-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1983-1988
doi:10.5923/j.ajmms.20261604.86
Received: Apr. 3, 2026; Accepted: Apr. 20, 2026; Published: Apr. 23, 2026

Results from Analysis of Effectiveness of Modified TAPP Hernioplasty in Inguinal Hernia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLObidov Sh. Kh., Mamarajabov S. E.
Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Obidov Sh. Kh., Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Inguinal hernia is one of the most prevalent ones in abdominal surgery, characterized by a high level of clinical and socioeconomic impact on pain, poor quality of life, and the risk of complications. The purpose of the study was to assess the relative effectiveness of modified transabdominal preperitoneal (TAPP) hernioplasty compared to the conventional TAPP and open Lichtenstein repair. An observational study was planned between 2022 and 2025, and comprised 252 patients with inguinal hernia, including three groups of patients with traditional TAPP (n=72), modified TAPP (n=70), and Lichtenstein repair (n=110). The baseline demographic and clinical variables, such as age, sex, body mass index, hernia size and type based on the EHS classification, were found to be similar across groups and therefore validity of the comparative analysis. The findings showed that modified TAPP technique exhibited a significant improvement in intraoperative performance as compared to traditional TAPP method, with a short operative time (69.8 vs 78.6 min), less intraoperative blood loss (9 vs 14 ml), and less peritoneal closure time. The Lichtenstein method was the least invasive in terms of operative time (58.7±14.8 min), yet, had much more blood loss (47 [28-74] ml), indicating more invasiveness. Intraoperative complications, such as peritoneal injury and conversion rates did not vary significantly. To sum up, the modified TAPP method is an enhanced form of the TAPP technique, which is more efficient and minimally invasive without compromising patient safety in comparison to other well-established methods.
Keywords: Inguinal hernia, TAPP, Modified TAPP, Lichtenstein repair, Intraoperative outcomes
Cite this paper: Obidov Sh. Kh., Mamarajabov S. E., Results from Analysis of Effectiveness of Modified TAPP Hernioplasty in Inguinal Hernia, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1983-1988. doi: 10.5923/j.ajmms.20261604.86.
1. Introduction
- Inguinal hernia is a type of surgery of the anterior abdominal wall, where the contents of the abdomen are pushed through the inguinal canal by the weakening of the anatomic structures of the abdominal wall congenitally or acquired [1,2]. It is a very common condition and it poses a serious clinical and socio-economic problem as well as pain, discomfort, diminished physical activity, impaired quality of life and the threat of imprisonment or even being strangled [3,4]. An inguinal hernia never goes away on its own and evolves to start as a small reducible bulge, which gradually grows to a symptomatic size and finally needs an operation to repair it [5,6].Clinically, an inguinal hernia is defined by a specific group of symptoms, including the development of an inguinal bulge, pain or discomfort, the feeling of heavy, and the exacerbation of symptoms during physical activities, coughing, and straining. Sometimes, the pain can extend to the scrotum or thigh [7,8]. Difficult types of hernia can be accompanied with acute pain, irreducibility, intestinal obstruction or ischaemia, which necessitates immediate surgery [9]. Therefore, earlier surgical intervention is deemed better than wait-and-see intervention.Instead, the standard evaluation of inguinal hernias is often performed according to the European Hernia Society (EHS) classification as it permits the assessment of the type of anatomy, location and size of the defect [10,11]. According to this classification inguinal hernias may be classified into lateral (indirect), medial (direct) and mixed hernias, each of which is different in anatomy, clinical implication, and surgical planning implications [11,12]. The lateral hernias run through the deep inguinal ring and are usually oblique, but medial hernias occur because of the weakness of the transverse fascia and are, therefore, able to enter through the posterior wall of the inguinal canal. The combination of the two mechanisms (pantalon hernias) means that the tissue weakness is more severe [12,13]. Moreover, the magnitude of the defect, according to the classification of the EOG, is of utility importance, as it determines the surgical procedure, mesh fixation plan and the probability of recurrence [14].The special focus is on modified TAPP techniques that have been designed to optimize intraoperative practices, decrease the length of the surgery, decrease the time to close the abdominal cavity, decrease blood loss, and enhance long-term and postoperative results [11-13]. The perceived benefits of the modified TAPP procedure could be linked to the ability to better dissect the tissues, better fixation of the mesh, less manipulation in the inguinal area, and less likely to injure the nerve [15]. Therefore, a comparative evaluation of standard and modified TAPP techniques and their comparison with the Lichtenstein technique are of great