Kaxxarov A. S.1, Ibragimov Kh. I.1, Ziyadullayev Sh. Kh.2
1Samarkand State Medical University, Samarkand, Uzbekistan
2Kimyo University in Tashkent, Samarkand Branch, Samarkand, Uzbekistan
Correspondence to: Kaxxarov A. S., Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Avascular necrosis of the femoral head (AVNFH) is a progressive and debilitating condition resulting from impaired blood supply to bone tissue, ultimately leading to structural collapse and joint dysfunction. The disease is particularly prevalent in patients with systemic rheumatic disorders such as systemic lupus erythematosus, rheumatoid arthritis, and antiphospholipid syndrome. Its development reflects a complex interplay between disease-related inflammation, vascular abnormalities, metabolic disturbances, and pharmacological factors, especially glucocorticoid therapy. Pathogenetically, AVNFH is driven by microcirculatory impairment involving arterial occlusion, venous stasis, microthrombosis, and endothelial dysfunction, which together result in ischemia and osteocyte death. At the molecular level, oxidative stress, apoptosis of osteoblasts and osteocytes, and impaired angiogenesis contribute to progressive bone destruction. Glucocorticoids further exacerbate these mechanisms by promoting adipogenesis, suppressing osteogenesis, and disrupting vascular integrity. Clinically, the disease often remains asymptomatic in early stages, delaying diagnosis until structural damage has occurred. Magnetic resonance imaging is the most sensitive modality for early detection, while laboratory biomarkers reflecting bone turnover, inflammation, and coagulation abnormalities are gaining importance in risk assessment and monitoring. Management strategies depend on disease stage and include conservative measures, pharmacological interventions aimed at reducing inflammation and improving microcirculation, and emerging regenerative approaches such as stromal vascular fraction therapy. Surgical options, including core decompression and total hip arthroplasty, are reserved for advanced stages. Given its increasing incidence and significant impact on young, active populations, early identification and personalized therapeutic strategies are essential to improve outcomes and preserve joint function.
Keywords:
Avascular necrosis, Femoral head, Rheumatic diseases, Glucocorticoids, Microcirculation
Cite this paper: Kaxxarov A. S., Ibragimov Kh. I., Ziyadullayev Sh. Kh., Pathogenesis and Management of Avascular Necrosis of the Femoral Head in Rheumatology, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1964-1972. doi: 10.5923/j.ajmms.20261604.83.
1. Introduction
Avascular necrosis of the femoral head represents a complex and multifactorial pathological condition that develops due to disruption of the intraosseous microcirculation and subsequent ischemia of bone tissue. This process leads to osteocyte apoptosis, structural weakening of trabecular bone, and progressive collapse of the femoral head. Ultimately, the disease results in secondary osteoarthritis and irreversible loss of joint function [1,2].The condition occurs frequently in patients with systemic rheumatic diseases such as systemic lupus erythematosus, rheumatoid arthritis, antiphospholipid syndrome, and systemic vasculitides. These disorders promote chronic systemic inflammation, endothelial dysfunction, and hypercoagulability, which directly impair vascular supply to the femoral head [8,9]. In addition, therapeutic interventions, particularly long-term glucocorticoid use, significantly increase the risk of osteonecrosis through multiple metabolic and vascular mechanisms [4,5].At the cellular level, ischemia initiates a cascade of pathological events that includes oxidative stress, mitochondrial dysfunction, and activation of apoptotic pathways in osteocytes and osteoblasts. These processes reduce bone regeneration and accelerate structural deterioration [15,16]. Simultaneously, impaired angiogenesis limits the capacity for vascular repair, which further perpetuates ischemic damage and necrosis [18].Clinically, avascular necrosis demonstrates a heterogeneous course. Early stages often remain asymptomatic despite ongoing structural damage. As the disease progresses, patients develop pain localized to the groin or thigh, reduced range of motion, and functional limitations. Advanced stages involve subchondral fractures and collapse of the femoral head, which require surgical intervention [3].The clinical importance of this condition has increased in recent years due to its growing incidence in younger and economically active populations. The disease leads to long-term disability, reduced quality of life, and increased need for total hip arthroplasty. Therefore, clinicians must recognize avascular necrosis as a major complication of rheumatic diseases and implement early diagnostic and preventive strategies [3].Epidemiology and Clinical SignificanceThe epidemiology of avascular necrosis of the femoral head demonstrates a substantial and persistent burden in patients with rheumatic diseases. Meta-analytical evidence indicates that the prevalence of osteonecrosis in systemic lupus erythematosus reaches approximately 14.6 percent, particularly among patients exposed to high cumulative doses of glucocorticoids [6]. Large population-based studies confirm these findings and report prevalence rates of approximately 8 to 10 percent [7].The disease frequently affects both hips. Bilateral involvement occurs in up to 50 percent of cases, which reflects the systemic nature of the underlying pathophysiological mechanisms [8]. In addition, multifocal osteonecrosis involving multiple joints has been increasingly reported, especially in patients with autoimmune diseases and prolonged immunosuppressive therapy (table 1) [12].Table 1. Epidemiology and Risk Factors of AVNFH in Rheumatologic Diseases
