-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1935-1940
doi:10.5923/j.ajmms.20261604.77
Received: Mar. 7, 2026; Accepted: Mar. 26, 2026; Published: Apr. 18, 2026

Outcomes of Skin Grafting in Post-Burn Scar Deformities of the Shoulder Joint
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSulaymonova X. H., Askhanov Z. P.
Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Sulaymonova X. H., Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Post-burn scar deformities of the shoulder joint remain one of the most challenging problems in reconstructive surgery, often leading to functional limitations and cosmetic defects that significantly affect patients’ quality of life. This study aimed to evaluate the effectiveness of skin grafting in the surgical management of post-burn scar deformities of the shoulder joint. The study included 42 patients with cicatricial deformities in the shoulder joint region. All patients were divided into two groups: the main group (21 patients), in whom improved tactical and technical approaches to skin grafting were applied, and the control group (21 patients), who received conventional surgical treatment. Early and long-term postoperative outcomes were assessed using physiological parameters, including thermometry and oximetry, as well as clinical evaluation of functional and cosmetic results. The analysis identified several factors that directly and indirectly influenced the treatment outcomes. These included the extent and localization of scar tissue, the condition of surrounding tissues, and the chosen surgical technique. The proposed tactical and technical approaches demonstrated improved effectiveness, increasing the proportion of good outcomes in the main group to 57.1%, while reducing the rate of unsatisfactory outcomes to 4.8%. The results indicate that the optimized surgical strategy for skin grafting can significantly improve functional recovery and cosmetic outcomes in patients with post-burn scar deformities of the shoulder joint. These findings may contribute to improving reconstructive surgical techniques and postoperative rehabilitation strategies.
Keywords: Shoulder joint, Post-burn scar deformity, Skin grafting, Thermometry, Oximetry, Reconstructive surgery, Functional outcomes
Cite this paper: Sulaymonova X. H., Askhanov Z. P., Outcomes of Skin Grafting in Post-Burn Scar Deformities of the Shoulder Joint, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1935-1940. doi: 10.5923/j.ajmms.20261604.77.
1. Introduction
- Burn injuries continue to pose a significant clinical and public health challenge worldwide, as they frequently result in scars that solidify into contractures, leading to long-term functional impairment and reduced quality of life. Contractures occur when excessive scar tissue forms across joints after deep thermal injury, restricting range of motion and causing disability; surgical intervention is often required to restore function and reduce disability [1,2]. Scar contractures result from abnormal wound healing involving excessive tissue contraction, fibrosis, and disrupted collagen remodeling, leading to persistent tension across joints and reduced elasticity of skin and soft tissues. Effective surgical management is therefore critical to prevent progressive disability and deformity [3]. Surgical release of scar contractures followed by appropriate defect coverage remains the cornerstone of reconstructive management. Evidence from a single-center 10-year retrospective cohort study demonstrates that flaps, such as local and expanded flaps, are associated with significantly lower rates of contracture recurrence and better functional satisfaction compared with full-thickness skin grafts alone [2,4]. Minimally invasive techniques for contracture release have also been described as safe and effective adjuncts to traditional reconstructive approaches. A retrospective case series involving a novel subcutaneous contracture release method showed substantial improvements in joint range of motion and Vancouver Scar Scale scores, with high patient satisfaction and minimal complications, suggesting that such techniques can enhance function after contracture formation [5]. Flap-based reconstruction is supported by systematic evidence as a reliable strategy for joint contracture management, with low rates of total flap loss and contracture recurrence in delayed reconstruction settings. Meta-analytic data indicate that free tissue transfer for joint contracture produces high contracture resolution and low recurrence, with acceptable complication profiles, underscoring the value of flap reconstructions in complex cases [6,7]. Local flaps such as Z-plasty and its modifications remain widely used for smaller defects, offering good functional and cosmetic outcomes with comparatively low complication rates, especially where adjacent healthy skin is available for transposition [8]. Comprehensive reviews in burn reconstructive surgery emphasize the integration of surgical and non-surgical modalities including scar prevention, physical rehabilitation, and contracture release to optimize both functional outcomes and quality-of-life metrics [3,9]. Despite these advances, the literature also highlights limitations: most studies remain observational, with heterogenous outcome measures, and definitive, large-scale randomized controlled trials are scarce. This underscores the need for standardized outcome reporting to better compare reconstructive strategies and guide clinical decision-making [3,10]. In summary, post-burn scar contracture management particularly around functional joints remains a clinically significant problem with profound implications for mobility and daily function. Surgical release combined with reconstructive techniques, especially flap-based solutions, offers improved functional results and lower recurrence relative to skin grafts alone, while adjunctive and minimally invasive procedures may further enhance recovery when integrated into comprehensive care protocols [1,2,4,5,6].Research objective: To improve the tactical and technical approaches in enhancing the outcomes of skin grafting procedures for post-burn scar deformities of the shoulder joint.