clinical interest.Accordingly, inguinal hernia could still be regarded as a burning problem of contemporary abdominal surgery, and the rationalisation of the methods is still a significant topic of study [16]. Evaluating the comparative effectiveness of modified TAPP hernioplasty in patients with inguinal hernias, one can not only determine its position among current surgical methods but also recognize some possible benefits in terms of postoperative pain reduction, decreased recovery period, a lower rate of complications, less risk of chronic pain and higher patient satisfaction rates [17-20]. The issue of which method proves to be more efficient i.e. modified TAPP or the traditional TAPP and the Lichtenstein technique, is a research question that is valid and important to the clinical sphere.
2. Materials and Methods
- This potential observational clinical trial was to compare the efficacy of various surgical techniques in the management of inguinal hernia, both traditional and modified transabdominal preperitoneal (TAPP) hernioplasty, open tension-free hernioplasty as per Lichtenstein. The researchers carried out the study on the surgical departments of Samarkand State Medical University clinic in Samarkand during the period 2022-2025. The participants in the study were 252 patients who had a clinically confirmed diagnosis of inguinal hernia. The patients were separated into three clinical groups, depending on the surgical method applied. The main group consisted of 70 patients who underwent modified TAPP hernioplasty. The first group of comparison consisted of 72 patients who had been operated under the traditional TAPP technique and the second group of comparison consisted of 110 patients who had undergone open Lichtenstein hernioplasty. All of the patients were dynamically followed. All the patients were subjected to regular clinical examinations to determine the degree of pain syndrome, the character of clinical manifestations, the size and type of hernial defect, and the functional condition of the patient. Inclusion criteria: Confirmed diagnosis of inguinal hernia; Age over 18 years; Principal or recurrent inguinal hernia; Signs of elective surgical treatment; Written consent to take part in the study. Exclusion criteria: Incarcerated inguinal hernia; Severe decompensated comorbidities; Coagulation disorders; Malignant neoplasms; Failure to comply with an examination procedure; Declined to take part in the study. Instrumental research methods. In clinical examination, the inguinal area was examined by inspecting and palpating it with evaluation of the size of the hernial protrusion, its reducibility, the availability of cough impulse, and whether it was unilateral or bilateral. To standardize the assessment of hernias, the European Hernia Society (EHS) classification was used. Ultrasound of the inguinal areas was carried out as required to explain the size of the hernial defect, the appearance of the hernial contents and the appearance of the surrounding tissues. The accuracy of diagnosis improved with the application of this method particularly in clinical cases that were doubtful. Patients were evaluated in terms of functional status through the use of standardized scales. The visual analog scale (VAS) was used to measure pain intensity. The parameters used intraoperative parameters were the length of surgery, the amount of blood loss, the rate of intraoperative complications, and the characteristics of mesh implant fixation. Such technical aspects of the intervention as the way of mesh fixation and the details of the work with the peritoneum during laparoscopic hernioplasty were analyzed independently. Laboratory research methods. Lab tests were done to objectively determine the somatic condition of patients and preoperative risk. Samples were taken in the morning on an empty stomach (812 hours of fasting) in 57 ml venous blood with the consideration of the standard preanalytical conditions. Complete blood count was done using an automatic hematology analyzer and included the level of hemoglobin (130160 g/L in men and 120140 g/L in women), leukocytes (4.090x109/L), and platelets (150400x109/L). Biochemical blood analysis was performed on an automatic analyzer and measured glucose (3.95mmol/L), creatinine (62106mmol/L), urea (2.583mmol/L), total protein (6585g/L), bilirubin (521mmol/L) and ALT, AST (<40U/L). In addition, prothrombin time (11-15 s), INR (0.8-1.2), and APTT (25-35 s) were determined in all patients. Statistical analysis. Variation statistics was used to evaluate the obtained results. The method of moments was used to obtain the arithmetic mean and the standard error. The Shapiro-Wilk test was used to check the hypothesis of normal distribution of the random variable. Student t -test was used to compare the quantitative variables that have normal distribution in two groups. For non-normally distributed data or ordinal variables, non-parametric tests such as ANOVA, Kruskal-Wallis, and Mann-Whitney U tests were used. All statistical calculations were carried out in R Studio version 4.3.2, Windows 10, with a significance level of p<0.05. The R packages that were used were epiDisplay, qwraps2, tidyverse, rstatix, ggpubr, and ggplot2. The 95% confidence intervals were used to present the results.