 |
| |
|
Recent epidemiological trends demonstrate a significant increase in the number of total hip arthroplasty procedures performed for avascular necrosis. This increase is particularly evident in patients younger than 45 years. Such findings indicate earlier disease onset and more aggressive progression compared with degenerative joint diseases [13,14]. Furthermore, patients with systemic autoimmune conditions often experience less favorable postoperative outcomes, including delayed rehabilitation and higher complication rates [14].Advances in diagnostic imaging have contributed to a rise in reported incidence. Magnetic resonance imaging allows detection of early ischemic changes before structural damage becomes visible on radiographs. Studies report that MRI achieves high sensitivity and specificity in early-stage disease, which facilitates timely diagnosis and intervention [23,24].At the same time, modern treatment strategies for rheumatic diseases have influenced disease patterns. Prolonged use of glucocorticoids and immunosuppressive agents increases survival in these patients but also elevates the cumulative risk of osteonecrosis. This paradox highlights the need to balance therapeutic benefits with long-term complications [11].Importantly, recent studies emphasize the high prevalence of asymptomatic forms of avascular necrosis. Many patients demonstrate early ischemic lesions on MRI without clinical symptoms. These subclinical forms often progress to symptomatic disease if left untreated, which underscores the importance of proactive screening in high-risk populations [12].The socioeconomic impact of avascular necrosis remains considerable. The disease affects individuals during their most productive years and leads to loss of work capacity, long-term disability, and increased healthcare costs. Surgical management, particularly total hip arthroplasty, imposes additional economic burden on healthcare systems [3].Taken together, these data indicate that avascular necrosis of the femoral head represents not only a clinical problem but also a significant public health issue. Early identification of high-risk patients and implementation of preventive strategies remain essential to reduce disease burden and improve patient outcomes.
2. Etiology and Risk Factors
Avascular necrosis of the femoral head develops through a complex interaction of pharmacological, immunological, vascular, metabolic, and demographic factors. Current evidence supports a multifactorial model in which several mechanisms act simultaneously and amplify the risk of bone ischemia and structural damage [1,3].Glucocorticoids represent the most consistently identified and clinically significant risk factor for avascular necrosis. Numerous studies demonstrate a strong dose dependent relationship between glucocorticoid exposure and disease development [4,5].A cumulative dose of prednisolone exceeding 10 g markedly increases the probability of osteonecrosis. Initial doses greater than 30 mg per day also correlate with a higher incidence of early disease onset [6]. Even short courses of high dose therapy can trigger pathological changes in susceptible individuals.Glucocorticoids impair bone and vascular homeostasis through several mechanisms. They induce apoptosis of osteocytes and osteoblasts, suppress angiogenesis, and promote adipogenesis within bone marrow. These changes increase intraosseous pressure and reduce perfusion, which accelerates ischemic injury [19,20]. In addition, glucocorticoids disrupt endothelial function and contribute to hypercoagulability, which further compromises microcirculation [4].Systemic rheumatic diseases contribute independently to the development of avascular necrosis. Chronic inflammation plays a central role in this process. Conditions such as systemic lupus erythematosus, rheumatoid arthritis, and dermatomyositis promote persistent immune activation and vascular injury [9].Proinflammatory cytokines including tumor necrosis factor alpha and interleukin 6 stimulate osteoclast activity and inhibit osteoblast function. These effects disrupt bone remodeling and favor resorption over formation [17]. At the same time, inflammatory mediators induce endothelial dysfunction, which reduces nitric oxide availability and impairs vascular tone regulation.Autoimmune diseases also promote microvascular damage and capillary rarefaction. These changes limit oxygen delivery to bone tissue and increase susceptibility to ischemia even in the absence of high dose glucocorticoid exposure [9].Thrombotic mechanisms play a crucial role in the pathogenesis of avascular necrosis, particularly in patients with antiphospholipid syndrome. This condition induces a hypercoagulable state that leads to microthrombosis within the intraosseous vasculature [10].Antiphospholipid antibodies, including anticardiolipin and beta2 glycoprotein I antibodies, directly damage endothelial cells and activate coagulation pathways. These processes promote fibrin deposition and vascular occlusion. As a result, blood flow to the femoral head becomes compromised, which initiates ischemic necrosis [10].In addition, subclinical coagulation abnormalities have been observed in patients without overt antiphospholipid syndrome. These findings suggest that thrombophilia represents a broader contributor to disease development [10].Metabolic abnormalities significantly increase the risk of avascular necrosis by affecting vascular integrity and bone metabolism. Hyperlipidemia promotes lipid deposition within blood vessels and bone