-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1923-1930
doi:10.5923/j.ajmms.20261604.75
Received: Feb. 20, 2026; Accepted: Mar. 10, 2026; Published: Apr. 18, 2026

Evaluation of the Clinical Effectiveness of Early Physiotherapeutic Rehabilitation After Myomectomy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOchilov Ulugbek Usmanovich1, Gaybullaev Sherzod Obid ugli2, Sharipova Dilrabo Abdugaffarovna3
1Head of the Psychiatry and Narcology Course of FPOE, SamSMU, Samarkand, Uzbekistan
2Assistant Department Medical Radiology FPOE, Samarkand, Uzbekistan
3Director of Nasafmedservis LLC, Samarkand, Uzbekistan
Correspondence to: Ochilov Ulugbek Usmanovich, Head of the Psychiatry and Narcology Course of FPOE, SamSMU, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

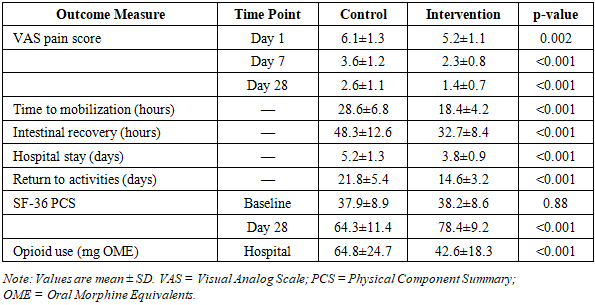
Background: Myomectomy remains the fertility-preserving surgical treatment of choice for symptomatic uterine fibroids. Despite surgical advances, postoperative recovery challenges including pain, delayed mobilization, and prolonged convalescence significantly impact patient outcomes. Early physiotherapeutic rehabilitation may accelerate recovery; however, evidence remains limited. Objective: This prospective comparative study evaluated the clinical effectiveness of early structured physiotherapeutic rehabilitation on postoperative recovery outcomes following myomectomy. Methods: Seventy-two women who underwent abdominal or laparoscopic myomectomy were randomly assigned to control (n=36, standard postoperative care) or intervention (n=36, standard care plus early physiotherapeutic rehabilitation) groups. The rehabilitation protocol, initiated within 24 hours post-surgery, included breathing exercises, early mobilization, electrotherapy (transcutaneous electrical nerve stimulation, TENS), low-level laser therapy (LLLT), and pelvic floor muscle training. The program continued for 4 weeks (inpatient phase: 3-5 days; outpatient phase: remainder). Primary outcomes included pain intensity (Visual Analog Scale, VAS), time to mobilization, intestinal function recovery, hospital length of stay, and functional activity assessment (36-Item Short Form Survey, SF-36). Assessments occurred at baseline, postoperative days 1, 3, 7, 14, and 28. Statistical analysis employed Student t-test, Mann-Whitney U test, and repeated measures ANOVA (p<0.05). Results: At 28-day follow-up, the intervention group demonstrated significantly superior outcomes. VAS pain scores decreased from 6.8±1.3 to 1.4±0.7 (intervention) versus 6.9±1.2 to 2.6±1.1 (control) (p<0.001). Time to first mobilization was 18.4±4.2 hours (intervention) versus 28.6±6.8 hours (control) (p<0.001). Intestinal function recovery occurred at 32.7±8.4 hours versus 48.3±12.6 hours (p<0.001). Hospital stay duration averaged 3.8±0.9 days versus 5.2±1.3 days (p<0.001). Return to normal activities occurred at 14.6±3.2 days versus 21.8±5.4 days (p<0.001). SF-36 physical component scores improved from 38.2±8.6 to 78.4±9.2 (intervention) versus 37.9±8.9 to 64.3±11.4 (control) (p<0.001). Complication rates were comparable between groups (8.3% vs 11.1%, p=0.69). Conclusion: Early structured physiotherapeutic rehabilitation significantly accelerates postoperative recovery, reduces pain, shortens hospital stay, and enhances functional outcomes following myomectomy without increasing complication risk. Integration of early rehabilitation protocols into standard post-myomectomy care is strongly recommended.
