-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1876-1881
doi:10.5923/j.ajmms.20261604.67
Received: Mar. 18, 2026; Accepted: Apr. 7, 2026; Published: Apr. 15, 2026

Nerve Growth Factor (NGF) Levels in Generalized Epilepsy and Their Association with Cognitive Impairment and Affective Symptoms
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRa’nogul H. Fayziyeva, Ra’no B. Azizova
Department of Neurology and Medical Psychology, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Ra’nogul H. Fayziyeva, Department of Neurology and Medical Psychology, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Epilepsy is a chronic neurological disorder often accompanied by cognitive impairment and affective disturbances in addition to recurrent seizures. Neurotrophic factors, particularly nerve growth factor (NGF), play an important role in neuronal plasticity and cognitive functioning, but their role in generalized epilepsy remains insufficiently studied. The aim of this study was to evaluate plasma NGF levels and their association with cognitive impairment and depressive symptoms in patients with generalized epilepsy. A total of 83 patients with epilepsy and 15 healthy controls were examined. Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA), affective symptoms using the Hospital Anxiety and Depression Scale (HADS), and plasma NGF levels were measured by ELISA. Cognitive decline was associated with longer disease duration (p = 0.023) and higher seizure frequency (p = 0.002). NGF levels decreased with increasing disease duration (p < 0.001) and showed a positive correlation with cognitive performance (p = 0.007), but were not significantly associated with anxiety or depression scores. Reduced NGF levels may reflect impaired neurotrophic support and could be related to cognitive dysfunction in generalized epilepsy.
Keywords: Generalized epilepsy, Cognitive impairment, Depression, Nerve growth factor (NGF), Neurotrophic factors, MoCA, HADS, Seizure frequency
Cite this paper: Ra’nogul H. Fayziyeva, Ra’no B. Azizova, Nerve Growth Factor (NGF) Levels in Generalized Epilepsy and Their Association with Cognitive Impairment and Affective Symptoms, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1876-1881. doi: 10.5923/j.ajmms.20261604.67.
Article Outline
1. Introduction
- Epilepsy is a chronic neurological disorder characterized by recurrent epileptic seizures, which represent its main clinical manifestation. Epileptic seizures arise from abnormal, excessive, or synchronous electrical activity of neuronal networks in the brain and may present as transient motor, sensory, autonomic, cognitive, or consciousness disturbances [2]. In modern epileptology, epilepsy is no longer considered a condition limited to seizures alone, but rather a complex clinical-neurobiological syndrome characterized by a persistent predisposition to generate epileptic seizures [3].Clinically, epileptic seizures are highly heterogeneous and may manifest as brief impairment of consciousness (absence seizures), myoclonic phenomena, focal motor or sensory symptoms, or generalized tonic–clonic convulsions involving the entire body [4]. Importantly, the clinical consequences of epilepsy are not restricted to seizures. The disorder is frequently associated with cognitive impairment, affective disturbances (anxiety and depression), difficulties in social adaptation, and reduced quality of life [5].The pathogenesis of cognitive and affective disturbances in epilepsy involves dysfunction of frontal–thalamo–cortical networks, imbalance between GABAergic and glutamatergic neurotransmission, neuroinflammatory processes, and alterations in neurotrophic factors [8]. In particular, changes in the levels of nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF) have been shown to influence synaptic plasticity, neuronal survival, and emotional regulation [1,6]. Decreased NGF levels observed in both depression and epilepsy suggest the presence of shared pathophysiological mechanisms underlying these conditions [7,9].In generalized epilepsy, cognitive and affective disorders are often underestimated in routine clinical practice. However, early detection and regular monitoring of these disturbances are essential for improving quality of life, enhancing treatment adherence, and optimizing disease prognosis. Therefore, the use of validated screening tools such as the Montreal Cognitive Assessment (MoCA) and the Hospital Anxiety and Depression Scale (HADS) should be considered an integral part of the comprehensive evaluation of patients with generalized epilepsy [10,11]. MoCA and HADS scales provide convenient and reliable instruments for the complex assessment of cognitive and affective disturbances in patients with generalized epilepsy.Therefore, the aim of this study was to investigate plasma NGF levels and their association with cognitive impairment and affective symptoms in patients with generalized epilepsy.
2. Material and Methods
- Patients for the study were selected from the clinical base of the Tashkent City Clinical Hospital No. 7, and laboratory investigations were performed at the scientific laboratory of the Tashkent State Medical University. The study was conducted between 2024 and 2025.A total of 83 patients with epilepsy were included in the study. Diagnosis of epilepsy was confirmed based on clinical evaluation and electroencephalography (EEG) findings according to ILAE recommendations. According to seizure type, the main group consisted of 46 patients with generalized epilepsy (GE), including 7 patients with juvenile absence epilepsy (YAE), 12 patients with juvenile myoclonic epilepsy (JME), and 27 patients with generalized tonic-clonic seizures (GTCS). The comparison group included 37 patients with focal structural epilepsy (FE). The control group consisted of 15 age-matched healthy volunteers (e.g. Figure 2.1).