marrow, which leads to fat embolism and reduced microvascular perfusion [11].Hypertension contributes to vascular stiffness and endothelial dysfunction, which impair blood flow regulation. Metabolic syndrome, characterized by obesity, insulin resistance, dyslipidemia, and hypertension, has been identified in up to 67 percent of patients with non traumatic osteonecrosis in certain populations [11].These metabolic disturbances also enhance oxidative stress and inflammation, which further damage vascular and bone tissues. Demographic characteristics influence both susceptibility and disease progression. Avascular necrosis occurs more frequently in women aged 20 to 45 years, particularly in association with autoimmune diseases [9]. However, studies indicate that men often experience a more aggressive disease course with faster progression and higher rates of bilateral involvement [8].Ethnic and geographic variations also affect disease prevalence. Differences in genetic predisposition, environmental factors, and treatment practices contribute to these variations across populations [11].In summary, avascular necrosis of the femoral head represents a multidimensional pathological syndrome driven by interacting risk factors. Pharmacological exposure, systemic inflammation, vascular dysfunction, coagulation abnormalities, and metabolic disturbances act synergistically to impair bone perfusion and initiate necrosis. Recognition of these factors is essential for early risk stratification and implementation of preventive strategies.
3. Pathogenesis
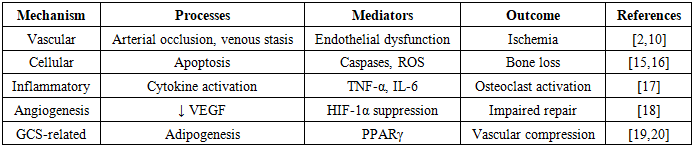
The pathogenesis of avascular necrosis of the femoral head involves a cascade of interrelated vascular, cellular, and molecular events that ultimately result in bone ischemia, structural collapse, and joint dysfunction. Current evidence supports a unified pathophysiological model in which vascular compromise acts as the initiating event, while subsequent cellular, biochemical, and inflammatory mechanisms drive disease progression and determine the extent of tissue damage [2,3].Impaired blood supply represents the central initiating mechanism in avascular necrosis. The femoral head possesses a unique vascular anatomy characterized by terminal branches and limited collateral circulation, which makes it highly vulnerable to ischemic injury. Even a moderate reduction in perfusion can disrupt oxygen delivery, alter cellular metabolism, and initiate irreversible damage to bone tissue [2].Several key vascular processes contribute to this impairment. Arterial occlusion reduces inflow to the subchondral bone and leads to acute or chronic ischemia. Venous stasis increases intraosseous pressure, which compresses arterial vessels and further decreases perfusion. This mechanism creates a compartment-like effect within the femoral head, intensifies hypoxia, and accelerates tissue injury (table 2) [18].Table 2. Mechanistic Overview of pathogenesis of AVNFH
 |
| |
|
Microthrombosis plays a critical role in obstructing small vessels within the femoral head. Thrombotic occlusion reduces capillary flow and promotes the formation of localized ischemic zones. Endothelial dysfunction further aggravates this process by impairing nitric oxide mediated vasodilation, increasing vascular resistance, and promoting a prothrombotic state [10].Experimental and clinical data indicate that a reduction in blood flow of approximately 30 to 40 percent is sufficient to initiate osteonecrosis. Sustained hypoperfusion leads to osteocyte death, disruption of bone matrix integrity, and activation of downstream degenerative mechanisms [2].Following vascular compromise, cellular and molecular alterations drive the progression of bone damage. Osteocytes and osteoblasts undergo apoptosis in response to hypoxia, nutrient deprivation, and metabolic stress. This loss of viable bone cells disrupts the dynamic balance between bone formation and resorption and leads to progressive weakening of trabecular architecture [15].Oxidative stress plays a central role in this process. Increased production of reactive oxygen species damages cellular membranes, proteins, and nucleic acids. Mitochondrial dysfunction further amplifies oxidative injury by impairing ATP production and promoting the release of pro apoptotic factors, which accelerates programmed cell death [16].Activation of caspase dependent pathways represents a key mechanism of apoptosis. Increased expression of apoptotic markers has been observed in steroid induced osteonecrosis and correlates with disease severity and extent of necrotic lesions [15].Inflammatory cytokines contribute significantly to disease progression. Tumor necrosis factor alpha and interleukin 6 stimulate osteoclast differentiation and activity, enhance bone resorption, and simultaneously inhibit osteoblast mediated regeneration. These processes create an imbalance in bone remodeling and lead to progressive structural deterioration [17].Impaired angiogenesis represents another critical component of pathogenesis. Physiological bone repair requires adequate formation of new blood vessels to restore perfusion and support regeneration of necrotic tissue. In avascular necrosis, this reparative process becomes markedly disrupted.Reduced expression of vascular endothelial growth factor and hypoxia inducible factor 1 alpha limits neovascularization within the affected region. This deficiency prevents restoration of microcirculation and prolongs the ischemic microenvironment [18].The persistence of hypoxia leads to continued cellular injury, inhibition of osteogenesis, and progressive expansion of the necrotic area. This mechanism establishes a vicious cycle in which inadequate perfusion promotes