-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1973-1978
doi:10.5923/j.ajmms.20261604.84
Received: Mar. 22, 2026; Accepted: Apr. 15, 2026; Published: Apr. 23, 2026

Clinical and Immunological Efficacy of Stromal Vascular Fraction in Rheumatologic Patients with Avascular Necrosis of the Femoral Head
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKaxxarov A. S.1, Ibragimov Kh. I.1, Ziyadullayev Sh. Kh.2
1Samarkand State Medical University, Samarkand, Uzbekistan
2Kimyo University in Tashkent, Samarkand Branch, Samarkand, Uzbekistan
Correspondence to: Kaxxarov A. S., Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Avascular necrosis of the femoral head (AVNFH) is a progressive disorder frequently observed in patients with rheumatologic diseases and is associated with impaired microcirculation, inflammation, and bone remodeling disturbances. The present study aimed to evaluate clinical, imaging, functional, and immunological outcomes in patients with AVNFH and to assess the effectiveness of combined therapy including stromal vascular fraction (SVF) compared with standard treatment over a 12-month follow-up period. A total of 122 patients were included and divided into a main group receiving SVF-based therapy and a comparison group receiving standard treatment. Disease progression was assessed using ARCO staging, magnetic resonance imaging, pain scores, functional indices, quality of life parameters, and immunological markers. The results demonstrated significantly slower progression of AVNFH in the SVF group, with a higher proportion of patients remaining at early stages and a reduced transition to advanced stages. MRI findings showed a marked reduction in the necrotic lesion size. Patients receiving SVF therapy exhibited greater pain reduction, improved hip joint function, and significantly better quality of life outcomes. In addition, SVF therapy was associated with increased levels of CD4⁺ T cells and NK cells, along with a significant decrease in proinflammatory cytokines, including tumor necrosis factor alpha and interleukin 6. These findings suggest that SVF-based therapy provides clinically meaningful benefits by modulating inflammation, improving microcirculation, and enhancing tissue regeneration in patients with AVNFH.
Keywords: Avascular necrosis, Stromal vascular fraction, Rheumatology, Cytokines, Bone regeneration
Cite this paper: Kaxxarov A. S., Ibragimov Kh. I., Ziyadullayev Sh. Kh., Clinical and Immunological Efficacy of Stromal Vascular Fraction in Rheumatologic Patients with Avascular Necrosis of the Femoral Head, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1973-1978. doi: 10.5923/j.ajmms.20261604.84.
1. Introduction
- Avascular necrosis of the femoral head (AVNFH) is a progressive and disabling condition characterized by impaired microcirculation, ischemia of bone tissue, and subsequent structural collapse of the femoral head [1–3]. The disease is particularly relevant in patients with rheumatologic disorders, including systemic lupus erythematosus and rheumatoid arthritis, where chronic inflammation, endothelial dysfunction, and long-term glucocorticoid therapy contribute significantly to its development and progression [4,5]. Epidemiological studies demonstrate that the prevalence of AVNFH is notably higher in patients with autoimmune diseases, especially systemic lupus erythematosus, where both disease-related and treatment-related factors play a critical role [6–8].The pathogenesis of AVNFH is complex and involves vascular compromise, oxidative stress, and apoptosis of bone cells. Proinflammatory cytokines such as tumor necrosis factor alpha and interleukin 6 play a key role in stimulating osteoclast activity and disrupting bone remodeling processes [11,12]. In addition, glucocorticoids contribute to disease progression by inducing endothelial dysfunction, promoting adipogenesis in bone marrow, and impairing angiogenesis [4,11]. Hypercoagulable states, particularly in patients with antiphospholipid syndrome, further exacerbate microvascular occlusion and bone ischemia [10]. These mechanisms highlight the multifactorial nature of AVNFH and the importance of systemic factors in its progression [9].Despite advances in diagnostic imaging, including magnetic resonance imaging that allows early detection of ischemic changes, the management of AVNFH remains challenging. Conventional treatment strategies are primarily focused on symptom control and slowing disease progression; however, their ability to prevent structural deterioration and restore bone integrity remains limited [3]. In many cases, disease progression leads to advanced stages requiring surgical intervention such as total hip arthroplasty.In recent years, regenerative approaches have gained increasing attention. Stromal vascular fraction (SVF), derived from adipose tissue, contains mesenchymal stem cells, endothelial progenitor cells, and immunomodulatory components that may enhance angiogenesis, stimulate osteogenesis, and modulate inflammatory processes. These properties make SVF a promising therapeutic strategy targeting key mechanisms of AVNFH pathogenesis [5,9,12].In addition to structural damage, AVNFH significantly affects patient quality of life through chronic pain and functional impairment. Emerging evidence suggests that immunological markers, including proinflammatory cytokines and indicators of bone resorption, may serve as important tools for assessing disease activity and monitoring therapeutic response [3,7].However, comprehensive clinical and immunological evaluation of patients with AVNFH in the context of rheumatologic diseases remains insufficiently explored. In particular, the effects of regenerative therapies on disease progression, functional outcomes, immunological parameters, and bone remodeling markers require further investigation.Therefore, the aim of the present study was to assess clinical, imaging, functional, and immunological outcomes in patients with AVNFH associated with rheumatologic diseases and to evaluate the effectiveness of combined therapy including stromal vascular fraction compared with standard treatment over a 12-month follow-up period.
