-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1979-1982
doi:10.5923/j.ajmms.20261604.85
Received: Apr. 2, 2026; Accepted: Apr. 21, 2026; Published: Apr. 23, 2026

Analysis of Effectiveness of Therapeutic Approaches in the Treatment of Recurrent Malignant Gliomas of the Brain
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKarimova Nargiza Sunnatillayevna1, Nishanov Daniyar Anarbayevich2, Mamadaliyeva Yashnar Mamasaliyevna3
1Oncology, Medical Radiology, Tashkent State Medical University, Uzbekistan, Republican Specialized Scientific-Practical Medical Center of Oncology and Radiology of the Republic of Uzbekistan
2Pathomorphology, Republican Specialized Scientific-Practical Medical Center of Oncology and Radiology of the Republic of Uzbekistan
3Medical Radiology, Center for the Development of Professional Qualification of Medical Workers, Uzbekistan
Correspondence to: Karimova Nargiza Sunnatillayevna, Oncology, Medical Radiology, Tashkent State Medical University, Uzbekistan, Republican Specialized Scientific-Practical Medical Center of Oncology and Radiology of the Republic of Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

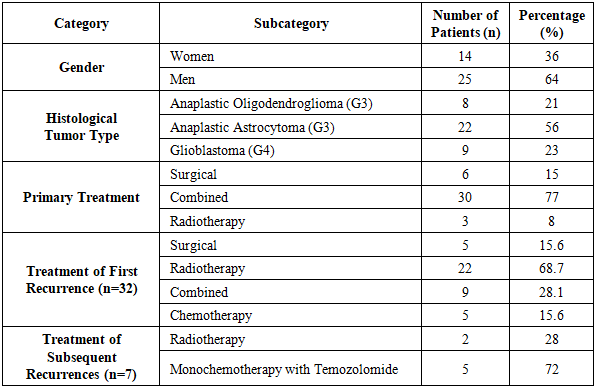
Objective: The aim of this study was to evaluate the overall survival (OS) of patients with recurrent malignant gliomas of the brain (MGGB) based on prognostic factors and treatment modalities. Materials and Methods: The treatment outcomes of 39 patients diagnosed with recurrent grade III-IV gliomas (G3-G4) were analyzed. These patients were admitted to the Republican Specialized Scientific-Practical Medical Center of Oncology and Radiology of the Republic of Uzbekistan (RSSPMCOandR) between 2018 and 2021. The mean age of the patients was 47±4.7 years, with a male-to-female ratio of 2:1. The average time to recurrence was 11.4 months. Among the patients, 32 had a single recurrence, while 7 experienced two consecutive recurrences. The treatment of high-grade glioma recurrences included repeat surgical resection in 5 patients, re-irradiation in various regimens in 22 patients, monochemotherapy with temozolomide in 5 patients, and combined therapy in 9 patients. Results: The OS of patients with recurrent malignant gliomas in the study was 27 months. The 1-year OS rate was 47.2%, and the 3-year OS rate was 27%. The median overall survival after recurrence treatment was 18 months. Age and gender did not significantly affect survival outcomes. The best OS outcomes for first-line recurrence treatment were observed in groups undergoing radiotherapy and reoperation, with a median OS of 18 months. In second-line recurrence treatment, the 1-year OS rate for patients receiving chemotherapy was 38%, compared to 31% for those undergoing re-irradiation (p=0.372). Conclusion: The OS of patients with recurrent malignant gliomas was 26.5 months, with a 1-year OS rate of 47.2%. No significant differences in survival outcomes were identified based on age or gender. Histological tumor type influenced prognosis: the median OS was 11 months for glioblastomas and 21 months for astrocytomas. Radiotherapy was identified as the most effective treatment for recurrence, achieving the highest survival outcomes.
Keywords: Glioma recurrence, Recurrence treatment method, Radiotherapy
Cite this paper: Karimova Nargiza Sunnatillayevna, Nishanov Daniyar Anarbayevich, Mamadaliyeva Yashnar Mamasaliyevna, Analysis of Effectiveness of Therapeutic Approaches in the Treatment of Recurrent Malignant Gliomas of the Brain, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1979-1982. doi: 10.5923/j.ajmms.20261604.85.
