-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2006-2009
doi:10.5923/j.ajmms.20261604.90
Received: Mar. 11, 2026; Accepted: Apr. 6, 2026; Published: Apr. 25, 2026

Pathomorphological Alterations of the Gallbladder Wall in Chronic Calculous Cholecystitis Among Patients with Varying Degrees of Obesity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLR. M. Zaripova, M. A. Mamatalieva
Andijan State Medical Institute, Uzbekistan
Correspondence to: R. M. Zaripova, Andijan State Medical Institute, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The study aimed to investigate the pathomorphological and histochemical changes in chronic calculous cholecystitis in patients with varying degrees of obesity. The study was based on archival materials from the clinic of Andijan State Medical Institute collected between 2020 and 2024, including a total of 70 cases. The patients were distributed by age as follows: 18-44 years (20 cases), 45-59 years (25 cases), 60-74 years (15 cases), and 75-90 years (10 cases). Analysis of gallbladder structural alterations according to the degree of obesity demonstrated distinct morphological differences. In patients with grade I obesity, moderate inflammatory infiltration and initial signs of fibrosis were observed. In grade II obesity, pronounced fibrosis of the submucosal and muscular layers, epithelial atrophy of the mucosa, vascular dilation, stasis, and microthrombosis were identified. In grade III obesity, severe fibrosis and sclerosis of all layers of the gallbladder wall, marked wall deformation, pronounced epithelial atrophy, significant macrophage and lymphocytic infiltration, and muscular layer atrophy were observed. Obesity of varying severity leads to impairment of compensatory-adaptive mechanisms of the gallbladder, resulting in chronic inflammation, progressive atrophy, sclerosis, and decreased contractile function of the gallbladder wall, accompanied by increasing fibrotic-sclerotic and metabolic changes.
Keywords: Chronic cholecystitis, Obesity, Lymphoid infiltration, Fibrosis, PAS reaction
Cite this paper: R. M. Zaripova, M. A. Mamatalieva, Pathomorphological Alterations of the Gallbladder Wall in Chronic Calculous Cholecystitis Among Patients with Varying Degrees of Obesity, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2006-2009. doi: 10.5923/j.ajmms.20261604.90.
1. Introduction
- In recent decades, obesity has been recognized as one of the most significant medical and social problems worldwide. According to epidemiological studies, the prevalence of obesity continues to increase in many countries and is accompanied by a growing incidence of hepatobiliary diseases, including chronic calculous cholecystitis [1,2]. Obesity is associated with disturbances in lipid metabolism, increased cholesterol secretion into bile, and impaired motor function of the gallbladder, which contributes to the formation of gallstones and the development of inflammatory processes [3]. Gallstone disease is one of the most common disorders of the digestive system. Epidemiological data indicate that gallstones are detected in approximately 10–15% of the adult population in developed countries [4]. It is estimated that up to 20% of individuals may develop gallstones during their lifetime, and a considerable proportion of these patients eventually develop symptomatic disease or related complications [5].Numerous studies have confirmed that obesity is one of the major risk factors for gallstone formation. Metabolic syndrome, insulin resistance, and hypercholesterolemia contribute to increased bile lithogenicity and impaired gallbladder motility [6]. These processes create favorable conditions for chronic inflammation and structural remodeling of the gallbladder wall [7]. It has been demonstrated that the prevalence of gallstone disease is significantly higher in patients with severe obesity. In individuals with morbid obesity, signs of gallstone disease are observed in at least 25% of cases [8]. Furthermore, obesity increases the risk of complications of biliary pathology, including acute cholecystitis, cholangitis, and biliary pancreatitis [9].Several studies have shown that an increasing degree of obesity is associated with more pronounced morphological changes in the gallbladder wall. These changes include thickening of the gallbladder wall, development of fibrotic processes, atrophy of the mucosal epithelium, and disturbances in microcirculation [10]. Such alterations lead to decreased contractile function of the gallbladder and progression of chronic inflammatory processes [11].Epidemiological data also indicate that gallstone disease and chronic cholecystitis occur more frequently in women, particularly during the reproductive period. This is associated with hormonal factors that influence cholesterol metabolism and increase the lithogenicity of bile [12]. During pregnancy, hormonal changes may lead to decreased gallbladder motility and bile stasis, which further contributes to gallstone formation [13]. Despite the considerable number of studies devoted to the clinical aspects of chronic calculous cholecystitis, the morphological and histochemical changes of the gallbladder wall in patients with different degrees of obesity remain insufficiently studied. Clarification of these alterations is important for a deeper understanding of the disease pathogenesis and for improving diagnostic and therapeutic approaches [14].Purpose of the StudyTo characterize the pathomorphological and histochemical changes in chronic calculous cholecystitis among patients with varying degrees of obesity, and to assess the relationship between obesity severity and the extent of gallbladder wall alterations.