further ischemia, cellular death, and structural collapse. The inability to restore microvascular integrity represents a major barrier to spontaneous recovery and contributes to disease progression.Glucocorticoids play a central role in the pathogenesis of avascular necrosis, particularly in patients with rheumatic diseases. These agents induce multiple pathological alterations that affect both bone cells and vascular structures and significantly amplify disease risk [4,5].Glucocorticoids shift the differentiation of mesenchymal stem cells from osteogenesis toward adipogenesis through activation of the PPAR gamma signaling pathway. This shift increases fat accumulation within bone marrow, elevates intraosseous pressure, and compresses microvascular structures, which reduces perfusion [19].In addition, glucocorticoids suppress the expression of vascular endothelial growth factor, which impairs angiogenesis and limits formation of new blood vessels. They also increase apoptosis of osteocytes and osteoblasts, which weakens bone architecture and reduces regenerative capacity [20].Glucocorticoids further contribute to endothelial dysfunction and promote a hypercoagulable state, which enhances microthrombus formation and exacerbates vascular compromise [4].These combined effects create a self perpetuating cycle of ischemia and degeneration. Reduced blood flow leads to cellular death, which further compromises bone integrity and vascular function. This mechanism explains the progressive nature of the disease and highlights the importance of early therapeutic intervention.
4. Clinical Presentation and Classification
Avascular necrosis of the femoral head demonstrates a variable clinical course that depends on the stage of disease, the extent of structural involvement, and the rate of progression. In early stages, patients often remain asymptomatic despite ongoing ischemic and cellular damage within the bone. This silent progression delays diagnosis and reduces the opportunity for early intervention, particularly in high risk populations such as patients receiving glucocorticoid therapy [3].As the disease advances, patients develop characteristic symptoms. Pain typically localizes in the groin region and may extend to the anterior thigh or radiate to the knee due to shared innervation pathways. Mechanical loading exacerbates pain, and patients frequently report discomfort during weight bearing activities, prolonged standing, or walking. Progressive limitation of hip joint mobility develops, particularly affecting internal rotation and abduction, which are often the earliest movements to be impaired [1,21].Pain in avascular necrosis has both mechanical and inflammatory components. Early pain often appears intermittently and relates to microfractures within the subchondral bone. With disease progression, pain becomes more persistent and may occur at rest, reflecting increased intraosseous pressure and synovial involvement (table 3).Table 3. Clinical Staging Systems Comparison
 |
| |
|
In later stages, structural collapse of the femoral head leads to severe joint dysfunction. Patients experience persistent pain at rest, marked restriction of movement, and significant impairment in daily activities such as walking, sitting, and climbing stairs. These changes often result in substantial disability, reduced quality of life, and eventual loss of functional independence.Importantly, clinical symptoms do not always correlate with the degree of structural damage. Some patients with advanced radiological changes report minimal symptoms, while others develop significant pain in earlier stages. This discrepancy reflects differences in lesion size, location, rate of progression, and individual pain perception. It also highlights the limitations of clinical examination alone and underscores the importance of imaging in disease evaluation [21].In addition, bilateral involvement is common and may remain asymptomatic on one side. Therefore, clinicians should maintain a high index of suspicion and consider imaging of both hips in patients at risk [8].Several classification systems have been developed to standardize staging of avascular necrosis and guide clinical decision making. These systems aim to correlate structural changes with clinical severity and to facilitate selection of appropriate treatment strategies. Among these, the most widely used systems include Ficat and Arlet, Steinberg, and ARCO classifications [21,22].The Ficat and Arlet classification represents one of the earliest and most widely applied systems. It relies primarily on radiographic findings and clinical features. The system categorizes disease progression from stage I, where radiographs appear normal but symptoms may be present, to stage IV, which includes femoral head collapse and secondary osteoarthritis. Despite its simplicity, this system has limitations in detecting early disease because it does not incorporate advanced imaging techniques [21].The Steinberg classification expands upon the Ficat system by incorporating quantitative assessment of lesion size. It subdivides each stage based on the percentage of femoral head involvement, which provides important prognostic information. Larger lesions associate with higher risk of collapse and poorer clinical outcomes. This classification improves risk stratification and supports more individualized treatment planning [22].The ARCO classification represents a more comprehensive and modern approach. It integrates findings from radiography, computed tomography, and magnetic resonance imaging. This system allows precise evaluation of lesion size, location, and structural integrity. It also improves reproducibility and interobserver