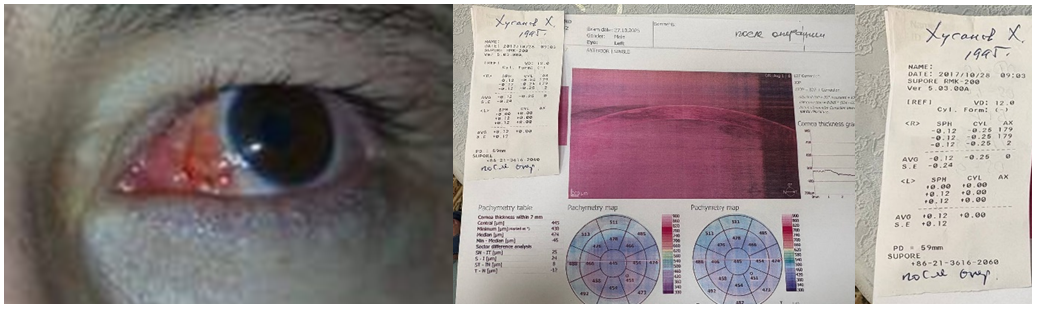 | Figure 2. A. The same patient after surgery. B. Refraction shows emmetropia; visual acuity 1.0 |
 | Table 2. Visual Functions Before and After Xenoplasty |
4. Conclusions
- In the advanced stages of pterygium, deep penetration into the corneal layers leads to destructive changes, and the growth of fibrovascular tissue significantly disrupts the sphericity of the cornea, which in turn induces astigmatism. Astigmatism is most often hypermetropic or mixed in nature. This is explained by traction exerted by fibrovascular tissue from the epithelium to the deeper layers of Bowman’s membrane.As the pterygium progresses, astigmatism intensifies, further reducing visual acuity. Specifically, in grade II pterygium, hypermetropic astigmatism averaged ±0.5 D; in grade III, it was ±1.5 D; and in grades IV–V, it reached ±3.0 D. In the postoperative period, astigmatism was eliminated in all studied groups. Visual acuity, which had decreased to between ±0.08 and ±0.8 before surgery, improved to between ±0.8 and ±1.0 after surgery. The visual field on the nasal side, which was narrowed by approximately 10–20° in grade III and IV–V pterygium, returned to normal limits postoperatively.