2. Materials and Methods
- The study material consisted of archival surgical and biopsy specimens collected from the clinic of Andijan State Medical Institute (AGMI) during the period 2020–2024, as well as the corresponding medical records of the patients. In total, 70 cases were included, distributed across age groups as follows: 20 patients aged 18-44 years, 25 patients aged 45-59 years, 15 patients aged 60-74 years, and 10 patients aged 75-90 years.For comparative purposes, control material was obtained from archival gallbladder specimens held by the Pathology Bureau of Andijan Region, collected from individuals who had no known gallbladder pathology and had died from causes unrelated to hepatobiliary disease. A total of five control cases were analyzed.The archival biopsy specimens were processed using standard histological techniques. Sections were stained with hematoxylin and eosin to assess general tissue architecture, Sudan III for lipid detection, periodic acid-Schiff (PAS) reaction for glycoconjugates, and Van Gieson stain for connective tissue evaluation. This comprehensive histochemical approach allowed for detailed assessment of pathomorphological and metabolic alterations in the gallbladder wall associated with varying degrees of obesity.
3. Results and Discussion
- The highest proportion of patients was observed in the age groups 45-59 years (36%) and 18-44 years (29%), while the lowest proportion was in the 75-90 years age group (14%). The male-to-female ratio was approximately 1:4. Regarding obesity severity, 57% of patients presented with grade I obesity, 27% with grade II obesity, and 16% with grade III obesity.Morphologically, chronic inflammation of the gallbladder mucosa was characterized by dense infiltration of lymphocytes and macrophages, segmented neutrophils, and eosinophils. The mucosal layer exhibited thickening, increased density, formation of Luschka’s ducts, focal atrophy, and the development of polypoid protrusions. In the muscular layer, hypertrophy, fibrotic changes, and thickening due to edema were observed.Macroscopically, the gallbladder walls were enlarged, tense, and congested, with engorged and deformed veins. The serosal surface appeared dull and uneven, the wall itself was thickened, and the mucosa showed scarring. Gallstones of various numbers, sizes, and morphological types were present, often causing mechanical compression of the mucosa. This compression resulted in epithelial injury, inflammatory responses, and impairment of the lymphatic and vascular networks. Consequently, microcirculatory disturbances, tissue edema, disruption of the fibro-architectural organization, and structural deformation were observed, leading to destructive degenerative changes in the gallbladder wall.These findings indicate a clear correlation between obesity severity and the extent of morphological alterations, highlighting the impact of metabolic and mechanical stressors on gallbladder pathology. The observed changes in both the mucosal and muscular layers suggest that chronic calculous cholecystitis in obese patients involves a combination of inflammatory, fibrotic, and degenerative processes, which may compromise gallbladder function and contribute to disease progression (see Figure 1).