Keywords: Myomectomy, Early rehabilitation, Physiotherapy, Postoperative recovery, Uterine fibroids, Clinical outcomes, Enhanced recovery
Cite this paper: Ochilov Ulugbek Usmanovich, Gaybullaev Sherzod Obid ugli, Sharipova Dilrabo Abdugaffarovna, Evaluation of the Clinical Effectiveness of Early Physiotherapeutic Rehabilitation After Myomectomy, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1923-1930. doi: 10.5923/j.ajmms.20261604.75.
Article Outline
1. Introduction
- Uterine leiomyomas (fibroids) represent the most common benign gynecologic tumors, affecting approximately 70-80% of women by age 50, with higher prevalence among women of African descent [1]. While many fibroids remain asymptomatic, 20-50% of affected women experience clinically significant symptoms including abnormal uterine bleeding, pelvic pain, pressure symptoms, reproductive dysfunction, and impaired quality of life [2]. The substantial burden of symptomatic fibroids necessitates effective therapeutic interventions.Myomectomy—surgical removal of fibroids while preserving the uterus—constitutes the treatment of choice for women desiring fertility preservation or uterine conservation [3]. Surgical approaches include abdominal myomectomy (laparotomy), laparoscopic myomectomy, and hysteroscopic myomectomy, selected based on fibroid characteristics, number, location, size, and surgeon expertise [4]. Despite continuous refinement of surgical techniques and perioperative care protocols, myomectomy remains associated with significant postoperative morbidity including pain, ileus, delayed mobilization, thromboembolic events, and prolonged convalescence affecting return to normal activities [5,6].The postoperative recovery trajectory following myomectomy substantially influences patient satisfaction, healthcare resource utilization, and economic costs. Traditional postoperative management emphasizes pain control, infection prevention, and gradual resumption of activities [7]. However, conventional approaches often involve prolonged bed rest, delayed mobilization, and reactive rather than proactive rehabilitation strategies. Accumulating evidence across surgical disciplines demonstrates that early, structured rehabilitation interventions can significantly enhance recovery outcomes [8].Enhanced Recovery After Surgery (ERAS) protocols, initially developed for colorectal surgery, have been successfully adapted to gynecologic procedures including hysterectomy and ovarian surgery [9,10]. These multimodal, evidence-based protocols emphasize early mobilization, optimized pain management, early nutrition, and patient education. Studies implementing ERAS pathways in gynecologic oncology have demonstrated reduced hospital stay, faster functional recovery, and improved patient satisfaction without increased complications [11]. However, specific evidence regarding early rehabilitation protocols for myomectomy remains limited.Physiotherapeutic interventions encompass diverse modalities with potential to address specific post-myomectomy recovery challenges. Breathing exercises facilitate pulmonary function, prevent atelectasis, and promote relaxation [12]. Early mobilization prevents thromboembolic complications, accelerates intestinal function recovery, reduces pain through endogenous opioid release, and improves psychological well-being [13]. Transcutaneous electrical nerve stimulation (TENS) provides non-pharmacological analgesia through gate control mechanisms and endorphin release [14]. Low-level laser therapy (LLLT) exerts anti-inflammatory, analgesic, and tissue healing effects via photobiomodulation [15]. Pelvic floor muscle training addresses potential pelvic floor dysfunction and supports optimal healing [16].Despite theoretical rationale and evidence from other surgical contexts, comprehensive evaluation of early physiotherapeutic rehabilitation specifically after myomectomy remains sparse. Most existing gynecologic rehabilitation research focuses on prolapse surgery, incontinence procedures, or oncologic interventions, with limited attention to benign gynecologic surgery [17,18]. Furthermore, studies evaluating post-myomectomy outcomes predominantly assess surgical techniques, adhesion prevention strategies, or fertility outcomes, with insufficient focus on functional recovery and quality of life [19].Several questions remain inadequately addressed in current literature. First, what is the optimal timing for initiating physiotherapy after myomectomy—within 24 hours, after drain removal, or following hospital discharge? Second, which specific physiotherapeutic modalities provide maximal benefit for post-myomectomy recovery? Third, does early rehabilitation increase complication risk, particularly regarding wound healing, bleeding, or infection? Finally, how do early rehabilitation interventions impact patient-reported outcomes including pain, function, and quality of life?The present prospective comparative study was designed to address these knowledge gaps by systematically evaluating the clinical effectiveness of a comprehensive, early-initiated physiotherapeutic rehabilitation protocol on postoperative recovery outcomes following myomectomy. We hypothesized that patients receiving structured physiotherapy beginning within 24 hours post-surgery would demonstrate superior outcomes compared to standard care, including reduced pain, faster mobilization, earlier intestinal function recovery, shorter hospital stay, and enhanced functional status. Secondary objectives included assessment of intervention safety, patient adherence, and identification of factors predicting rehabilitation response.