1. Introduction
- Malignant glial tumors of the brain are among the most aggressive primary neuroepithelial neoplasms, characterized by high mortality rates and frequent local and distant recurrences [7]. These tumors exhibit diffuse infiltrative growth, which complicates complete surgical resection and contributes to their high recurrence rates [1, 8]. Glioblastoma is the most aggressive type of glioma, representing nearly 49% of all malignant brain tumors diagnosed in adults (JAMA, 2023) [2]. The classification of glial tumors is based on their histological structure and degree of malignancy. According to the classification of the World Health Organization (WHO), gliomas are categorized into four grades (I–IV). Tumors classified as grades I–II are considered low-grade malignancies, whereas those in grades III–IV exhibit high-grade malignancy characteristics. High-grade gliomas, such as anaplastic astrocytoma (grade III) and glioblastoma (grade IV), are distinguished by rapid growth and a high propensity for recurrence [1,6].Prognostic factors for recurrence include patient age, tumor localization, and molecular-genetic characteristics. Younger age and superficial tumor localization are associated with a more favorable prognosis [7]. Mutations in the IDH1/2 genes, MGMT promoter methylation, and 1p/19q codeletion are critical molecular markers influencing prognosis and recurrence rates [7].Several molecular predictors are associated with the recurrence of malignant glial brain tumors. Mutations in the IDH gene have been linked to shorter time to recurrence [4,9]. Ransohoff [3] determined that surgical intervention for tumor recurrence does not significantly impact survival rates, particularly in patients experiencing further disease progression. These findings suggest that surgical management of recurrence should be considered only in cases of confirmed clinical progression. In such instances, reoperation contributes to a more precise morphological diagnosis by taking into account the tumor’s specific characteristics, thereby enabling a more accurate prediction of its future course [11].The role of chemotherapy in the treatment of recurrent malignant gliomas remains a subject of debate. Temozolomide is the standard chemotherapeutic agent for the treatment of recurrent high-grade malignant gliomas (Grade III and IV). Studies have shown that different dosing regimens of temozolomide can affect its efficacy and tolerability. A meta-analysis including 33 studies with 1,760 participants demonstrated that the 7-day on/7-day off regimen outperforms the standard schedule in terms of 6-month progression-free survival (34.8%) and 12-month progression-free survival (15.5%) in patients with Grade IV gliomas [12].Van den Bent et al. [5] documented a 63% objective response rate, along with an enhancement in overall survival, among patients undergoing PCV therapy. Nonetheless, the clinical efficacy and safety of alternative chemotherapeutic agents, including nitrosoureas, hydroxyurea in combination with imatinib, irinotecan, and paclitaxel, in the context of recurrent gliomas, have not been extensively investigated, limiting their adoption in standard clinical practice [1,5].Objective: The aim of this study was to evaluate the overall survival (OS) of patients with recurrent malignant gliomas of the brain (MGGB) based on prognostic factors and treatment modalities.
2. Materials and Methods
- A retrospective analysis of medical records was conducted for 39 patients with confirmed recurrences of high-grade malignant gliomas (G3-G4) who underwent treatment at the RSSPMCOandR from 2018 to 2021. Morphological examination identified anaplastic oligodendroglioma (G3) in 8 patients, anaplastic astrocytoma (G3) in 22 patients, and glioblastoma (G4) in 9 patients (Table 1). The mean age of the patients was 47±4.7 years, with a male-to-female ratio of 2:1.
|
3. Results
- The OS with recurrent MGGB was 26.5 months. The one-year OS rate was 47.2%, while the three-year OS rate was 27.0%. The median OS following recurrence treatment was 27 months.An analysis of OS considering age demonstrated that elderly patients have a less favorable prognosis due to challenges in administering intensive treatment, whereas younger patients tend to exhibit a more aggressive disease course. However, no statistically significant differences between age groups were identified (p=0.46). Similarly, OS analysis by gender did not reveal statistically significant differences (p=0.89), although women exhibited a slightly higher OS rate (27.0%) compared to men (18.8%).When OS was analyzed by histological tumor type, it was found that patients with glioblastomas had a poorer prognosis compared to those with astrocytomas, with median OS of 11 and 21 months, respectively, although the differences did not reach statistical significance (p=0.578).The analysis of survival based on the number of recurrences demonstrated a trend toward reduced survival rates in cases with two recurrences (Figure 1.). The impact of treatment modalities on OS showed that the best outcomes were achieved in groups receiving radiotherapy or reoperation, with median OS of 18 and 17 months, respectively (p=0.26) (Figure 2.).