2. Materials and Methods
- A total of 47 patients with post-burn scar deformities of the shoulder joint who presented to the Republican Scientific Center for Emergency Medical Care and its branches between 2020 and 2024 were included in the study. The patients were divided into two groups: the main group comprised 26 patients (17 males, 9 females) with a mean age of 34.6 ± 4.2 years. In this group, skin grafting procedures were performed using improved tactical and technical approaches. The control group included 21 patients (13 males, 8 females) with a mean age of 35.2 ± 3.8 years, who underwent skin grafting using conventional methods.The following assessment methods were applied:1. Clinical examination: Scar type, size, location, relation to surrounding tissues, and joint range of motion (ROM) were evaluated.2. Thermometry: Skin surface temperature was measured using a “Termotest-1” device. Measurements were taken at the scar center, at the border between scarred and healthy tissue, and in a control area of healthy skin. Assessments were conducted preoperatively, and at 20 minutes, 1, 3, 7, and 14 days postoperatively.3. Oximetry: Skin oxygen saturation was evaluated using a pulse oximeter (“Oxitest-2”). Measurement points and timing were identical to those used in thermometry.4. Functional assessment: Joint mobility was quantified according to the ROM scale.5. Cosmetic evaluation: Parameters such as the color, elasticity, surface smoothness of the grafted skin, and development of pathological scarring were assessed.Surgical technique: All procedures were performed under general endotracheal anesthesia. The operative field was sterilized using the Filonchikov-Gross method: 70% alcohol for 2 minutes, 5% iodine-alcohol solution for 2 minutes, followed by 70% alcohol three times. Dense scars restricting joint mobility were outlined with a sterile marker to indicate areas requiring excision. Layer-by-layer incisions were made perpendicular to the marking line using a scalpel. In cases of hypertrophic or keloid scars, significant intraoperative bleeding was noted, whereas bleeding was minimal in other cases. Hemostasis of larger vessels was achieved using electrocautery, and smaller vessels were ligated mechanically or chemically. Layered tissue separation using sharp and blunt dissection minimized trauma to vessels and tendons. The separation of scar tissue from healthy tissue restored movement around the joint axis. Special attention was given to the graft recipient site: the area was designed with flaps resembling swallow wings at both ends to preserve joint mobility and prevent secondary contractures. After applying an aseptic dressing to the wound surface, the skin graft was harvested from the inner aspect of the upper third of the thigh, shaped like a boat. The donor site was prepared with sterile drapes and antiseptic treatment (70% alcohol for 2 minutes, 5% iodine-alcohol for 2 minutes, and 70% alcohol). Skin incisions were made down to the subcutaneous fat, and the graft was carefully separated while preserving underlying adipose tissue, as it affects graft integration. The harvested graft was applied to the recipient site and fixed with continuous interrupted sutures. In selected cases, additional perpendicular sutures were placed to ensure adhesion of the graft to the underlying tissue, and small incisions were made to prevent hematoma formation. An aseptic dressing and opposing-site gypsum splint were applied. In cases of extensive donor skin harvesting, closure of the donor wound involved sharp and blunt dissection down to the muscular aponeurosis, ligation or cauterization of bleeding vessels, and layered suturing to reduce dead space. A rubber drain was placed under the graft to prevent fluid accumulation. The surgical procedure was completed with aseptic dressing.Postoperative evaluation of the recipient site was conducted on days 5–6. Early outcomes were assessed between 14 and 21 days postoperatively using thermometry, oximetry, finger tests, and visual inspection. All patients were followed through outpatient visits to monitor early results.