2. Materials and Methods
- This prospective observational study included rheumatologic patients diagnosed with avascular necrosis of the femoral head (AVNFH) who were hospitalized and received inpatient treatment between 2021 and 2025 at the Department of Rehabilitation, Medical Tourism, and Adult Orthopedics No. 3 of the Samarkand branch of the Republican Scientific and Practical Center of Traumatology and Orthopedics. A total of 122 patients were enrolled, including individuals with rheumatoid arthritis (n = 73) and systemic lupus erythematosus (n = 44), aged between 32 and 68 years. The mean age of the cohort was 41.5 ± 6.2 years, and the study population included 83 women (68.0%) and 39 men (32.0%). Patients were divided into two groups depending on the treatment received: a main group (n = 64) and a comparison group (n = 58). Additionally, a control group consisting of 100 age- and sex-matched healthy individuals was included for baseline comparison of clinical and laboratory parameters. The follow-up period lasted 12 months, with repeated assessments conducted every 3 months.Patients were eligible for inclusion if they were aged between 18 and 70 years, had a confirmed diagnosis of a rheumatologic disease in remission for at least 12 weeks, and were diagnosed with AVNFH stage I or II according to the ARCO classification. Patients with prior hip surgery, advanced stages of AVNFH (stage III–IV), severe comorbid conditions, active infections, malignancy, pregnancy, lactation, or contraindications to therapy were excluded from the study.The main group received combined therapy including stromal vascular fraction (SVF), while the comparison group received standard pharmacological treatment. SVF was obtained using a standardized protocol based on minimally invasive liposuction. Adipose tissue was harvested under local anesthesia from the abdominal region following antiseptic preparation. The aspirated material underwent centrifugation, filtration, and mechanical processing to isolate the cellular fraction. The final product was combined with autologous conditioned plasma, resulting in a total injectable volume of approximately 15 mL. The SVF preparation was administered intra-articularly into the affected hip joint under ultrasound or fluoroscopic guidance to ensure precise delivery to the necrotic area. Patients received one to three injections at 6-week intervals depending on clinical response.All patients received comprehensive therapy aimed at controlling the underlying rheumatologic disease and preventing progression of necrosis. Rheumatoid arthritis patients were treated with methotrexate at doses of 15–25 mg per week, with folic acid supplementation, and in selected cases with Janus kinase inhibitors or rituximab. Patients with systemic lupus erythematosus received immunosuppressive therapy including mycophenolate mofetil or azathioprine, with biologic agents such as belimumab or rituximab when indicated. Glucocorticoids were administered at the lowest effective dose, generally not exceeding 7.5 mg/day in prednisolone equivalents. Bisphosphonates, vitamin D, and calcium supplementation were prescribed to support bone metabolism. In patients with antiphospholipid antibodies, anticoagulation therapy was implemented according to clinical indications.Clinical and functional outcomes were assessed at baseline and at 3, 6, and 12 months using validated scales, including the Visual Analog Scale for pain, the Harris Hip Score, and the WOMAC index. Imaging evaluation was performed using magnetic resonance imaging as the primary modality for staging and monitoring disease progression according to ARCO criteria. Additional imaging methods, including radiography, computed tomography, and in selected cases SPECT/CT, were used to assess structural changes and perfusion.Laboratory assessment included measurement of inflammatory cytokines, coagulation parameters, lipid profile, and bone remodeling markers. Levels of tumor necrosis factor alpha, interleukin 6, and interleukin 1 beta were determined using enzyme-linked immunosorbent assay. Coagulation status was evaluated using prothrombin time, activated partial thromboplastin time, fibrinogen, and international normalized ratio. Lipid metabolism was assessed through measurement of total cholesterol, triglycerides, low-density lipoproteins, and high-density lipoproteins. Bone turnover markers, including procollagen type I N-terminal propeptide (P1NP) and C-terminal telopeptide (CTX), were measured using automated immunoassay systems.Statistical analysis was performed using R software version 4.3.2. Data distribution was assessed using the Shapiro–Wilk test. Continuous variables were expressed as mean ± standard deviation or median with interquartile range. Comparisons between groups were conducted using Student’s t-test or the Mann–Whitney U test as appropriate. Categorical variables were analyzed using the chi-square test. A p-value of less than 0.05 was considered statistically significant.