reliability, which makes it particularly useful in both clinical practice and research settings [22].In addition to staging, lesion location plays a critical role in prognosis. Lesions located in the weight bearing zone of the femoral head demonstrate a higher risk of collapse compared with medial or non weight bearing regions. This factor is particularly emphasized in ARCO and Steinberg classifications.These classification systems have direct clinical relevance. Early stages allow the use of joint preserving strategies such as pharmacological therapy, load modification, and core decompression. In contrast, advanced stages with structural collapse typically require surgical intervention, most commonly total hip arthroplasty [26].Accurate staging also guides prognosis. Patients diagnosed at early stages have significantly better outcomes and higher rates of joint preservation. Conversely, delayed diagnosis often results in irreversible structural damage and limited therapeutic options.Overall, integration of clinical assessment with imaging based classification systems remains essential for optimal management of avascular necrosis of the femoral head.
5. Diagnostic Approaches
Imaging plays a central role in the diagnosis of avascular necrosis, particularly in early stages when clinical findings remain nonspecific and physical examination lacks sensitivity. Early detection relies almost entirely on imaging modalities that can identify ischemic changes before irreversible structural damage occurs.Magnetic resonance imaging represents the gold standard diagnostic modality. It provides high sensitivity, ranging from approximately 96 to 99 percent, and allows detection of early ischemic changes before radiographic abnormalities become apparent. MRI identifies bone marrow edema, subchondral lesions, and early necrotic zones with high accuracy [23,24].Characteristic MRI findings include the “double line sign” on T2 weighted images, which reflects the interface between necrotic and viable bone. Bone marrow edema patterns often correlate with pain severity and may indicate active disease progression. MRI also enables precise assessment of lesion size, location, and extent, which are critical parameters for prognosis and treatment planning.Computed tomography provides detailed visualization of bone structure and is particularly useful for assessing subchondral fractures, femoral head collapse, and architectural distortion in advanced stages. It also supports preoperative planning by allowing accurate evaluation of cortical integrity and lesion geometry [3].Conventional radiography remains widely available but has limited sensitivity in early disease. Radiographic changes such as sclerosis, cyst formation, and crescent sign typically appear only after substantial structural damage has occurred. Therefore, radiographs are more useful for staging rather than early diagnosis.Table 4. Comparative Imaging Modalities in AVNFH and corresponding characteristics
 |
| |
|
Scintigraphy and single photon emission computed tomography allow evaluation of functional bone metabolism and regional blood flow. These techniques can detect early perfusion abnormalities and may assist in identifying multifocal disease. Hybrid SPECT CT improves anatomical localization and diagnostic accuracy compared with conventional scintigraphy [25].Each imaging modality provides complementary information. MRI detects early disease, CT evaluates structural damage, and nuclear imaging assesses functional perfusion. Integration of these techniques enhances diagnostic accuracy and improves clinical decision making.Biomarkers are gaining increasing attention as tools for early detection, risk stratification, and monitoring of avascular necrosis. Although imaging remains the cornerstone of diagnosis, laboratory markers provide valuable insight into underlying pathophysiological processes and may help identify high risk patients before radiological changes occur.Markers of bone turnover reflect imbalance in bone remodeling. Increased levels of C terminal telopeptide indicate enhanced osteoclastic activity and bone resorption, while decreased levels of procollagen type I N terminal propeptide suggest reduced osteoblastic bone formation. This imbalance contributes to progressive structural weakening of the femoral head [20].Table 5. Role of Biomarkers in AVNFH and their prognostic significance
 |
| |
|
Inflammatory markers such as tumor necrosis factor alpha and interleukin 6 indicate activation of immune pathways and contribute to osteoclast mediated bone destruction and inhibition of bone regeneration [17]. Elevated levels of these cytokines often correlate with disease activity and may reflect ongoing tissue damage.Coagulation markers including D dimer and fibrinogen reflect hypercoagulable states that predispose to microvascular thrombosis and impaired perfusion. In patients with antiphospholipid syndrome, detection of beta2 glycoprotein antibodies provides additional diagnostic and prognostic information and identifies patients at particularly high risk for vascular occlusion [10].Emerging research also highlights the role of endothelial dysfunction markers and oxidative stress indicators, which further support the concept of avascular necrosis as a systemic vascular and metabolic disorder.Together, these biomarkers reflect key mechanisms involved in disease progression, including bone remodeling imbalance, systemic inflammation, and vascular dysfunction. Their integration into clinical practice, particularly in combination with imaging findings, may improve early diagnosis, allow more accurate risk stratification, and support the development of personalized management strategies.
