-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2000-2005
doi:10.5923/j.ajmms.20261604.89
Received: Mar. 11, 2026; Accepted: Apr. 10, 2026; Published: Apr. 25, 2026

Clinical and Immunological Characteristics of Broncho-Obstructive Syndrome in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNormatov Dilmurod Khasanovich, Fayzieva Ugilbibi Ruzibadalovna
Department " Propaedeutics of Children's Diseases, Children's Diseases and Pediatrics in Family Medicine", Termez Branch of Tashkent State Medical University, Surkhandarya region, Termez, I. Karimov Street 65, Uzbekistan
Correspondence to: Normatov Dilmurod Khasanovich, Department " Propaedeutics of Children's Diseases, Children's Diseases and Pediatrics in Family Medicine", Termez Branch of Tashkent State Medical University, Surkhandarya region, Termez, I. Karimov Street 65, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article describes modern immunological diagnostics for broncho-obstructive syndrome in children. The key to improving the diagnosis and differential diagnosis of broncho-obstructive syndrome in children is the timely identification of sick children with complicated disease courses. According to the author, the levels of cytokine genes IL-5, IL-13, TNF-α, IFN-γ, IL-18, and Th /Th2 in the serum of children with broncho-obstructive diseases depend on the prevalence and duration of the disease, as well as the duration of obstructive attacks.
Keywords: Children, Cytokines, IL-5, IL-13, TNF-α, IFN-γ, IL-18, Immune response, Th1/Th2
Cite this paper: Normatov Dilmurod Khasanovich, Fayzieva Ugilbibi Ruzibadalovna, Clinical and Immunological Characteristics of Broncho-Obstructive Syndrome in Children, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2000-2005. doi: 10.5923/j.ajmms.20261604.89.
Article Outline
1. Introduction
- Respiratory diseases are a leading cause of childhood morbidity and are the primary and/or competing cause of mortality in children in the first years of life. In the Russian Federation, respiratory diseases are the third leading cause of infant mortality. Respiratory diseases in children associated with bronchial obstruction syndrome are among the most common, and their importance is steadily increasing due to the constant increase in the number of patients with acute obstructive bronchitis, recurrent obstructive bronchitis, and bronchial asthma. Broncho-obstructive syndrome (BOS) is a pathophysiological concept characterized by impaired bronchial patency in patients with acute and chronic diseases. It is widespread BOS in children determines the importance of timely identification of significant differential diagnostic signs, as well as establishing the relationship between risk factors and the characteristics of the course of bronchial obstruction in infants. Common clinical signs of bronchial obstruction include tachypnea, expiratory dyspnea with the involvement of accessory muscles, noisy wheezing (in English-language literature, this symptom complex is called wheezing), chest distension, and a wet or paroxysmal, spasmodic cough. With severe bronchial obstruction, cyanosis and other symptoms of respiratory failure may be present. Auscultation reveals Scattered moist fine bubbling rales, dry wheezing, and crepitation in bronchiolitis; percussion sounds are box-like, narrowing the boundaries of cardiac dullness. Chest X-ray reveals pulmonary distension [1,2,6,10].One of the most difficult and controversial issues in pediatric practice is the diagnosis of bronchial asthma (BA) based on the first episodes of bronchial obstruction (BO), especially in infants, young children, and preschoolers (Balabolkin I.I., Baranov A.A., Astafieva N.G., Wright A.L.). It is during these age periods that the anatomical and physiological characteristics of the respiratory organs and the systems that regulate their function remain important, and a high incidence of respiratory infections with broncho-obstructive syndrome (BOS) is observed (Smolenov I.V., Volkov I.K., Gore C.).The main etiologic factors of acute respiratory distress syndrome (AOS)/ bronchiolitis are respiratory viruses, most commonly the respiratory syncytial virus (RSV). The onset of the disease is acute, with catarrhal symptoms, and body temperature is normal or subfebrile. Clinical signs of AOS may appear on the first day or 2–4 days after the onset of the disease. Infants, especially premature infants, may experience apnea, typically early in the disease, before respiratory symptoms manifest [3,4,5,7].Cytokines are currently considered protein-peptide molecules produced by various cells of the body and mediating intercellular and intersystemic interactions. Cytokines (CK) are hormone-like molecules whose action on the target cell is mediated by highly specific high-affinity membrane receptors. Cytokines are universal regulators of the cell life cycle; they control the processes of differentiation, proliferation, functional activation, and apoptosis of the latter. Currently, there are several different classifications of cytokines, taking into account their structure, functional activity, origin, and the type of cytokine receptors [6,8,9,11].The immune system of young and preschool-aged children is characterized by functional immaturity, manifested by reduced production of certain cytokines, insufficient activation of T-helper type 1 (Th1) cells, and a predominance of the Th2 response. This creates the preconditions for the development of airway gyperreactivity and chronic inflammation. Cytokines play a key role in regulating inflammatory processes and the immune response during respiratory infections. However, their precise role in the pathogenesis of BOS in children of different age groups remains a subject of scientific debate (Golshah). et al., 2024).Of particular concern is the high incidence of broncho-obstructive syndrome (BOS) in children, manifesting as bronchiolitis, acute and recurrent obstructive bronchitis, and asthmatic conditions. BOS not only impairs a child's quality of life but can also lead to long-term consequences, including the development of chronic lung diseases in adulthood. Despite significant research, the pathogenic mechanisms underlying the development of BOS in children remain poorly understood, particularly in the context of immunological changes occurring in early life.Recent studies highlight the importance of studying immunological markers to understand the mechanisms of BOS development. For example, it has been established that levels of certain cytokines can correlate with disease severity and prognosis. However, most existing data are based on studies of adult patients or older children, which limits their applicability to younger age groups (Golshah et al., 2024).The limitations of the research include heterogeneity of the groups, different approaches and time points, and unclear terminology. In the Russian literature, we were able to find only a few studies devoted to the study of diseases associated with broncho-obstructive syndromes, such as acute bronchiolitis, obstructive bronchitis, and recurrent bronchitis. This information convinces us of the need for further research in this area. Thus, the relevance of this study is due to the need for an in-depth study of the clinical and immunological mechanisms of the development of diseases occurring with broncho-obstructive syndrome in children.The aim of the study is to evaluate the concentrations of the cytokine profile in diseases accompanied by broncho-obstructive syndromes in children.
2. Study Material and Method
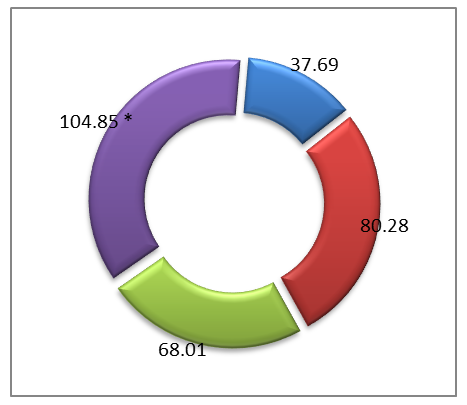