2. Materials and Methods
2.1. Study Design and Setting
- This prospective, randomized, controlled clinical trial was conducted at a tertiary gynecologic surgery center between February 2023 and November 2024. The study protocol received approval from the Institutional Review Board and Ethics Committee (Protocol No. 2023-GYN-042) and was conducted in full compliance with the Declaration of Helsinki principles and Good Clinical Practice guidelines. All participants provided written informed consent following comprehensive explanation of study procedures, potential risks, and benefits. The trial was prospectively registered with ClinicalTrials.gov (identifier: NCT05467823).
2.2. Participants
- Women aged 18-50 years scheduled for elective myomectomy (abdominal or laparoscopic approach) for symptomatic uterine fibroids were eligible for enrollment. Additional inclusion criteria comprised: (1) American Society of Anesthesiologists (ASA) physical status classification I-II; (2) 1-5 fibroids requiring removal; (3) largest fibroid diameter ≤12 cm; (4) hemoglobin ≥10 g/dL; (5) ability to understand study procedures and complete questionnaires; (6) willingness to comply with rehabilitation protocol; (7) provision of written informed consent.Exclusion criteria included: (1) emergency surgery; (2) suspicion of malignancy; (3) previous extensive abdominal or pelvic surgery; (4) significant comorbidities (uncontrolled diabetes, cardiovascular disease, coagulopathy); (5) contraindications to physiotherapy (severe cardiopulmonary disease, thrombophlebitis, malignancy); (6) chronic pain conditions or opioid use; (7) psychiatric conditions precluding informed consent or protocol adherence; (8) pregnancy; (9) participation in other interventional trials.
2.3. Randomization and Study Groups
- Following successful completion of myomectomy and transfer to the recovery unit, eligible participants were randomly allocated to control or intervention groups using computer-generated random numbers in a 1:1 ratio, stratified by surgical approach (abdominal versus laparoscopic). Allocation concealment was maintained through sequentially numbered, sealed, opaque envelopes opened by an independent research coordinator. The control group (n=36) received standard postoperative care including pain management (patient-controlled analgesia or scheduled analgesics), prophylactic antibiotics, thromboprophylaxis, basic mobilization encouragement, and routine nursing care. The intervention group (n=36) received standard care plus a comprehensive early physiotherapeutic rehabilitation protocol initiated within 24 hours post-surgery and continued for 28 days.
