-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1870-1875
doi:10.5923/j.ajmms.20261604.66
Received: Mar. 16, 2026; Accepted: Apr. 12, 2026; Published: Apr. 15, 2026

Immunopathogenetic Significance of Inflammatory Markers and Innate, B-Cell, and Humoral Immunity Parameters in Early Childhood Community-Acquired Pneumonia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNodira Khoshimovna Abrieva1, Alisher Mirkhamidovich Sharipov2, Akhmataliyeva Mayram3, Rakhimova Suray Ruzimetovna4, Zafar Fayzullaevich Safarov5
1Assistant, Department of Emergency Medicine and Disaster Medicine, Tashkent State Medical University, Uzbekistan
2Doctor of Medical Sciences, Professor, Head of the Department of Emergency Medicine and Disaster Medicine, Tashkent State Medical University, Uzbekistan
3Associate Professor, Department of Emergency Medicine and Disaster Medicine, Tashkent State Medical University, Uzbekistan
4Assistant, Republican Research Center of Emergency Medicine, Tashkent, Uzbekistan, Uzbekistan
5PhD, Associate Professor, Department of Emergency Medicine and Disaster Medicine, Tashkent State Medical University
Correspondence to: Nodira Khoshimovna Abrieva, Assistant, Department of Emergency Medicine and Disaster Medicine, Tashkent State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective. To evaluate the diagnostic and prognostic significance of inflammatory markers and innate immunity parameters in combination with B-cell and humoral immune response indicators in children with different severities of community-acquired pneumonia (CAP). Materials and Methods. This prospective single-center study included 80 children aged 1 month to 3 years with clinically and radiologically confirmed community-acquired pneumonia. Patients were stratified into mild (n=40) and severe (n=40) disease groups. Systemic inflammatory markers (leukocyte count, procalcitonin, C-reactive protein), innate immunity parameters (CD64 and CD16 expression, neutrophil phagocytic activity), as well as adaptive and humoral immune indicators (lymphocyte count, CD19, IgA, IgM, and IgG levels) were assessed. Statistical analysis included estimation of effect size using Cohen’s d. Results. Severe CAP was characterized by leukocytosis, lymphopenia, elevated procalcitonin and C-reactive protein levels, and pronounced activation of innate immunity, reflected by a significant increase in CD64 expression and neutrophil phagocytic activity (p<0.001). CD19 demonstrated moderate intergroup differences, indicating secondary involvement of the B-cell immune compartment. Serum immunoglobulin concentrations (IgA, IgM, and IgG) did not show statistically significant differences between groups. CD16 lacked independent diagnostic value. Conclusion. Severe community-acquired pneumonia in early childhood is associated with the development of an immunophenotype characterized by predominant innate immune activation accompanied by functional impairment of adaptive and humoral immune responses. A comprehensive assessment of inflammatory and innate immune markers, including CD64, improves early risk stratification and may support optimized clinical management.
Keywords: Community-acquired pneumonia, Early childhood, Innate immunity, B-cell immunity, Humoral immunity, Inflammatory markers, CD64, CD19, Immune phenotype
Cite this paper: Nodira Khoshimovna Abrieva, Alisher Mirkhamidovich Sharipov, Akhmataliyeva Mayram, Rakhimova Suray Ruzimetovna, Zafar Fayzullaevich Safarov, Immunopathogenetic Significance of Inflammatory Markers and Innate, B-Cell, and Humoral Immunity Parameters in Early Childhood Community-Acquired Pneumonia, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1870-1875. doi: 10.5923/j.ajmms.20261604.66.