3. Results
- Description of Preoperative Scars. The characteristics of scar deformities in the shoulder joint area are presented, analysis of postoperative outcomes was carried out using skin thermometry at 20 minutes, 1, 3, 7, and 14 days after the surgery (Figure 1).
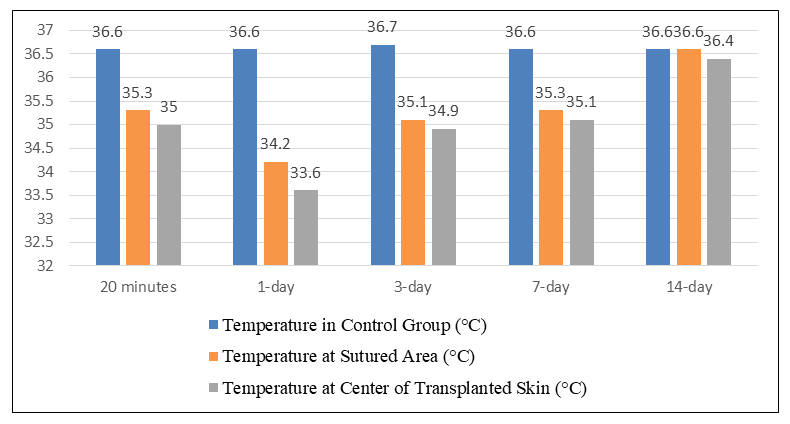 | Figure 1. Postoperative outcomes in patients of the control group |
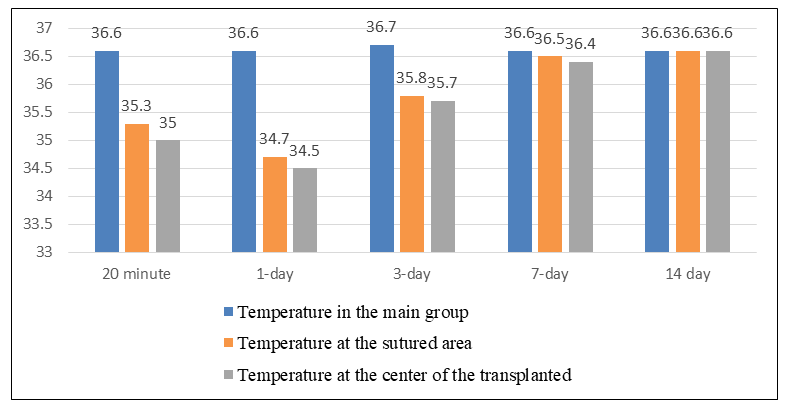 | Figure 2. Postoperative outcomes in patients of the main group |
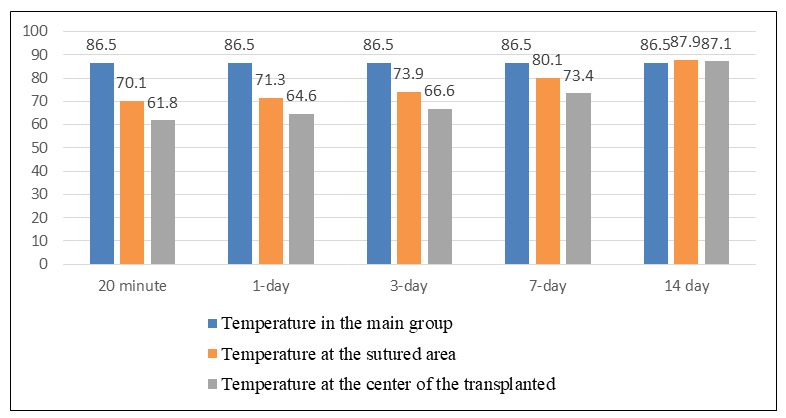 | Figure 3. Postoperative outcomes in patients of the control group |
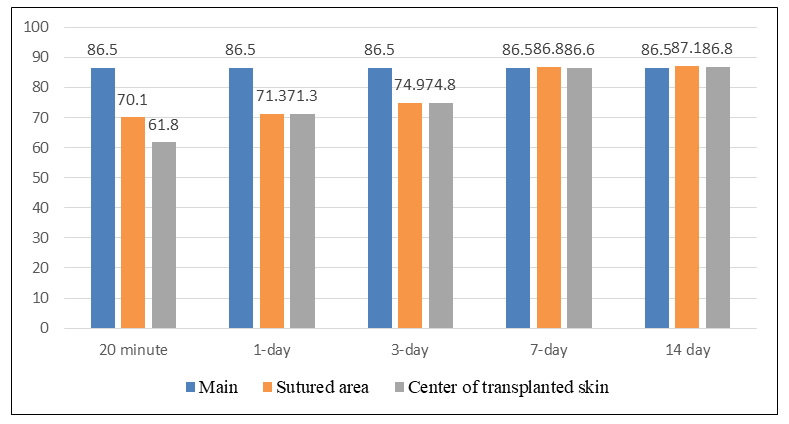 | Figure 4. Postoperative outcomes in patients of the main group |
 | Figure 5. Patient M. Post-burn scar deformities of both shoulders, elbows, chest, scapular region, lumbar region, both gluteal regions, and both thighs (posterior view). Complication: Grade III contracture of both shoulder joints |
 | Figure 6. The surgical field in this patient: scar deformity and contracture of the right shoulder joint (anterior view) |
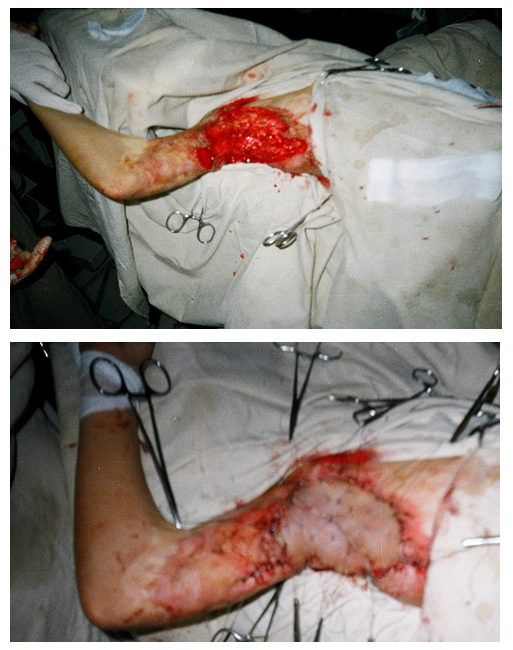 | Figure 7. The surgical field in this patient: scar deformity and contracture of the right shoulder joint |
 | Figure 8. Long-term postoperative outcome (1 year after surgery) |
4. Discussion
- Analysis of the outcomes of skin grafting procedures for the correction of post-burn scar deformities of the shoulder joint demonstrated that the improvement of tactical and technical approaches made it possible to increase the proportion of favorable outcomes in the main group up to 57.1%, while reducing unsatisfactory results to 4.8%.Preoperative assessment of the physiological characteristics of scars revealed that in hypertrophic and keloid scars, a significant increase in temperature at the center of the scar (39.3 ± 1.6°C) and a higher level of oxygen saturation (96.2 ± 7.1 mmHg) can be explained by increased blood circulation and enhanced metabolic activity in the scar tissue. In contrast, atrophic scars were characterized by a decrease in temperature (35.3 ± 1.3°C) and lower oximetric values (80.8 ± 3.9 mmHg), indicating insufficient blood circulation and impaired tissue trophism.In the postoperative period, the dynamics of physiological indicators allowed objective evaluation of graft integration and restoration of blood circulation. In the main group, normalization of thermometry and oximetry indicators occurred more rapidly compared with the control group (by the 7th postoperative day), which confirms the effectiveness of the improved tactical and technical approaches.Analysis of complications showed that the most common complications included epidermal peeling (9.5%), partial skin necrosis (7.1%), and subgraft hematoma (7.1%). Prevention of these complications requires improvement of operative field management techniques, meticulous hemostasis, as well as proper preparation and fixation of the graft.Analysis of functional outcomes demonstrated that complete restoration of joint mobility was achieved in 85.7% of patients in the main group, which is 14.3% higher than in the control group. In addition, grade III contracture was not observed in the main group, whereas it was recorded in 4.8% of cases in the control group. These findings confirm the functional effectiveness of the proposed surgical approaches.Regarding cosmetic outcomes, it is noteworthy that unsatisfactory cosmetic results were more frequently observed in the main group (28.6%). This may be associated with the greater initial severity of scarring in this group (grade III contracture was present in 81% of patients). Nevertheless, the overall number of complications negatively affecting cosmetic results in the main group was two times lower compared with the control group (23.8% vs. 47.6%).Analysis of physiological indicators in cases with complications demonstrated that in partial skin necrosis, a decrease in temperature to 33.1°C and a drop in oximetric values to 51.1 mmHg represent signs of tissue death and constitute an indication for necrectomy. In contrast, in cases of epidermal peeling, the temperature did not decrease below 35.1°C, and oximetric values remained above 74.8 mmHg, indicating preservation of the viability of deeper skin layers.