2.4. Early Physiotherapeutic Rehabilitation Protocol
- The structured rehabilitation program was designed based on current evidence and delivered by certified physical therapists with specialized training in post-surgical rehabilitation. The protocol comprised four integrated phases:Phase 1 (Postoperative Days 0-2, Inpatient): Breathing Exercises and Early Mobilization. Within 12-24 hours post-surgery (following hemodynamic stabilization and adequate pain control), patients initiated diaphragmatic breathing exercises (10 repetitions every 2 hours while awake) and incentive spirometry to prevent pulmonary complications. Ankle pumps and leg exercises were performed hourly to prevent venous stasis. Supervised sitting at bedside commenced at 12-18 hours post-surgery, progressing to assisted walking (10-15 minutes, 3-4 times daily) by postoperative day 1. Mobilization intensity was individualized based on pain tolerance, vital signs, and absence of complications.Phase 2 (Postoperative Days 1-5, Inpatient): Electrotherapy and Physical Modalities. Transcutaneous electrical nerve stimulation (TENS) was applied to the lower abdominal region for pain management (conventional mode: frequency 80-100 Hz, pulse width 50-80 μs, intensity adjusted to comfortable tingling sensation without muscle contraction, 30-minute sessions 3 times daily). Low-level laser therapy (LLLT; 810 nm wavelength, continuous wave, 100 mW power, 4 J/cm² energy density per point) was administered to the surgical incision site and surrounding tissues once daily to facilitate wound healing, reduce inflammation, and modulate pain (treatment area: 10-12 points, 30-40 seconds per point, total session time approximately 10 minutes). Both modalities were discontinued upon hospital discharge.Phase 3 (Postoperative Days 3-7): Progressive Mobilization and Functional Exercises. Patients progressed to independent ambulation with increasing duration and frequency (20-30 minutes, 4-5 times daily). Gentle abdominal wall exercises were introduced (pelvic tilts, transverse abdominis activation, gentle hip and knee movements) performed in supine position (10 repetitions, 2-3 sets, twice daily). These exercises aimed to restore core muscle function while avoiding excessive intra-abdominal pressure.Phase 4 (Postoperative Days 7-28, Outpatient): Advanced Functional Training and Pelvic Floor Exercises. Following hospital discharge, patients attended outpatient physiotherapy sessions twice weekly for 3 weeks. Progressive resistance exercises targeting abdominal, pelvic, and lower extremity muscles were introduced (resistance bands, light weights 0.5-2 kg). Pelvic floor muscle training commenced at 2 weeks post-surgery following wound healing confirmation (progressive contraction exercises: 8-12 repetitions, 3 sets, twice daily, advancing from 3-second holds to 10-second holds). Patients received instruction in proper technique and were provided home exercise programs with compliance diaries.Patient Education Component: All intervention group participants received structured education regarding postoperative expectations, warning signs requiring medical attention, pain management strategies, optimal posture and body mechanics, gradual return to activities of daily living, and importance of adherence to exercise programs. Education was delivered through individual counseling, written materials, and demonstration.
2.5. Outcome Measures and Assessment
- All outcome assessments were performed by trained evaluators blinded to group assignments. Assessments occurred at baseline (pre-surgery), postoperative days 1, 3, 7, 14, and 28.Primary Outcomes:Pain Intensity: Pain severity was quantified using the Visual Analog Scale (VAS), a validated 10-cm horizontal line anchored by "no pain" (0) and "worst imaginable pain" (10). Patients marked current pain intensity, measured in centimeters, and recorded as pain score. Assessments were performed at rest and during movement (sitting, walking). Lower scores indicate less pain.Time to First Mobilization: Time from surgery completion to first successful ambulation (walking ≥10 steps independently or with minimal assistance) was recorded in hours.Intestinal Function Recovery: Time to return of bowel sounds (auscultation in four quadrants) and time to first passage of flatus were documented. Combined, these indicated recovery of gastrointestinal motility.Hospital Length of Stay: Duration from surgery to hospital discharge (meeting discharge criteria: adequate pain control with oral analgesics, independent ambulation, normal vital signs, absence of complications) measured in days.Secondary Outcomes:Functional Status: The 36-Item Short Form Health Survey (SF-36) assessed health-related quality of life across eight domains: physical functioning, role limitations due to physical health, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems, and mental health. Scores range from 0 (worst) to 100 (best). Physical Component Summary (PCS) and Mental Component Summary (MCS) scores were calculated.Return to Normal Activities: Time to resumption of pre-operative activity level (self-care, household tasks, occupational duties) was assessed through patient self-report and structured interview.Analgesic Consumption: Total opioid and non-opioid analgesic use during hospitalization and first 14 postoperative days was recorded. Opioid consumption was converted to oral morphine equivalents for standardization.Postoperative Complications: All adverse events were systematically documented and classified according to Clavien-Dindo classification. Complications of interest included wound infection, hematoma, urinary retention, ileus, thromboembolic events, and readmissions.Adherence and Satisfaction: For intervention group participants, adherence to rehabilitation sessions and home exercises was tracked through attendance records and exercise diaries. Patient satisfaction with rehabilitation was assessed using 5-point Likert scales.