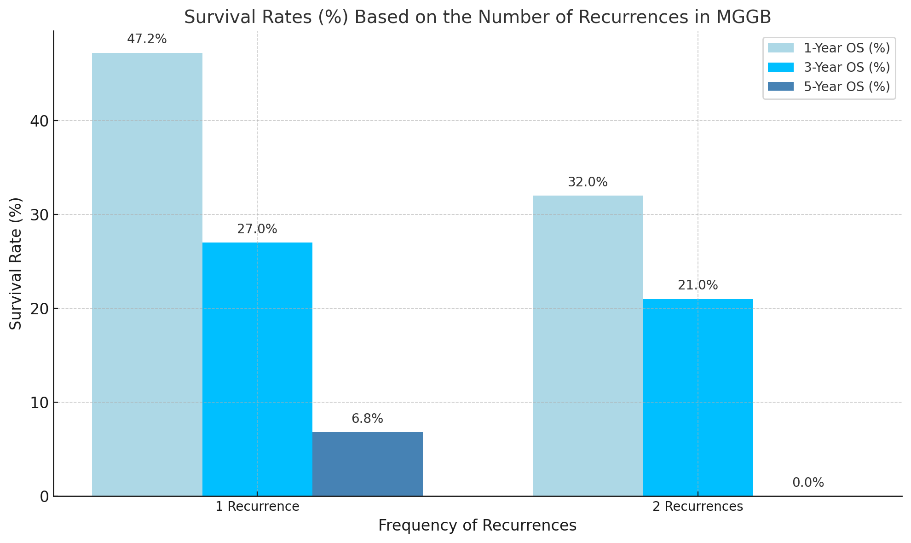 | Figure 1. Comparison of Survival Rates (%) Based on the Number of Recurrences in MGGB |
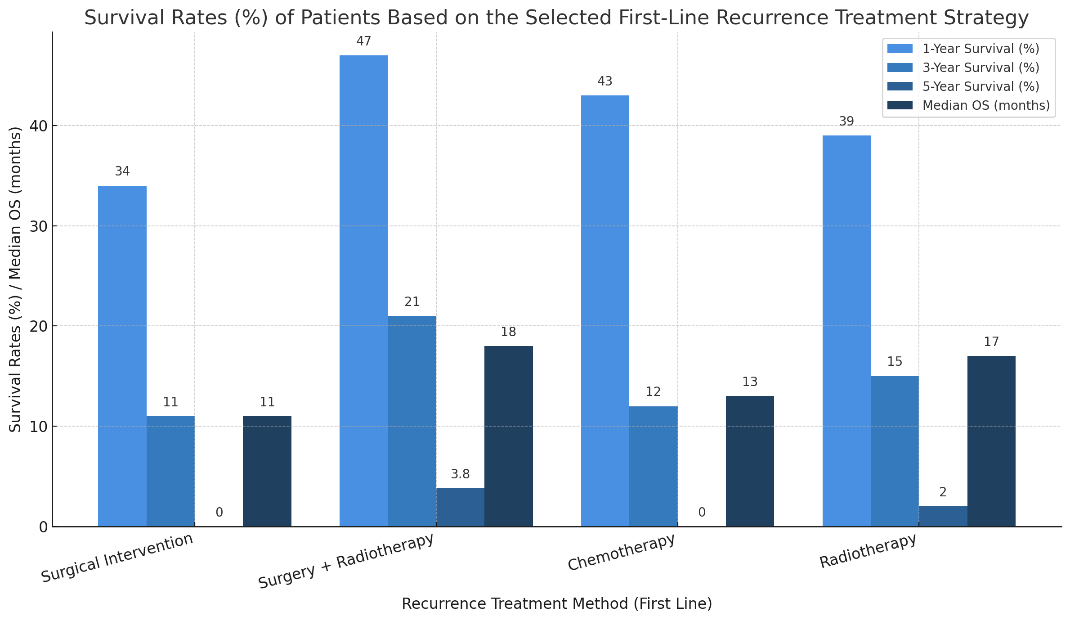 | Figure 2. Survival Rates (%) of Patients Based on the Selected First-Line Recurrence Treatment Strategy |
4. Conclusions
- The OS of patients with recurrent malignant gliomas of the brain was 26.5 months, with a 1-year OS rate of 47.2% and a 3-year OS rate of 27.0%. No statistically significant differences in survival outcomes were observed based on age or gender (p>0.05), although women demonstrated slightly higher 1-year OS rates compared to men. The histological tumor type had a notable impact on prognosis, with glioblastoma patients exhibiting worse survival outcomes than those with astrocytomas (median OS of 11 months and 21 months, respectively, p=0.578).The most effective treatment for recurrences was radiotherapy. At the same time, second-line chemotherapy demonstrated better one-year overall survival (OS) rates (38%) compared to repeat radiotherapy (31%). Despite the treatment efforts, neurological deterioration was observed in 11 patients, indicating tumor progression.