5. Conclusions
- 1. Skin grafting in post-burn scar deformities of the shoulder joint is an effective treatment method that allows improvement of both functional and cosmetic outcomes.2. Preoperative assessment of the physiological characteristics of scars (thermometry and oximetry) enables proper determination of surgical tactics and allows prediction of possible complications.3. In hypertrophic and keloid scars, a significant increase in temperature at the center of the scar (39.3 ± 1.6°C) and a high level of oxygen saturation (96.2 ± 7.1 mmHg) indicate enhanced blood circulation, whereas in atrophic scars a decrease in these indicators (35.3 ± 1.3°C and 80.8 ± 3.9 mmHg) reflects insufficient blood circulation.4. The dynamics of postoperative physiological indicators make it possible to objectively assess graft integration. In the main group, normalization of thermometry and oximetry indicators was observed by the 7th postoperative day, while in the control group it occurred by the 14th day.5. The improved tactical and technical approaches reduced the rate of direct complications in the main group from 33.3% to 14.3%, and indirect complications from 19.0% to 9.5%.6. Good functional outcomes were observed in 85.7% of patients in the main group, which is 14.3% higher than in the control group. Grade III contracture was not observed in the main group.7. Analysis of physiological indicators in cases with complications showed that a decrease in temperature to 33.1°C and a reduction in oximetric values to 51.1 mmHg represent reliable signs of tissue necrosis and constitute an indication for necrectomy.8. To improve the outcomes of skin grafting in the correction of shoulder joint scar deformities, it is advisable to apply a comprehensive approach, including thorough preoperative evaluation, improved surgical techniques, and early postoperative rehabilitation as part of an integrated treatment algorithm.