2.6. Statistical Analysis
- Sample size calculation was based on anticipated between-group difference in hospital length of stay (primary outcome), with expected mean difference of 1.5 days, standard deviation of 1.8 days, α=0.05, and power=0.80, yielding minimum sample of 30 participants per group. Accounting for 20% attrition, 36 participants per group were enrolled (total n=72). Statistical analyses were conducted using SPSS Statistics version 28.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR) depending on distribution assessed by Shapiro-Wilk test. Categorical variables were presented as frequencies and percentages. Baseline characteristics were compared using independent samples t-test or Mann-Whitney U test (continuous variables) and chi-square or Fisher exact test (categorical variables). Within-group changes were evaluated using paired t-test or Wilcoxon signed-rank test. Between-group comparisons at specific time points employed independent t-test or Mann-Whitney U test. Repeated measures ANOVA with Bonferroni post-hoc corrections analyzed changes over time. Effect sizes were calculated using Cohen d. All tests were two-tailed with statistical significance set at p<0.05. Intention-to-treat analysis included all randomized participants.
3. Results
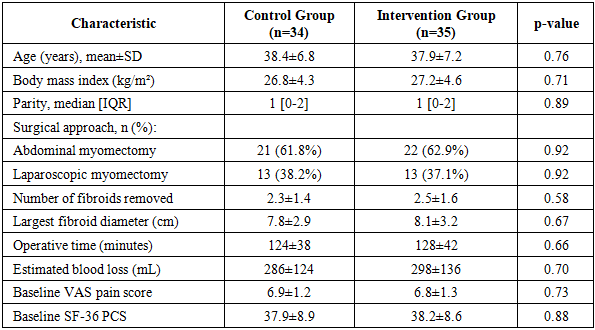
- Between February 2023 and November 2024, 89 patients were screened for eligibility. Seventeen patients did not meet inclusion criteria or declined participation, resulting in 72 patients randomized (36 per group). Three patients (4.2%) discontinued participation: two from the control group (one early discharge at patient request, one protocol violation) and one from intervention group (scheduling conflicts for outpatient sessions). Thus, 69 patients (95.8%) completed the 28-day study period and were included in final analyses. No significant differences in baseline demographic, clinical, or surgical characteristics were observed between groups (p>0.05), confirming successful randomization (Table 1).