1. Introduction
- Community-acquired pneumonia (CAP) is one of the most common respiratory tract infections in children and represents a significant challenge for modern pediatrics. CAP is defined as an acute inflammatory disease of the lungs that develops outside the hospital setting or is diagnosed within the first 48 hours after hospitalization, or not earlier than four weeks after discharge [1].CAP remains one of the leading causes of morbidity and mortality in early childhood. The incidence is approximately 15–20 cases per 1,000 children under three years of age and 5–6 cases per 1,000 children at older ages [2]. According to the World Health Organization, pneumonia is one of the major causes of childhood mortality, accounting for 17.5% of all deaths in children under five years old (approximately 1.1 million cases annually), with up to 99% of deaths occurring in low- and middle-income countries [3]. Worldwide, around 156 million cases of pneumonia in children are recorded annually, of which up to 2 million result in death [1].Assessment of risk and prediction of treatment outcomes in children with CAP is of great practical importance, especially in early childhood, which is characterized by functional immaturity of the immune system. The pathogenesis of CAP is largely driven by innate immune mechanisms that provide the primary anti-infective response, as well as their interaction with adaptive and humoral components of the immune system. An imbalance between activation of innate immune responses and the functional capacity of the adaptive immune response may determine the severity of the disease and the likelihood of unfavorable outcomes.Immunological biomarkers—such as systemic inflammatory markers, cellular subpopulations, and humoral immunity parameters—allow for an objective assessment of immune response characteristics and disease severity. Classical inflammatory markers, including leukocyte count, lymphocyte count, procalcitonin, and C-reactive protein, are widely used in clinical practice for the initial evaluation of infectious activity [5,6]. At the same time, innate immunity markers such as CD64⁺ expression and neutrophil phagocytic activity are considered more sensitive indicators of severe bacterial inflammation and systemic immune activation [7].In addition, adaptive and humoral immunity indicators—including B‑cell parameters (CD19⁺) and serum immunoglobulin levels (IgA, IgM, IgG)—reflect the involvement of specific immune mechanisms in the anti‑infective response. Analysis of these indicators allows for a more comprehensive characterization of the immune profile and identification of immunoregulatory features associated with severe CAP [4]. A combined assessment of inflammatory markers and parameters of innate, adaptive, and humoral immunity may serve as the basis for early risk stratification, optimization of monitoring, and justification of management strategies for children with community-acquired pneumonia.Objective. To evaluate the diagnostic and prognostic significance of inflammatory markers and innate immunity parameters, in combination with indicators of B‑cell and humoral immune responses, in children with different severities of community‑acquired pneumonia (CAP).
2. Materials and Methods
- This study was conducted as a single-center prospective observational investigation, in which children with community-acquired pneumonia (CAP) hospitalized at the Republican Scientific Center for Emergency Medical Care from September 2024 to May 2025 were consecutively enrolled. A total of 80 children aged 1 month to 3 years with clinically and radiologically confirmed CAP were included. Depending on disease severity, patients were divided into two groups: 40 children with mild CAP and 40 children with severe CAP.Inclusion criteria required the presence of clinical and radiological signs of community-acquired pneumonia, age under 3 years, and hospitalization within the first 24 hours from disease onset. Exclusion criteria included primary and secondary immunodeficiency disorders, long-term immunosuppressive therapy, severe chronic diseases of the cardiopulmonary, hepatic, renal, or nervous systems, hospital-acquired pneumonia, a history of severe infection or hospitalization within the previous four weeks, absence of informed consent, or incomplete clinical and laboratory data. Hospital-acquired pneumonia was excluded if clinical and radiological signs of lung inflammation appeared ≥48 hours after hospitalization in the absence of respiratory symptoms and infiltrative changes on the initial chest radiograph.Venous blood samples were collected on the first day of hospitalization, before initiation or in the early phase of antibiotic therapy. All patients underwent a complete blood count with measurement of leukocyte count and absolute and relative lymphocyte numbers. Procalcitonin and C-reactive protein levels in plasma were assessed as systemic inflammatory markers.Immunological evaluation included assessment of innate, adaptive, and humoral immunity parameters. Innate immune response was characterized by determining neutrophil CD64+ and CD16+ expression, as well as neutrophil phagocytic activity. Adaptive immunity was assessed by quantitative evaluation of the B-cell subset through measurement of CD19+ levels. Humoral immunity was evaluated by measuring serum concentrations of immunoglobulins IgA, IgM, and IgG.Statistical analysis was performed using descriptive and inferential statistical methods. The normality of data distribution was assessed using the Shapiro–Wilk test, and homogeneity of variances was evaluated using the F-test. Quantitative variables were compared between groups using Student’s t-test for normally distributed data with equal variances and Welch’s t-test when variances were unequal. For non-normally distributed data, the Mann–Whitney U test was applied. The magnitude of intergroup differences was assessed using Cohen’s d effect size. A p-value <0.05 was considered statistically significant.