- The study included 58 children aged 4 to 6 years with clinically confirmed forms of BOS, including acute and recurrent obstructive bronchitis (AOB and ROB), as well as bronchiolitis. Diagnosis was established based on history, physical examination, and standard clinical criteria. The control group consisted of apparently healthy children of the same age (n=18). Immunological studies were conducted in the Immunoregulation laboratory at the Institute of Human Immunology and Genomics of the Academy of Sciences of the Republic of Uzbekistan. Peripheral blood serum served as the material for the study. Determination of serum cytokine levels (TNF-α, IFN-γ, IL-18, IL-5, IL-13). Serum concentration cytokines (TNF-α, IFN-γ, IL-18, IL-5, IL-13) were determined by the method of solid-phase enzyme-linked immunosorbent assay using the test systems of JSC "Vector - Best " (Russia) and " Cloud - Clone" Corp » (China) in accordance with the manufacturer's recommendations.Cytokines were determined by the enzyme-linked immunosorbent assay method using the Vector-Best (Russia) and Cloud - Clone test systems. Corp » (China).To determine the cytokine content in the blood of the study groups, a three-stage “sandwich” method was used – this is a variant of a three-phase enzyme immunoassay using monoclonal antibodies to a specific cytokine.BOS were examined in this study. The sample was selected based on age-specific stages of immune system development, in accordance with the concept of critical periods of immune ontogenesis proposed by J.B. Solomon (1978). For this purpose, patients were divided into two age categories: 0 to 3 years (n=54), allowing for consideration of the influence of age factors on the nature of the immune response.Statistical processing of the obtained data was performed using the computer program " Statistica 6.0". The data were statistically processed using standard approaches, the results are presented as the sample mean (M) and standard error of the mean (m); the median (Me), characterizing the central tendency, and the upper and lower quartiles characterizing the spread of the indicator values in 50% of respondents (Q1-Q3), where Q1 is the 25% percentile, Me is the 50% percentile, Q3 is the 75% percentile. The reliability of differences in the mean values (p) of the compared indicators was assessed using the Student's criterion (t).Within each age group, children with diseases associated with broncho-obstruction were further stratified by the clinical form of the disease. The following subgroups were identified: those with acute obstructive bronchitis (AOB), recurrent obstructive bronchitis (ROB), and bronchiolitis (B), which enabled a differentiated analysis of immunological parameters.To ensure the validity of the comparative analysis, a control group was formed, including clinically healthy children with no signs of acute or chronic diseases. Taking into account age-related characteristics, the control sample also included children aged 0 to 3 years (n=15), allowing for the interpretation of the obtained results in light of age-appropriate values for immunological parameters.An analysis of the immunological study results revealed that serum levels of the cytokines studied (TNF-α, IFN-γ, IL-18, IL-13, and IL-5) did not differ significantly between the age groups 0 to 3 years, indicating similarities in the immunological mechanisms that develop during the second and third critical periods. Therefore, to increase the representativeness of the study, it was decided to combine patients in this age group into a single group. Further analysis stratified them by clinical forms of the disease—AOB, ROB, and bronchiolitis —allowing for a more objective assessment of the specific immune profile depending on the course of broncho-obstructive syndrome.
|
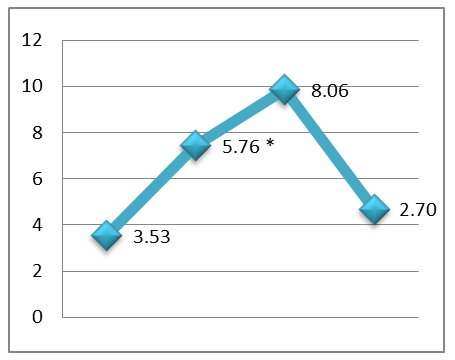
 | Figure 1. Serum concentration of TNF-α in the examined young children. Note:* - significant compared to the control group data p<0.05 -0.001) |
 | Figure 2. Serum IFN-γ levels in the examined young children. Note:*- significant compared to control group data (p<0.05 -0.001).^ -not significant compared to control group data (p>0.05) |
 | Figure 3. Serum IL-18 levels in the examined young children. Note: * - significant compared to the control group data ( p <0.05 -0.001) |
 | Figure 4. Serum IL-13 level in the examined young children. Note:* - reliable compared with the data of the control group (p<0.05 -0.001) |
 | Figure 5. Serum IL-5 levels in the examined young children. Note:* - significant compared to the control group data ( p <0.05 -0.001) |
3. Study Results and Discussion