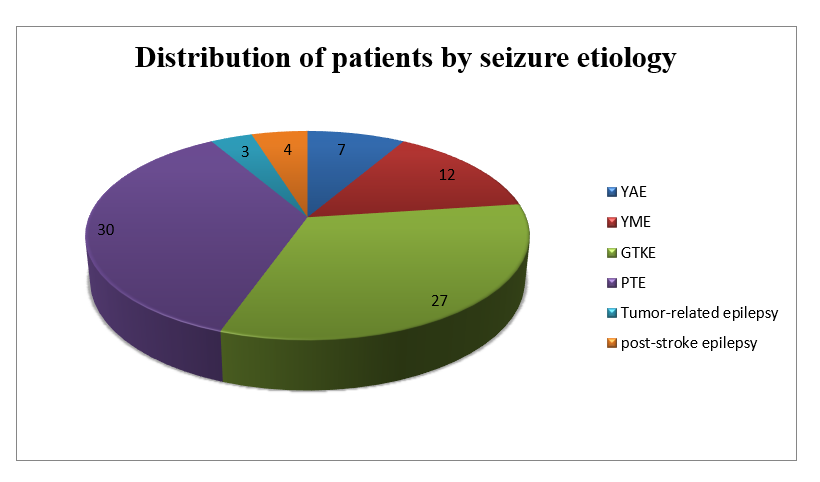 | Figure 2.1. Distribution of patients by seizure etiology |
2.1. Inclusion Criteria
- Patients were included in the study according to the following criteria:• Age ≥ 18 years• Diagnosis of epilepsy confirmed according to ILAE criteria• Presence of generalized tonic-clonic seizures• Duration of epilepsy ≥ 1 year• Blood samples obtained in the postictal period (at least 3 days after the last seizure)• Written informed consent obtained from the patient
2.2. Exclusion Criteria
- Patients were excluded from the study if any of the following conditions were present:• Patients with severe depression were excluded based on HADS-D scores ≥11, in accordance with standard interpretation guidelines.• Pregnancy or breastfeeding• Epilepsy caused by infectious or autoimmune diseases of the central nervous system• Recent use of immunomodulators, glucocorticoids, or other therapies that may affect neurotrophic factor levelsAll patients underwent a standard neurological examination. Cognitive functions were evaluated using the Montreal Cognitive Assessment (MoCA), which assesses attention, executive functions, memory, language, abstract reasoning, visuospatial abilities, and orientation.anxiety and depressive symptoms were assessed using the Hospital Anxiety and Depression Scale (HADS). Blood samples were obtained at least 3 days after the last seizure. Plasma was separated and nerve growth factor (NGF) levels were determined using an enzyme-linked immunosorbent assay (ELISA).The mean age of patients was 35.93 ± 11.67 years in the generalized epilepsy group, 42.24 ± 11.79 years in the comparison group, and 37.53 ± 12.25 years in the control group. A total of 51 patients (61.44%) were male and 32 (38.55%) were female.
3. Results
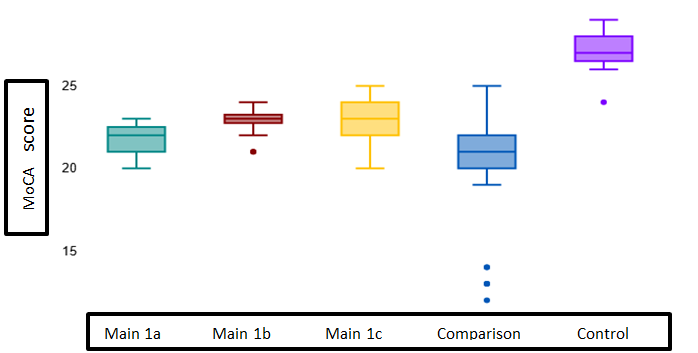
- In this study, cognitive function in patients with generalized epilepsy was assessed comprehensively. Cognitive impairment was detected in the majority of participants. Mild cognitive impairment was observed in 78 patients (79.5%), normal cognitive function in 14 patients (14.3%), and moderate cognitive impairment in 6 patients (6.2%). These findings suggest that long disease duration and recurrent seizures may be associated with neurofunctional changes.According to MoCA scores, ≥26 points were considered normal, 18–25 points as mild cognitive impairment, and ≤17 points as moderate cognitive impairment. Figure 3.1 shows the distribution of MoCA scores at baseline in the main (1a–1c), comparison, and control groups, presented as a box plot.