3. Results
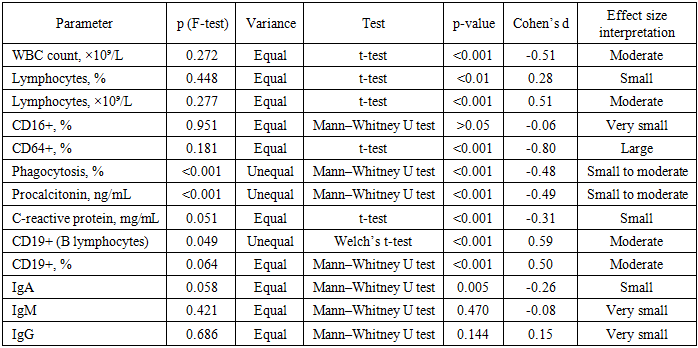
- The most pronounced differences between the groups were observed in the white blood cell (WBC) count. The t-test revealed a highly statistically significant difference (p<0.001), with an effect size of d = –0.51, indicating a moderate effect. Increased WBC counts in children with severe community-acquired pneumonia (CAP) reflect activation of the systemic inflammatory response and suggest the development of a pronounced innate immune cascade directed toward elimination of the infectious agent. In this setting, leukocytosis should be regarded not only as a marker of inflammation, but also as an indicator of generalized immune activation associated with a more severe clinical course of the disease (Table 1).The lymphocyte-related parameters also showed statistically significant differences. The t-test demonstrated a significant decrease in both the relative lymphocyte count (p<0.01; d = 0.28) and the absolute lymphocyte count (p<0.001; d = 0.51) in children with severe CAP (Table 1). The presence of lymphopenia in severe disease reflects suppression of the adaptive immune response, which is characteristic of systemic inflammatory reactions and is associated with functional impairment of both the T-cell and B-cell compartments of immunity. This phenomenon may be related to lymphocyte redistribution to the site of inflammation, apoptosis of immune cells induced by proinflammatory cytokines, and exhaustion of immunoregulatory mechanisms, thereby contributing to the development of an immunodeficiency-like state in the context of a hyperinflammatory response.
|
4. Discussion
- The present findings confirm the high diagnostic and prognostic value of a comprehensive assessment of inflammatory markers and innate immunity parameters in community-acquired pneumonia (CAP) in young children. The observed changes reflect activation of the systemic inflammatory response and innate immune mechanisms in the setting of relative suppression of the adaptive immune compartment, which is generally consistent with current concepts regarding the pathogenesis of severe pediatric CAP described in clinical guidelines and epidemiological studies [1–3].The elevated white blood cell (WBC) count observed in children with severe CAP in the present study is consistent with the findings of the retrospective observational study by Cao et al., in which marked leukocytosis was associated with respiratory failure, the need for intensive care, and an unfavorable prognosis in patients with severe community-acquired pneumonia [2]. Similar conclusions are also reflected in the clinical guidelines of the Union of Pediatricians of Russia, which emphasize the importance of complete blood count parameters as accessible and informative tools for the initial assessment of disease severity [1].The lymphopenia identified in our study among patients with severe CAP is also consistent with clinical and pathophysiological studies showing that a reduced absolute lymphocyte count reflects impairment of the adaptive immune response and is associated with a more severe course of infectious and inflammatory processes in young children [2,9,12]. From a pathogenetic perspective, lymphopenia may result from redistribution of lymphocytes to the inflammatory focus, apoptosis of immune cells induced by proinflammatory cytokines, and exhaustion of immunoregulatory mechanisms, leading to a state of functional immune insufficiency in the context of a hyperinflammatory response.Classical inflammatory biomarkers, namely procalcitonin and C-reactive protein (CRP), also demonstrated a significant association with severe CAP in the present study. In the study by Cao et al., elevated procalcitonin was identified as an independent predictor of severe disease and adverse outcome in children with pneumonia [2]. Similar findings have also been reported in domestic studies evaluating the diagnostic value of procalcitonin in hospitalized children with CAP [10]. At the same time, several studies have emphasized the limitations of using procalcitonin and CRP in isolation, which supports the