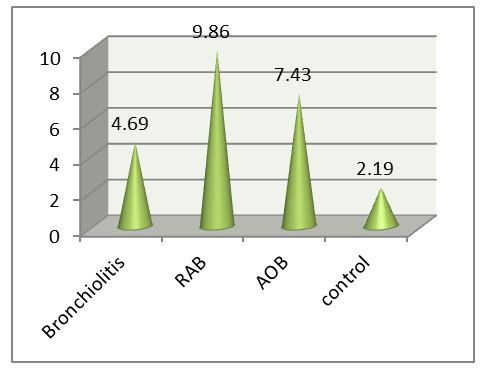
- An analysis of the cytokine profile in children aged 0–3 years with various forms of BOS revealed a clear relationship between the clinical course of the disease and the nature of the inflammatory response. Heterogeneity in immunopathogenesis, reflected in varying activation of proinflammatory mediators, was established.Bronchiolitis is characterized by marked activation of the innate immune system, with a sharp increase in TNF-α and IL-18 against a background of low IFN-γ, indicating neutrophil -macrophage inflammation and functional immaturity of the Th1 response. In acute obstructive pulmonary disease (AOB), combined activation of TNF-α, IFN-γ, IL-5, and IL-13 is observed, indicating the involvement of both the innate and adaptive immune systems. ROB is characterized by a dominant Th2 response with maximum levels of IL-5 and IL-13, as well as moderate activation of TNF-α and IFN-γ, reflecting the chronicity of eosinophilic inflammation.Thus, clinical forms of BOS in young children are realized through various immune mechanisms, which emphasizes the need to take them into account when developing pathogenetically based approaches to therapy. Thus, at present, a number of problems and issues related to improving the system of organizing the diagnosis and treatment of diseases with broncho-obstructive syndromes in young children, which determines the choice of topic for this scientific study and its relevance. Finally, it can be concluded that, in order to develop a scientifically sound set of measures to reduce the health losses of the child population from bronchopulmonary pathologies and their complications, it is necessary to study the immunological aspects of the disease.The study revealed that the immunological profile in children with BOS varies depending on age and the clinical form of the disease, reflecting age-related developmental characteristics of the immune system and the type of inflammatory response. Based on stratification by age-related critical periods of immune ontogenesis, significant differences in the serum levels of key proteins were identified. proinflammatory and Th2-associated cytokines.In children aged 0 to 3 years, a relative immaturity of the adaptive immune system and a predominance of the innate inflammatory response were revealed. In bronchiolitis and acute obstructive pulmonary disease in this age group, pronounced activation of TNF-α and IL-18 was observed, with weak expression of IFN-γ and limited involvement of Th2 cytokines, indicating a macrophage - neutrophil nature of the inflammation. At the same time, in In young children with ROB, an increase in IL-5 and IL-13 is recorded, reflecting the gradual formation of Th2-associated immune reactivity.Thus, clinical forms of BOS in young and preschool-aged children are characterized by differentiated immunopathogenetic mechanisms determined by the age stage of immune maturation and the type of cytokine imbalance. The identified changes in the levels of TNF-α, IL-18, IFN-γ, IL-5, and IL-13 suggest that they can be considered pathogenetic markers with diagnostic and prognostic value, as well as targets for immunomodulatory therapy.
4. Conclusions
- 1. Bronchiolitis is characterized by hyperactivation of the innate immune system, as evidenced by a maximum increase in TNF-α and IL-18 in the absence of a significant increase in IFN-γ and IL-13, indicating macrophage-neutrophil inflammation and Th1 regulation deficiency.2. Acute obstructive bronchitis is accompanied by a balanced activation of the Th1/Th2 response, in which the levels of TNF-α, IL-18, IFN-γ simultaneously increase, and IL-5 and IL-13 also moderately increase, reflecting the involvement of both innate and adaptive components of the immune defense.3. Recurrent Obstructive bronchitis demonstrates the dominance of the Th2 immune response, with a maximum increase in IL-5 and IL-13 against the background of a decrease in IFN-γ, which indicates chronic inflammation, eosinophilic infiltration and the formation of the Th2-dominant bronchial gyperreactivity phenotype.