 | Figure 3.1. Distribution of MoCA scores in the main, comparison, and control groups |
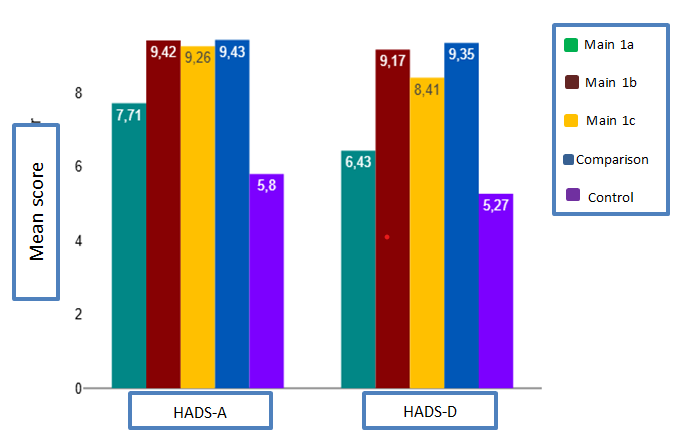 | Figure 3.2. HADS-A and HADS-D scores in the main, comparison, and control groups |
|
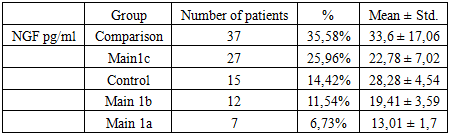
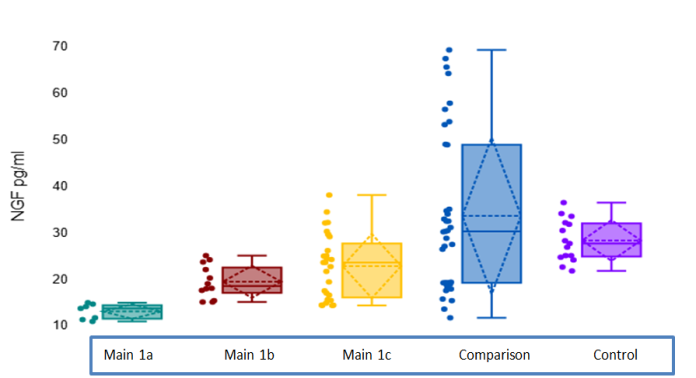 | Figure 3.3. Plasma NGF levels (pg/ml) across study groups. Error bars represent standard deviation |
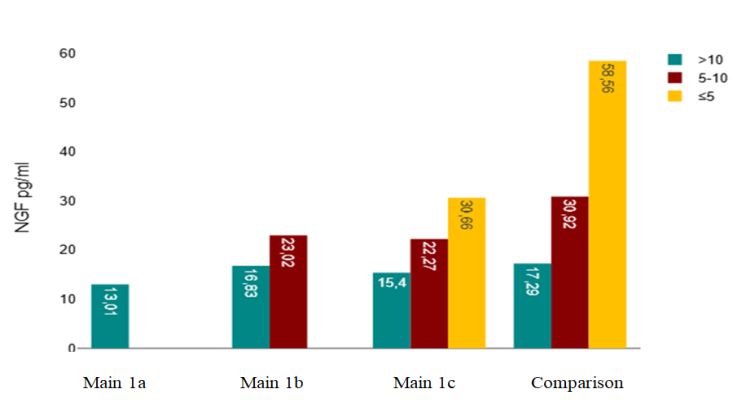 | Figure 3.4. Changes in NGF levels according to disease duration in the study groups |
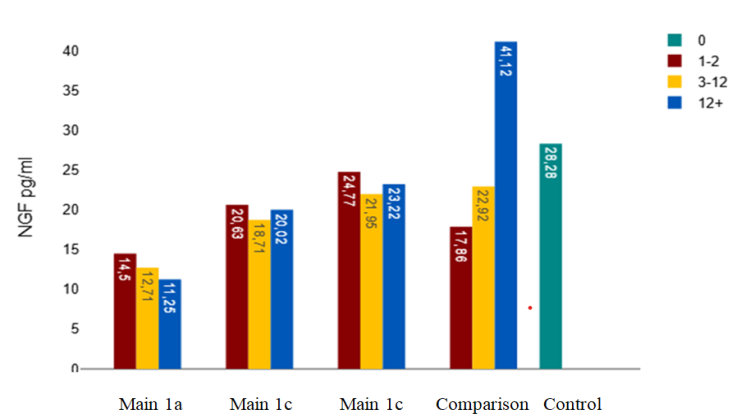 | Figure 3.5. Changes in plasma NGF levels according to annual seizure frequency in the study groups |
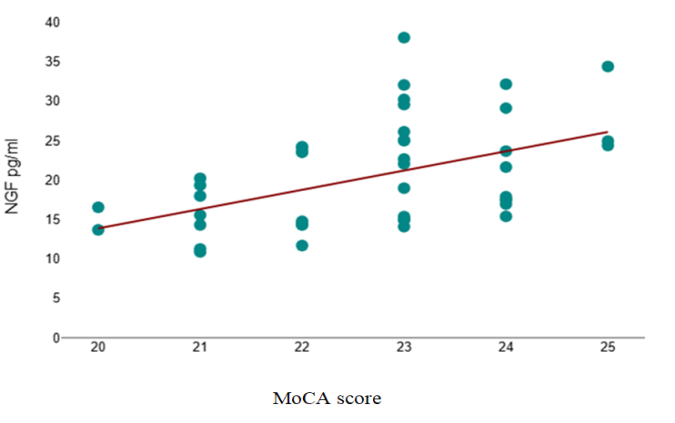 | Figure 3.6. Relationship between plasma NGF level and MoCA score in the main group |
4. Discussion
- In this study, the relationship between cognitive function, affective status, and plasma nerve growth factor (NGF) levels was evaluated in patients with generalized epilepsy. The results showed that certain clinical characteristics of epilepsy, particularly disease duration and seizure frequency, were associated with cognitive decline. In the main group, longer disease duration was associated with lower cognitive performance. The negative correlation between MoCA scores and disease duration suggests that long-standing epilepsy may lead to progressive functional changes in the central nervous system. In addition, the negative association between seizure frequency and cognitive function indicates that recurrent epileptic activity may contribute to a reduction in cognitive reserve. These findings are consistent with previous studies reporting that repeated epileptic discharges and neuronal network reorganization may play an important role in the development of cognitive impairment. In this study, the relationship between cognitive function, affective status, and plasma nerve growth factor (NGF) levels was evaluated in patients with generalized epilepsy. The results showed that certain clinical characteristics of epilepsy, particularly disease duration and seizure frequency, were associated with cognitive decline. In the main group, longer disease duration was associated with lower cognitive performance. The negative correlation between MoCA scores and disease duration suggests that long-standing epilepsy may lead to progressive functional changes in the central nervous system. In addition, the negative association between seizure frequency and cognitive function indicates that recurrent epileptic activity may contribute to a reduction in cognitive reserve. These findings are consistent with previous studies reporting that repeated epileptic discharges and neuronal network reorganization may play an important role in the development of cognitive impairment. Analysis of psychoemotional status demonstrated higher levels of anxiety and depression in patients with epilepsy compared with the control group. However, no significant correlations were found between HADS scores and clinical parameters such