rationale for their combined assessment with immunological markers reflecting activation of innate immunity [11].The most pronounced between-group differences in the present study were observed for CD64+ expression, which is in line with current evidence supporting its role as a highly sensitive marker of innate immune activation in bacterial infections. In the study by Abdelmohsen and Allam, neutrophil CD64 expression in children with CAP was significantly higher than in the control group and correlated with clinical disease severity and CRP levels [7]. Similar findings have been reported in other studies confirming the diagnostic value of CD64 specifically in the pediatric population with pneumonia [8]. According to the meta-analysis by Shang et al., the CD64 index is comparable to, and in some settings superior to, traditional inflammatory markers in terms of sensitivity and specificity in severe infections, further underscoring its prognostic potential [9].The increased neutrophil phagocytic activity observed in children with severe CAP reflects activation of the innate immune response under conditions of high microbial burden. Similar changes have been described in studies focusing on Fc receptors and mechanisms of neutrophil activation in severe infectious and inflammatory diseases in children, where enhanced phagocytosis is regarded as a compensatory mechanism aimed at pathogen elimination, but one that may simultaneously contribute to persistence of the inflammatory cascade and tissue injury [11,12].Unlike the other investigated parameters, CD16+ did not reach statistical significance in our study. This finding is consistent with published data indicating high age-related and interindividual variability in CD16 expression in young children, as well as its limited independent prognostic value compared with CD64 in assessing the severity of infectious and inflammatory conditions [9,11].The integrated analysis of inflammatory markers and parameters of innate, adaptive, and humoral immunity allowed us to formulate an integrative model of the immune phenotype associated with severe CAP in young children. This phenotype is characterized by predominance of innate immune mechanisms against a background of relative functional insufficiency of the adaptive and humoral immune compartments (Figure 1).
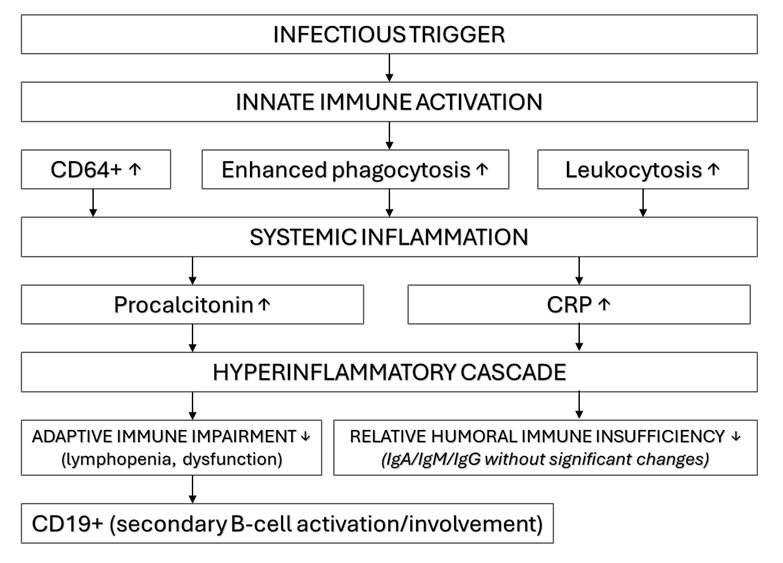 | Figure 1. Proposed immunopathogenetic model of severe community-acquired pneumonia in young children. The model illustrates the predominance of innate immune activation, characterized by activation of the neutrophil–monocyte compartment (CD64+, enhanced phagocytosis, and leukocytosis) and the development of a systemic inflammatory response (procalcitonin and C-reactive protein), in the setting of adaptive immune impairment (lymphopenia) and relative functional immaturity of the humoral immune compartment (IgA, IgM, and IgG), with secondary involvement of the B-cell component (CD19+) |
5. Conclusions
- Severe community-acquired pneumonia (CAP) in young children is characterized by an immune phenotype of innate immune predominance, developing in the setting of relative functional impairment of the adaptive and humoral immune compartments. The most informative diagnostic and prognostic markers were those reflecting systemic inflammation and innate immune activation, including leukocytosis, lymphopenia, elevated procalcitonin and C-reactive protein levels, and marked activation of the neutrophil–monocyte compartment, as evidenced by increased CD64+ expression and enhanced neutrophil phagocytic activity. Moderate alterations in CD19+ support secondary involvement of the B-cell compartment, whereas the absence of statistically significant differences in IgA, IgM, and IgG levels suggests relative functional immaturity of the humoral immune response in early childhood. A combined assessment of inflammatory markers and innate immunity parameters, particularly CD64+, may improve early identification of children at risk for severe CAP and support more precise risk stratification and clinical decision-making in this vulnerable age group.