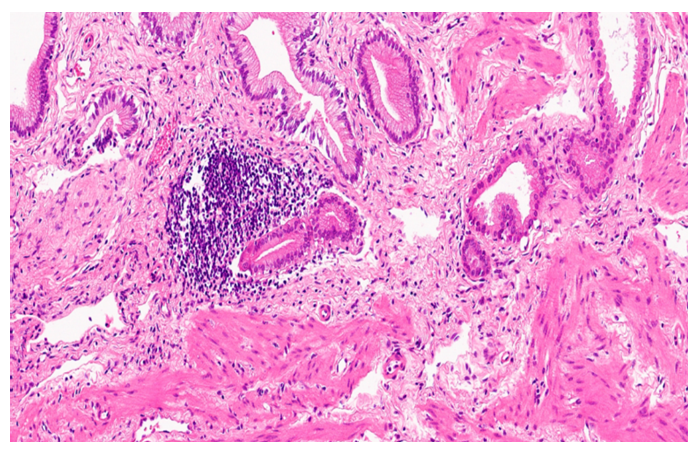 | Figure 1. A 34-year-old female patient with chronic calculous cholecystitis and grade I obesity. The mucosal and submucosal layers show focal and diffuse lymphoid infiltration, with a small number of leukocytes and eosinophils. The submucosal layer is thickened, Luschka’s ducts are present, and there are areas of focal atrophy and polypoid proliferations. Sclerotic changes were observed in the muscular layer. Hematoxylin and Еosin staining; magnification ×10 |
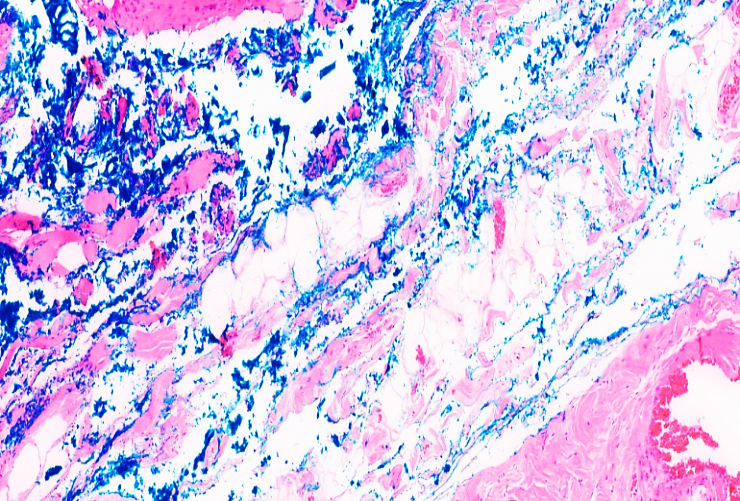 | Figure 2. A 45-year-old female patient with grade II obesity and chronic cholecystitis. The mucosal layer shows atrophy, and the glands exhibit atrophy with myxomatous changes. Diffuse proliferation of adipose tissue is present in the submucosal layer, accompanied by edema, sclerotic alterations, and diffuse lymphoid infiltration. The vessel walls demonstrate congestion and hyalinosis. Periodic acid-Schiff (PAS) reaction; magnification ×4/10 |
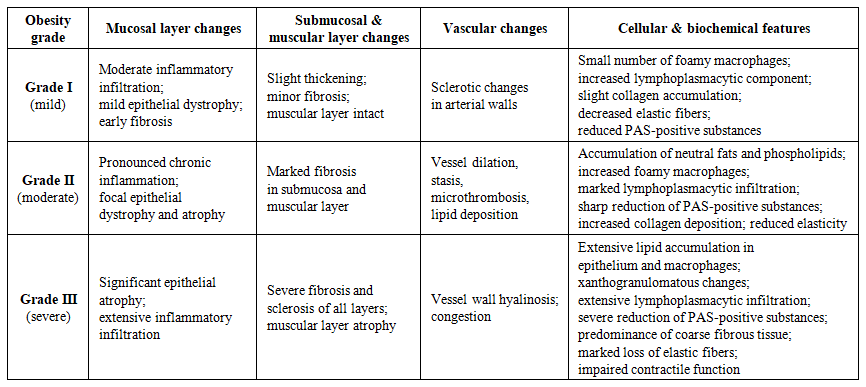 | Table 1. Summarizes the main morphological and histochemical features of the gallbladder wall according to obesity severity |
4. Conclusions
- Obesity of varying degrees profoundly affects the compensatory and adaptive mechanisms of the gallbladder. This impairment manifests as chronicization of inflammatory processes, progressive atrophy, and sclerosis of the gallbladder wall, leading to a significant reduction in its contractile function. The structural compromise is accompanied by an increase in fibrotic and sclerotic remodeling, as well as metabolic alterations within the gallbladder wall, including collagen accumulation, loss of elastic fibers, and lipid infiltration of both the epithelium and macrophages.These changes not only reduce the organ’s functional capacity but also exacerbate the pathological progression of chronic calculous cholecystitis in obese patients. The severity of these alterations is closely correlated with the degree of obesity, highlighting the importance of early diagnosis and management of obesity to prevent advanced gallbladder pathology.Understanding these pathomorphological and histochemical changes provides crucial insights into the mechanisms underlying gallbladder dysfunction and can guide the development of more targeted therapeutic strategies. In clinical practice, monitoring and mitigating obesity-related metabolic and inflammatory processes may help preserve gallbladder structure and function, thereby reducing the risk of severe complications such as biliary obstruction, xanthogranulomatous transformation, and impaired bile excretion.