as disease duration or seizure frequency, suggesting that affective disturbances may also be influenced by psychosocial factors and individual adaptive mechanisms.An important part of the study was the evaluation of plasma NGF levels in different groups. The results showed a tendency toward decreased NGF levels with longer disease duration. Neurotrophic factors, including NGF, play a key role in neuronal survival, synaptic plasticity, and maintenance of neural connections; therefore, reduced NGF levels may reflect weakening of neurotrophic mechanisms during chronic epileptic activity.A moderate positive correlation between NGF level and cognitive performance in the main group suggests that NGF may act as a biological factor supporting cognitive function. Higher NGF levels were associated with better cognitive scores, which may reflect the role of neurotrophic factors in maintaining neuronal plasticity. In contrast, no statistically significant relationship was found between NGF level and affective symptoms.These findings are consistent with previous studies demonstrating the role of neurotrophic factors in epilepsy and cognitive impairment (Iughetti et al., 2018). Previous studies have mainly focused on BDNF as a key neurotrophic factor in epilepsy (Iughetti et al., 2018). However, the role of NGF remains insufficiently studied. Our results suggest that NGF may also contribute to cognitive impairment in generalized epilepsy.This study has several limitations, including a relatively small sample size and single-time measurement of NGF levels. In addition, the potential effect of antiepileptic drugs on NGF concentration was not analyzed separately. Nevertheless, the findings suggest that NGF may be a biological factor associated with cognitive impairment in generalized epilepsy and indicate the need for further research in this area.
5. Conclusions
- In the main group, a statistically significant negative correlation was found between disease duration and cognitive performance (p = 0.023), and a moderate negative correlation was observed between seizure frequency and MoCA scores (p = 0.002), while no significant associations between these variables were detected in the comparison group. Analysis of psychoemotional status showed that anxiety levels were highest in subgroup comparison 2b and lowest in subgroup main 1a, whereas depressive symptoms were subclinically higher in subgroup comparison 2a. However, no statistically significant correlations were found between HADS-A or HADS-D scores and disease duration or seizure frequency. Plasma NGF levels were higher in the comparison group and demonstrated a strong negative correlation with disease duration (p < 0.001), while the relationship between NGF level and seizure frequency was non-linear. In the main group, a moderate positive and statistically significant correlation was found between NGF level and cognitive performance (p = 0.007), whereas correlations between NGF level and anxiety or depression scores were weak and not statistically significant.