6. Treatment Strategies
Management of avascular necrosis of the femoral head depends on disease stage, extent of necrosis, lesion location, and patient-specific factors such as age, comorbidities, and underlying rheumatic disease activity. The primary goals include pain reduction, preservation of joint structure, prevention of femoral head collapse, and restoration of function. Current strategies combine conservative, pharmacological, regenerative, and surgical approaches in a stage dependent and increasingly personalized manner [3,26].Early diagnosis plays a decisive role in treatment success. Joint preserving strategies demonstrate the greatest efficacy before structural collapse occurs, whereas advanced stages require reconstructive or replacement procedures. Therefore, treatment algorithms strongly rely on imaging based staging systems such as ARCO and Steinberg classifications.Conservative management plays a key role in early stages of disease before structural collapse occurs. Load reduction through the use of crutches decreases mechanical stress on the femoral head and may slow disease progression by limiting microfracture formation within the subchondral bone [26].Nonsteroidal anti inflammatory drugs provide symptomatic relief by reducing pain and inflammation. However, these agents do not influence the underlying ischemic or structural pathological process and should be considered supportive rather than disease modifying therapy.Bisphosphonates reduce osteoclast activity, inhibit bone resorption, and help preserve trabecular architecture. Clinical studies report that these agents decrease the risk of femoral head collapse by approximately 40 to 50 percent in early stage disease. Their effect appears particularly relevant in patients with small to medium sized lesions [3].Anticoagulant therapy is indicated in patients with hypercoagulable states, particularly in antiphospholipid syndrome. These agents improve microcirculation, prevent thrombotic occlusion of intraosseous vessels, and may reduce progression of ischemic damage [10].Pentoxifylline improves blood rheology, reduces blood viscosity, and enhances microvascular perfusion. It may contribute to improved oxygen delivery in ischemic bone tissue and has been investigated as adjunctive therapy in early disease stages.Hyperbaric oxygen therapy increases tissue oxygenation, stimulates angiogenesis, and enhances osteoblast activity. Clinical observations demonstrate improved perfusion, reduction of bone marrow edema, and potential delay in disease progression, although high quality randomized evidence remains limited [3].In addition, lifestyle modifications such as reduction of alcohol intake, smoking cessation, and control of metabolic risk factors may contribute to improved outcomes and should be integrated into early management strategies (table 6).Table 6. Available Treatment Strategies by Disease Stage
 |
| |
|
Optimization of underlying rheumatic disease treatment represents a critical component of management. Persistent systemic inflammation and glucocorticoid exposure significantly contribute to disease progression, therefore targeted control of these factors is essential.Clinicians must minimize glucocorticoid exposure whenever possible by using the lowest effective dose and shortest duration. This strategy directly reduces the risk of osteonecrosis and limits further vascular and cellular damage [4,5].Steroid sparing agents such as cyclophosphamide and mycophenolate mofetil allow effective control of autoimmune activity while reducing cumulative glucocorticoid dose. These agents improve long term outcomes by suppressing inflammation, reducing endothelial injury, and preventing further microvascular compromise [9].Biological therapies provide targeted modulation of immune pathways. Rituximab reduces B cell mediated immune activation, while belimumab inhibits B lymphocyte stimulator signaling. Janus kinase inhibitors suppress intracellular cytokine signaling and reduce production of proinflammatory mediators such as interleukin 6 and tumor necrosis factor alpha [9].These therapeutic approaches aim to reduce systemic inflammation, improve endothelial function, and limit vascular injury. As a result, they may indirectly slow the progression of avascular necrosis and improve overall disease prognosis.Emerging strategies also include combination therapy that integrates immunomodulation with vascular protective agents, which reflects the multifactorial nature of disease pathogenesis.Regenerative TherapyRegenerative medicine has emerged as one of the most promising approaches for early stage avascular necrosis. These therapies aim not only to halt disease progression but also to restore bone structure and vascular integrity.Stromal vascular fraction derived from adipose tissue contains a heterogeneous population of mesenchymal stem cells, endothelial progenitor cells, pericytes, and immunomodulatory cells. These components collectively support tissue repair and regeneration [27].Mesenchymal stem cells promote osteogenesis by differentiating into osteoblasts and enhancing bone formation. Endothelial progenitor cells stimulate angiogenesis and restore microcirculation within the necrotic area. In addition, immunomodulatory effects reduce local inflammation and improve the microenvironment for tissue regeneration.These combined effects enhance angiogenesis, stimulate osteogenesis, and modulate inflammatory responses within the necrotic region. As a result, regenerative therapy promotes restoration of