-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1941-1944
doi:10.5923/j.ajmms.20261604.78
Received: Mar. 23, 2026; Accepted: Apr. 12, 2026; Published: Apr. 18, 2026

Clinical-Dynamic Evaluation of Social Functioning and Quality of Life in Geriatric Patients with Depressive Disorders and Psychoorganic Syndrome
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKuchimova Charos Azamatovna, Ochilov Ulugbek Usmonovich, Boltaev Kakhramon Kakharovich
Samarkand State Medical University, Uzbekistan
Correspondence to: Kuchimova Charos Azamatovna, Samarkand State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Clinical-dynamic analysis of social functioning and quality-of-life indicators in elderly patients with depressive disorders comorbid with psychoorganic syndrome. Elderly patients with this comorbidity often experience significant declines in physical and intellectual productivity, difficulties in performing daily and household activities, and a reduction in self-care ability, which directly affects their quality of life [1]. The combination of depressive and psychoorganic symptoms leads to reduced social activity, decreased interaction with family and the community, and an overall decline in social adaptation [2,3]. Assessing life satisfaction, intellectual and physical productivity, and psychosocial functioning allows for qualitative and quantitative evaluation of disease impact, helping to identify patients at high risk of functional decline. This clinical-dynamic analysis is essential for detecting functional impairments, monitoring disease progression, and planning comprehensive care strategies for elderly patients [4,5].
Keywords: Depression, Psycho-organic syndrome, Quality of life, Social activity, Intellectual productivity, Psychodynamics
Cite this paper: Kuchimova Charos Azamatovna, Ochilov Ulugbek Usmonovich, Boltaev Kakhramon Kakharovich, Clinical-Dynamic Evaluation of Social Functioning and Quality of Life in Geriatric Patients with Depressive Disorders and Psychoorganic Syndrome, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1941-1944. doi: 10.5923/j.ajmms.20261604.78.
Article Outline
1. The Purpose of the Study
- The objective is to determine the clinical and dynamic characteristics of social functioning and quality-of-life indicators in elderly patients with depressive disorders comorbid with psychoorganic syndrome of vascular origin.
2. Research Tasks
- 1. To study the clinical characteristics of depressive disorder in elderly patients with comorbid psychoorganic disturbances of vascular origin. 2. To compare the features of social functioning in elderly patients with depressive disorder in the presence and absence of psychoorganic disturbances of vascular origin. 3. To analyze the dynamics of the identified impairments (depressive and psychoorganic), as well as indicators of social functioning during the course of therapy.
3. Research Materials and Methods
- During the study, clinical-psychopathological examination methods were used, along with standard clinical scales to assess the severity of mental disorders, including the Hamilton Depression Rating Scale, the Mini-Mental State Examination (MMSE) for the assessment of cognitive functions, the Clinical Global Impression (CGI) scale, and mathematical-statistical methods for data processing. The study was conducted in 2023–2025 at the Samarkand branch (outpatient and inpatient departments) of the Psychiatry Service of the Republican Specialized Scientific and Practical Medical Center for Psychiatry. The main group consisted of 105 patients undergoing treatment for depressive disorders associated with psychoorganic disorders of vascular origin (22 male patients and 83 female patients aged 60–80 years). The control group included 53 patients diagnosed with depressive disorders. Patients included in the study met the diagnostic criteria and course specifications according to ICD-10 classification: F33 (Recurrent Depressive Disorder) and F06.7 (Mild Cognitive Disorder of vascular origin, not reaching the level of dementia).
4. Research Results
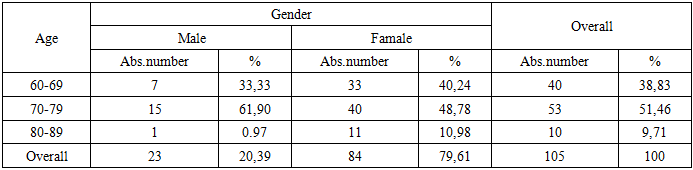
- When the study materials were analyzed from a clinical-statistical perspective, patients aged 70–79 years predominated in both the main and control groups (mean age – 71.06 ± 1.09 years). In the main group, the majority of patients were female (79.62%). In the control group, the mean age of patients was 73.36 ± 1.62 years, and female patients also predominated (84.31%, n=43). Undoubtedly, these indicators can be explained by specific demographic ratios in the general population and trends identified in several epidemiological studies of morbidity in late life.In the present study, among patients over 60 years of age, the male-to-female ratio was 1:1.5 and this trend is particularly characteristic of depressive disorders [6,7]. For example, it has been documented that depressive disorders occur three times more frequently in elderly women than in men of the same age [8,9].
|
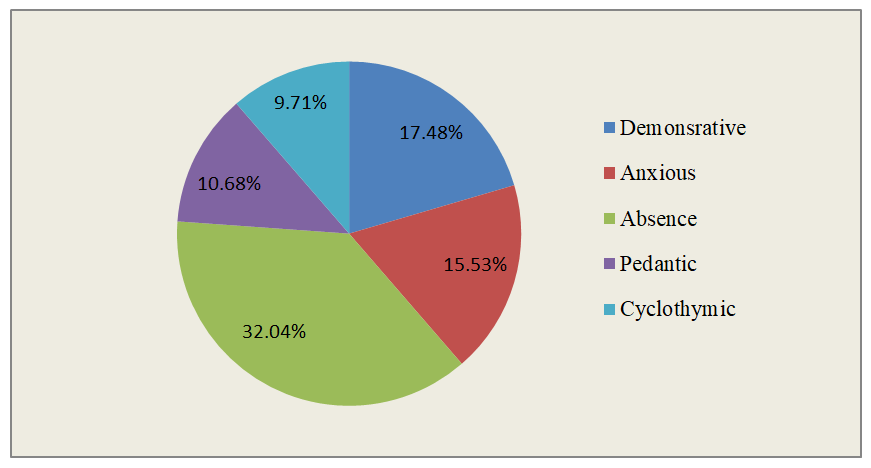 | Graph 1. Patients’ personality traits |
|
|
|

5. Conclusions
- The results of the study indicate that depressive disorders in elderly patients comorbid with vascular-origin psychoorganic syndrome lead to significant declines in social functioning and quality of life. In the main group, patients showed a marked reduction in physical and intellectual productivity, experienced difficulties in daily activities and household tasks, and had decreased self-care ability, which was more pronounced compared to the control group. Particularly, low satisfaction with physical and intellectual performance, as well as reduced life satisfaction and subjective well-being, were noted as key characteristics. Clinical-dynamic analysis demonstrated that depressive symptoms combined with vascular-origin cognitive impairment are a major cause of reduced social adaptation and functional independence in elderly patients. Furthermore, the comorbidity of depressive disorders with psychoorganic syndrome in older adults is clinically associated with unfavorable outcomes, characterized by social withdrawal and low quality-of-life indicators. These findings highlight the importance of early diagnosis, comprehensive therapy, and psychosocial rehabilitation interventions for this patient population.