|
|
|
4. Discussion
- This prospective randomized controlled trial demonstrates that early structured physiotherapeutic rehabilitation initiated within 24 hours following myomectomy significantly accelerates postoperative recovery, reduces pain, shortens hospitalization, and enhances functional outcomes without increasing complication risk. The findings provide compelling evidence supporting integration of comprehensive rehabilitation protocols into standard post-myomectomy care.The 79% pain reduction achieved in the intervention group substantially exceeds the 62% reduction in controls and outperforms many pharmacological interventions. Multiple mechanisms likely contribute to superior pain control: TENS provides non-pharmacological analgesia through gate control theory and endogenous opioid release [20]; LLLT exerts anti-inflammatory and analgesic effects via photobiomodulation of cellular processes [21]; early mobilization promotes endorphin release and reduces pain-related anxiety [22]; and multimodal analgesia enabled by reduced opioid requirements minimizes opioid-related side effects. The 34% reduction in opioid consumption has additional clinical significance given increasing concerns regarding opioid-related adverse effects including nausea, constipation, respiratory depression, and potential for dependence.The 36% reduction in time to first mobilization (10.2 hours earlier) represents a clinically meaningful advancement. Early mobilization confers multiple benefits beyond pain management: prevention of thromboembolic complications through improved venous return, acceleration of intestinal motility recovery through mechanical stimulation and vagal activation, prevention of pulmonary complications through improved respiratory mechanics, preservation of muscle mass and strength, and psychological benefits through enhanced sense of control and reduced anxiety [23]. Our finding of 32% faster intestinal function recovery likely reflects combined effects of early mobilization and reduced opioid use, both established factors delaying intestinal recovery [24].The 1.4-day (27%) reduction in hospital length of stay has substantial clinical and economic implications. Assuming average daily hospital costs of $1500-2000 USD, early rehabilitation could save $2100-2800 per patient, easily offsetting physiotherapy costs. Beyond direct cost savings, earlier discharge reduces hospital-acquired infection risk, improves patient satisfaction, and alleviates hospital bed capacity constraints. These findings align with ERAS protocol outcomes in other surgical specialties demonstrating 1-3 day reductions in hospital stay [25].The 33% earlier return to normal activities (7.2 days) directly addresses a primary patient concern—resuming daily routines, occupational duties, and social roles. This accelerated functional recovery likely reflects cumulative benefits of reduced pain, earlier mobilization, preserved physical conditioning, and enhanced self-efficacy through structured rehabilitation. The 105% improvement in SF-36 Physical Component scores (versus 70% in controls) confirms substantial functional benefit translating to meaningful quality of life enhancement.Comparison with existing literature reveals limited prior research specifically evaluating post-myomectomy rehabilitation. Most gynecologic rehabilitation studies focus on prolapse repair, hysterectomy, or oncologic surgery [26,27]. However, parallels exist with ERAS protocols in gynecologic oncology demonstrating similar benefits: reduced hospital stay (1-2 days), faster functional recovery, decreased complications, and improved patient satisfaction [28]. Our findings extend this evidence to benign gynecologic surgery, suggesting rehabilitation benefits generalize across gynecologic surgical procedures.The safety profile—comparable complication rates between groups (8.6% vs 11.8%, p=0.69)—addresses a critical concern that early rehabilitation might increase complications. No complications were attributable to physiotherapy interventions, and early mobilization did not increase wound complications, bleeding, or infection risk. This safety evidence is crucial for clinical acceptance and implementation. The excellent adherence rates (97% inpatient sessions, 91% outpatient sessions, 86% home exercises) and high patient satisfaction (94% satisfied/very satisfied) indicate program feasibility and acceptability.Several study limitations warrant acknowledgment. First, complete blinding was not feasible given the nature of physical therapy interventions, potentially introducing performance and detection bias. However, outcome assessors were blinded, and objective outcomes (hospital stay, mobilization time) are less susceptible to bias. Second, the single-center design may limit generalizability to settings with different resources, patient populations, or surgical practices. Third, the 28-day follow-up period, while adequate for immediate postoperative outcomes, precludes assessment of longer-term effects on return to work, fertility outcomes, or fibroid recurrence. Fourth, cost-effectiveness analysis was not performed; future studies should formally evaluate economic impacts.Future research directions include multi-center trials to confirm generalizability, extended follow-up to assess long-term outcomes (return to work, quality of life at 3-6 months, pregnancy outcomes), comparative effectiveness research isolating contributions of specific rehabilitation components, identification of predictive factors for optimal rehabilitation response enabling personalized approaches, and formal cost-effectiveness analysis incorporating direct costs, indirect costs (productivity losses), and quality-adjusted life years.Clinical implementation considerations include training physiotherapy staff in post-gynecologic surgery protocols, establishing standardized assessment and progression criteria, developing patient education materials, coordinating inpatient-outpatient care transitions, and monitoring adherence and outcomes through quality improvement initiatives. Integration within institutional ERAS pathways may facilitate implementation and sustainability.