microcirculation, improves structural stability, and delays disease progression.Clinical studies demonstrate encouraging outcomes. Reports indicate joint survival rates of up to 80 to 85 percent at six years following treatment, particularly in early stage disease with limited lesion size. These therapies also reduce pain and improve functional outcomes [27].Despite promising results, challenges remain regarding standardization of cell preparation, dosing, and long term efficacy. Ongoing research continues to refine these approaches and evaluate their role in routine clinical practice.Surgical TreatmentSurgical intervention becomes necessary when conservative and pharmacological measures fail or when structural damage progresses beyond the capacity for biological repair.Core decompression represents the standard surgical procedure in early stages. The technique reduces intraosseous pressure, improves blood flow, and stimulates reparative processes within the femoral head. Clinical evidence supports its effectiveness in delaying disease progression and reducing symptoms, particularly in small to medium sized lesions [26].Stem cell augmented procedures enhance the effects of core decompression by introducing osteogenic and angiogenic cells directly into the necrotic region. These approaches improve bone regeneration, increase vascularization, and enhance structural stability, which leads to improved long term outcomes [27].Osteotomy may be considered in selected patients with localized lesions. This procedure redistributes mechanical load away from the necrotic area and shifts weight bearing to viable bone regions. Although technically demanding, it may delay the need for joint replacement in younger patients.Total hip arthroplasty remains the treatment of choice in advanced stages characterized by femoral head collapse and secondary osteoarthritis. Modern surgical techniques, including improved implant design and minimally invasive approaches, achieve high success rates, durable outcomes, and significant improvement in quality of life (table 6) [3].However, arthroplasty in younger patients presents challenges related to implant longevity and the potential need for revision surgery. Therefore, joint preserving strategies remain preferable whenever feasible.Emerging Trends in TreatmentCurrent trends emphasize minimally invasive techniques combined with biological augmentation. Integration of regenerative medicine with surgical procedures represents a shift toward restoring native joint structure rather than replacing it. Future directions include development of targeted therapies that address specific pathophysiological mechanisms such as angiogenesis impairment, oxidative stress, and endothelial dysfunction. Personalized treatment strategies based on imaging, biomarkers, and genetic profiles may further improve outcomes.
7. Conclusions
Avascular necrosis of the femoral head in rheumatology represents a complex and multifactorial disorder driven by the interaction of vascular impairment, immune dysregulation, metabolic abnormalities, and pharmacological exposure. Current evidence demonstrates that impaired microcirculation initiates the disease, while inflammatory, cellular, and molecular mechanisms accelerate progression toward structural collapse and joint dysfunction [2,3].The clinical course often begins without symptoms, which delays diagnosis and limits the effectiveness of early interventions. At the same time, disease progression may occur rapidly, particularly in patients with systemic lupus erythematosus and antiphospholipid syndrome. These features highlight the need for proactive clinical strategies aimed at early detection, continuous monitoring, and prevention of irreversible structural damage [6,10].Active screening of high risk populations remains essential, especially in patients receiving long term glucocorticoid therapy or presenting with autoimmune disease. Clinicians should apply rational glucocorticoid use by minimizing dose and duration whenever possible, while ensuring adequate control of underlying disease activity. Early use of magnetic resonance imaging enables detection of subclinical disease and significantly improves the likelihood of successful joint preserving treatment [23,24].In addition, integration of imaging findings with laboratory biomarkers and clinical risk factors allows more precise stratification of patients and supports individualized therapeutic decision making. A multidisciplinary approach that combines rheumatological management, orthopedic evaluation, and advanced imaging techniques is critical for optimizing outcomes.Therapeutic strategies should prioritize early stage intervention, where conservative and regenerative approaches may effectively delay or prevent structural collapse. In advanced stages, timely surgical intervention remains essential to restore function and improve quality of life.Future research should focus on biomarker driven risk prediction, refinement of regenerative therapies, and development of targeted treatments addressing key pathogenic pathways such as angiogenesis impairment, oxidative stress, and endothelial dysfunction. Improved understanding of disease mechanisms may enable earlier intervention and more effective prevention strategies.Overall, early recognition, individualized management, and integration of emerging diagnostic and therapeutic approaches remain fundamental for reducing disease burden and preserving joint function in patients with avascular necrosis of the femoral head.