3. Results
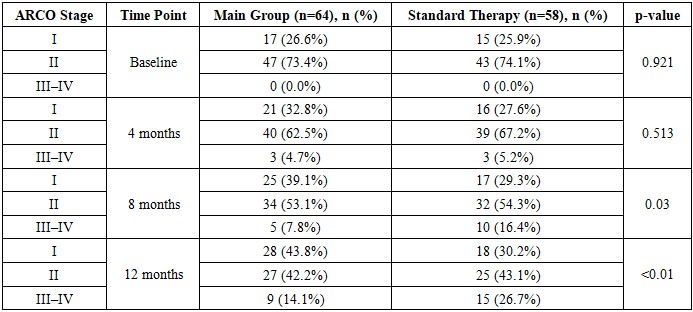
- At baseline, both groups were comparable in terms of disease stage distribution. In the main group, stage I was observed in 17 patients (26.6%) and stage II in 47 patients (73.4%), while in the comparison group stage I was present in 15 patients (25.9%) and stage II in 43 patients (74.1%), with no cases of stages III–IV in either group (p=0.921).At 4 months, a modest increase in stage I cases was observed in both groups (32.8% vs 27.6%), without statistically significant differences (p=0.513). However, by 8 months, a significant divergence emerged: stage I was observed in 39.1% of patients in the main group compared with 29.3% in the comparison group, while progression to stages III–IV occurred in 7.8% versus 16.4% of patients, respectively (p=0.03).By 12 months, these differences became more pronounced. In the main group, 43.8% of patients remained in stage I compared with 30.2% in the comparison group, while progression to advanced stages (III–IV) occurred in 14.1% versus 26.7%, respectively (p<0.01), indicating a significant slowing of disease progression with SVF therapy.
|
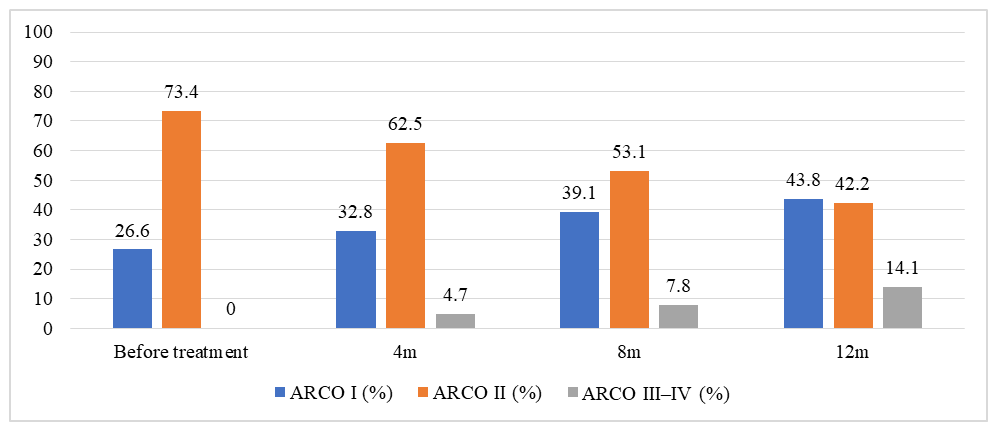 | Figure 1. Changes in ARCO stage distribution over 12 months in rheumatologic patients with avascular necrosis of the femoral head treated with SVF |
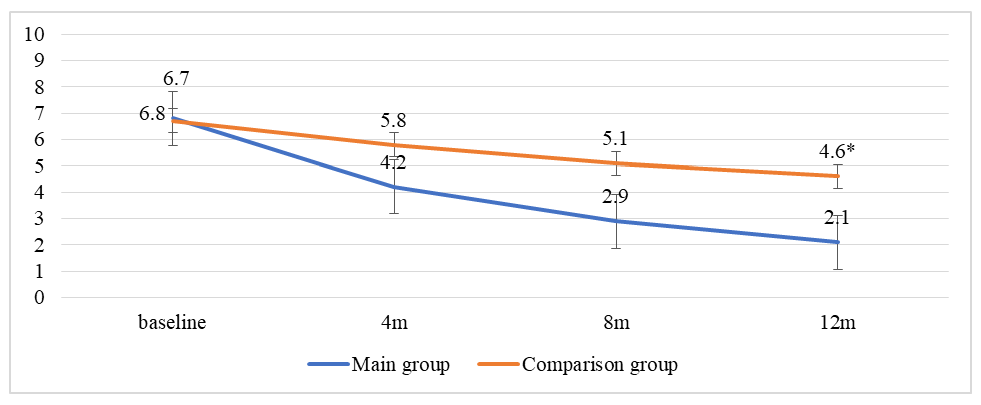 | Figure 2. Changes in VAS scale over 12 months in rheumatologic patients with avascular necrosis of the femoral head treated with SVF |
|

|
4. Discussion
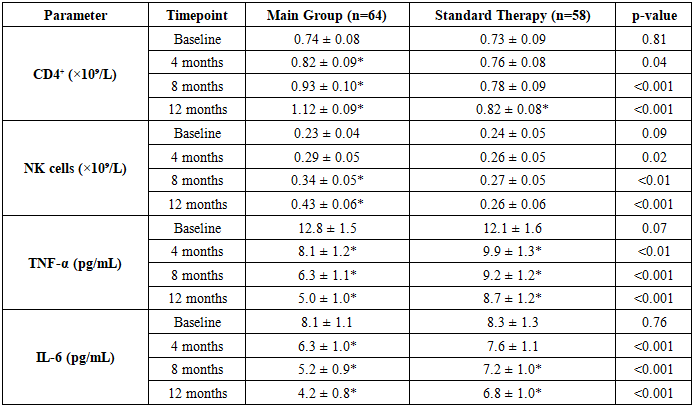
- The present study demonstrates that stromal vascular fraction (SVF)-based therapy provides clinically meaningful benefits in patients with avascular necrosis of the femoral head associated with rheumatologic diseases. These findings are consistent with current evidence indicating that AVNFH is a multifactorial condition driven by vascular impairment, chronic inflammation, immune dysregulation, and altered bone remodeling [1–3]. Targeting these mechanisms simultaneously appears to improve clinical and structural outcomes.In this study, patients receiving SVF therapy showed greater improvement in pain and functional status compared with those receiving standard treatment. These results are in line with previous reports suggesting that regenerative therapies can enhance tissue repair and reduce symptoms in early-stage AVNFH [3]. The observed clinical improvements may be explained by improved microcirculation, reduced intraosseous pressure, and modulation of inflammatory pathways.Imaging findings further support these observations. Patients in the SVF group demonstrated stabilization of disease at early stages and a lower rate of progression compared with the comparison group. This aligns with current understanding that preservation of blood supply and early intervention are critical for preventing femoral head collapse [2,3]. The reduction in necrotic lesion size and bone marrow edema suggests a regenerative effect mediated through enhanced angiogenesis.A key finding of the study is the modulation of immunological parameters. The decrease in proinflammatory cytokines, including tumor necrosis factor alpha and interleukin 6, confirms the central role of inflammatory mediators in disease progression [11,12]. These cytokines promote osteoclast activation and impair bone regeneration, and their reduction likely contributes to improved clinical outcomes. At the same time, the increase in CD4⁺ T cells and natural killer cells suggests activation of immune-regulatory mechanisms, supporting the immunomodulatory potential of SVF therapy.Changes in coagulation parameters further emphasize the importance of vascular mechanisms. The observed normalization of fibrinogen and D-dimer levels is consistent with previous studies demonstrating the role of hypercoagulability and microthrombosis in AVNFH pathogenesis, particularly in patients with autoimmune diseases and antiphospholipid syndrome [9,10]. Improvement in these parameters suggests enhanced microcirculation and reduced thrombotic risk.The analysis of bone remodeling markers revealed increased P1NP and decreased CTX levels in the SVF group, indicating a shift toward bone formation and reduced resorption. These findings support the concept that regenerative therapies can restore the balance of bone turnover, which is disrupted in osteonecrosis due to hypoxia and cellular apoptosis [2,5].The strengths of this study include its prospective design, comprehensive evaluation of clinical, imaging, immunological, and metabolic parameters, and inclusion of a comparison group. However, several limitations should be acknowledged. The study was conducted at a single center, and the follow-up period of 12 months may not fully reflect long-term outcomes. In addition, the absence of randomization may introduce potential bias.Overall, the results suggest that SVF-based therapy represents a promising and pathogenetically justified approach for the management of early-stage AVNFH in patients with rheumatologic diseases. By targeting inflammation, vascular dysfunction, and impaired bone remodeling, this therapy may delay disease progression and improve functional outcomes.
5. Conclusions
- Stromal vascular fraction–based therapy demonstrated significant clinical and structural advantages over standard treatment in patients with avascular necrosis of the femoral head of rheumatologic origin, as evidenced by a higher proportion of patients remaining in early ARCO stages and reduced progression to advanced stages over 12 months, along with a marked decrease in necrotic lesion size on MRI. Patients receiving SVF therapy experienced greater pain reduction and superior functional recovery, reflected by improved VAS and Harris Hip Score outcomes, as well as substantial improvements in quality of life parameters. These clinical benefits were accompanied by pronounced immunomodulatory effects, including increased CD4⁺ T-helper and NK cell levels and significant reductions in proinflammatory cytokines such as TNF-α and IL-6. Additionally, the strong positive correlation between NTX-I levels and lesion size highlights its potential role as a biomarker of disease severity.