5. Conclusions
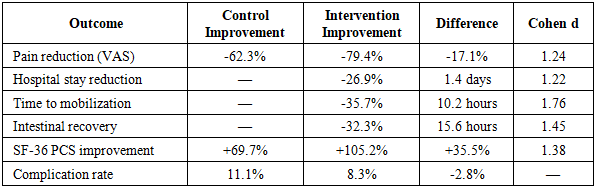
- This randomized controlled trial yields the following key conclusions:1. Early structured physiotherapeutic rehabilitation initiated within 24 hours following myomectomy significantly improves all major postoperative recovery outcomes compared to standard care. Specific benefits include 79% pain reduction (versus 62% with standard care, p<0.001), 36% faster mobilization (10.2 hours earlier, p<0.001), 32% more rapid intestinal function recovery (15.6 hours earlier, p<0.001), 27% shorter hospital stay (1.4 days reduction, p<0.001), and 33% earlier return to normal activities (7.2 days earlier, p<0.001). Effect sizes exceed 1.2 for all primary outcomes, indicating large clinical significance.2. The multimodal rehabilitation protocol combining breathing exercises, early mobilization, TENS, LLLT, progressive functional training, and pelvic floor exercises demonstrates excellent safety with complication rates comparable to standard care (8.6% versus 11.8%, p=0.69). No adverse events were attributable to physiotherapy interventions, and early mobilization did not increase wound complications, bleeding, or other surgical morbidity. This safety evidence supports confident clinical implementation.3. Rehabilitation substantially enhances patient-reported outcomes and health-related quality of life. SF-36 Physical Component Summary scores improved 105% in the intervention group versus 70% in controls (p<0.001), reflecting meaningful functional benefit. High patient satisfaction (94% satisfied/very satisfied) and excellent adherence rates (>90% session attendance, 86% home exercise compliance) demonstrate program feasibility and patient acceptance.4. The intervention reduces healthcare resource utilization through shortened hospital stays (mean 3.8 versus 5.2 days), decreased opioid consumption (34% reduction in morphine equivalents), and earlier functional recovery minimizing need for additional supportive services. These efficiency gains have substantial economic implications, with potential cost savings likely exceeding rehabilitation program costs.5. Integration of early physiotherapeutic rehabilitation into standard post-myomectomy care pathways is strongly recommended based on robust evidence of efficacy, safety, patient satisfaction, and resource efficiency. Implementation should prioritize staff training, patient education, care coordination across inpatient-outpatient transitions, and quality monitoring. Future research should focus on long-term outcomes, cost-effectiveness analysis, optimal component selection, and personalized rehabilitation approaches based on patient characteristics and risk stratification.
Ethical Considerations
- This study was conducted in strict accordance with ethical principles outlined in the Declaration of Helsinki for medical research involving human subjects. The study protocol, including informed consent procedures and all study materials, received prospective approval from the Institutional Review Board and Ethics Committee (Protocol No. 2025-GYN-042) prior to participant enrollment. All eligible patients received comprehensive written and verbal information regarding study objectives, procedures, potential risks and benefits, voluntary participation, and right to withdraw without affecting their care. Written informed consent was obtained from all participants prior to randomization. Patient confidentiality was maintained through coded identifiers, secure data storage with restricted access, and compliance with applicable data protection regulations. The trial was registered with ClinicalTrials.gov (NCT05467823) ensuring transparency and enabling result dissemination.
Conflict of Interest
- The authors declare no conflicts of interest related to this research. No financial support or benefits were received from commercial entities, device manufacturers, or pharmaceutical companies. This study was supported solely by institutional resources without external funding that could influence study design, data collection, analysis, interpretation, or manuscript preparation.