3. Results
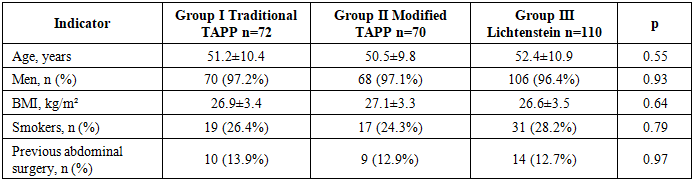
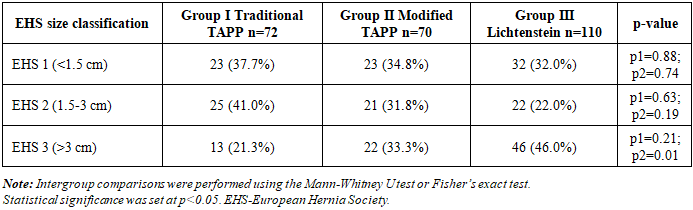
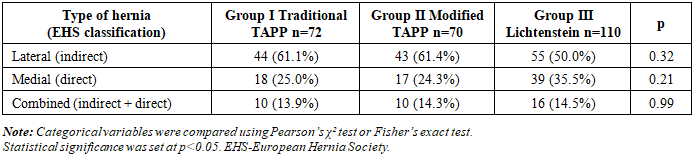
- The comparative demographic characteristics of patients across the study groups are presented in Table 1. The analysis demonstrated no statistically significant differences between the groups, confirming their homogeneity and supporting the validity of subsequent comparative evaluation of surgical outcomes.
|
|
|
|
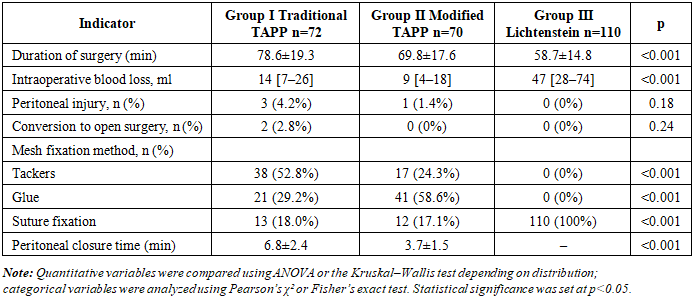
4. Conclusions
- The comparison of the study groups was based on similar baseline demographic and clinical features, which provided methodological validity of the outcomes comparison. Compared to the conventional TAPP, the modified TAPP technique exhibited a better intraoperative performance, with decreased operation time, reduced blood losses, and superior peritoneal closure. The Lichtenstein technique had the shortest length of operation, however, it was also accompanied by a much higher level of blood loss which means it was more invasive. The safety profiles of all surgical methods were similar, and there was no significant difference in the intraoperative complications.