References
| [1] | Arbab D, König DP. Atraumatic femoral head necrosis epidemiology etiology diagnosis and treatment. Deutsches Ärzteblatt Int. 2016; 113(3): 31. |
| [2] | Guerado E, Caso E. The physiopathology of avascular necrosis of the femoral head an update. Injury. 2016; 47: S16–S26. |
| [3] | Konarski W, et al. Avascular necrosis of femoral head overview and current state of the art. Int J Environ Res Public Health. 2022; 19(12): 7348. |
| [4] | Chang C, Greenspan A, Gershwin ME. The pathogenesis diagnosis and clinical manifestations of steroid induced osteonecrosis. J Autoimmun. 2020; 110: 102460. |
| [5] | Wang A, Ren M, Wang J. The pathogenesis of steroid induced osteonecrosis of the femoral head a systematic review. Gene. 2018; 671: 103–109. |
| [6] | Nevskaya T, Gamble MP, Pope JE. A meta analysis of avascular necrosis in systemic lupus erythematosus prevalence and risk factors. Clin Exp Rheumatol. 2017; 35(4): 700–710. |
| [7] | Joo YB, et al. Prevalence incidence and associated factors of avascular necrosis in systemic lupus erythematosus. Rheumatol Int. 2015; 35(5): 879–886. |
| [8] | Gladman DD, et al. Osteonecrosis in systemic lupus erythematosus prevalence patterns outcomes and predictors. Lupus. 2018; 27(1): 76–81. |
| [9] | Tsai HL, et al. Epidemiology and risk factors associated with avascular necrosis in autoimmune diseases. Korean J Intern Med. 2022; 37(4): 864. |
| [10] | Evangelidis P, et al. Avascular necrosis of the femoral head in antiphospholipid syndrome. Hematol Rep. 2025; 17(2): 15. |
| [11] | Ikeuchi K, et al. Epidemiology of nontraumatic osteonecrosis of the femoral head in Japan. Mod Rheumatol. 2015; 25(2): 278–281. |
| [12] | Nadi F, et al. Asymptomatic multifocal avascular necrosis in systemic lupus erythematosus. BMC Rheumatol. 2024; 8(1). |
| [13] | Buddhiraju A, et al. Epidemiology management and surgical trends in osteonecrosis of the femoral head. J Arthroplasty. 2025. |
| [14] | Dhital R, et al. Trends in avascular necrosis and arthroplasty in patients with systemic lupus erythematosus and rheumatoid arthritis. 2024. |
| [15] | Bai R, et al. Roles of osteocyte apoptosis in steroid induced avascular necrosis of the femoral head. Genet Mol Res. 2016; 15(1). |
| [16] | Chen K, et al. Steroid induced osteonecrosis of the femoral head mechanisms and oxidative stress. Int J Biol Sci. 2020; 16(11): 1888. |
| [17] | Zheng L, et al. TNF alpha mediated mechanisms in avascular necrosis of the femoral head. Cell Biol Int. 2020; 44(9): 1881–1889. |
| [18] | Ma T, et al. Pathogenesis of hormone induced osteonecrosis based on microvascular mechanisms. J Orthop Surg Res. 2024; 19(1). |
| [19] | Duan P, et al. PPAR gamma signaling in steroid induced osteonecrosis of the femoral head. Stem Cell Res Ther. 2022; 13(1). |
| [20] | Li L, et al. Mechanisms and biomarkers of steroid induced osteonecrosis. Ann Med. 2024; 56(1). |
| [21] | Choi HR, Steinberg ME, Cheng EY. Osteonecrosis of the femoral head diagnosis and classification systems. Curr Rev Musculoskelet Med. 2015; 8: 210–220. |
| [22] | Sultan AA, et al. Classification systems of hip osteonecrosis an updated review. Int Orthop. 2019; 43: 1089–1095. |
| [23] | Manenti G, et al. Imaging in diagnosis and management of femoral head osteonecrosis. Clin Cases Miner Bone Metab. 2016; 12: 31. |
| [24] | Zhang YZ, et al. Accuracy of MRI diagnosis of early osteonecrosis of the femoral head. J Orthop Surg Res. 2018; 13(1). |
| [25] | Iqbal B, Currie G. Value of SPECT CT in diagnosis of avascular necrosis of the femoral head. Radiography. 2022; 28(2): 560–564. |
| [26] | Calori GM, et al. Core decompression and biotechnologies in treatment of avascular necrosis. EFORT Open Rev. 2017; 2(2): 41–50. |
| [27] | Tantuway V, et al. Stromal vascular fraction therapy in osteonecrosis long term outcomes. Indian J Orthop. 2024; 58(1): 68–78. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML