-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1858-1862
doi:10.5923/j.ajmms.20261604.63
Received: Mar. 10, 2026; Accepted: Mar. 28, 2026; Published: Apr. 15, 2026

Antibiotic Resistance of Nosocomial Infections in Newborns and Older Children on Prolonged Mechanical Ventilation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJakhongir Inomjon ugli Mukhtorov, Elmira Abdusamatovna Satvaldiyeva, Nazifa Abduraufovna Umarova
National Children’s Medical Center, Tashkent, Republic of Uzbekistan
Correspondence to: Jakhongir Inomjon ugli Mukhtorov, National Children’s Medical Center, Tashkent, Republic of Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Nosocomial infections remain a major cause of morbidity and mortality in pediatric intensive care units (PICUs), particularly among children requiring prolonged mechanical ventilation. This prospective observational cohort study evaluated the spectrum of pathogens, the dynamics of respiratory tract colonization, and antibiotic resistance patterns in tracheal aspirates obtained from mechanically ventilated children treated in an intensive care unit from 2023 to 2025. A total of 159 tracheal aspirate samples from 48 patients were analyzed using conventional susceptibility testing, automated identification systems (Vitek 2, MALDI-TOF mass spectrometry), carbapenem minimum inhibitory concentration (MIC) determination, and phenotypic and molecular detection of carbapenem resistance mechanisms. The tracheal aspirate microbiota yielded 327 isolates from 27 microbial species. Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Staphylococcus aureus predominated. Carbapenem resistance was especially pronounced among P. aeruginosa (61.8% meropenem resistance) and A. baumannii (79.4% meropenem resistance), whereas colistin retained activity against all tested isolates. Colonization with multidrug-resistant (MDR) Gram-negative pathogens developed rapidly, appearing by days 4–6 in primarily admitted patients and already present at admission in transferred patients. These findings support individualized, microbiology-guided antibiotic therapy over empirical broad-spectrum treatment and underscore the critical role of local microbiological surveillance in pediatric intensive care.
Keywords: Nosocomial infection, Pediatric intensive care unit, Mechanical ventilation, Antibiotic resistance, Carbapenem resistance, Tracheal aspirate, Multidrug-resistant organisms, Antimicrobial stewardship
Cite this paper: Jakhongir Inomjon ugli Mukhtorov, Elmira Abdusamatovna Satvaldiyeva, Nazifa Abduraufovna Umarova, Antibiotic Resistance of Nosocomial Infections in Newborns and Older Children on Prolonged Mechanical Ventilation, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1858-1862. doi: 10.5923/j.ajmms.20261604.63.
Article Outline
1. Introduction
- In the era of increasing antimicrobial resistance, nosocomial infections in intensive care units (ICUs) have become one of the most pressing challenges in modern clinical medicine. ICU patients are exposed to invasive procedures, broad-spectrum antibiotics, prolonged hospitalization, and severe underlying illness, all of which substantially elevate the risk of hospital-acquired infection [1–3]. The global burden of antimicrobial resistance continues to rise, with the World Health Organization estimating that by 2050 drug-resistant infections could cause up to 10 million deaths annually if not addressed [23].This risk is particularly pronounced in children receiving prolonged mechanical ventilation. Ventilator-associated lower respiratory tract infections, including ventilator-associated pneumonia (VAP), are among the most frequent and most dangerous complications in PICUs, associated with prolonged hospitalization, increased costs, and high mortality rates of 20–50% [4,5]. In pediatric patients, therapeutic options are further constrained by age-related restrictions on several antimicrobial classes, making pathogen-specific therapy even more essential [24,25].Gram-negative microorganisms predominate in many ICU settings and increasingly exhibit multidrug resistance (MDR), including resistance mediated by extended-spectrum beta-lactamases (ESBLs) and carbapenemases [6,7]. Carbapenem-resistant Enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aeruginosa (ESKAPE pathogens) are now recognized as priority pathogens by the WHO [26]. Data from Central Asian and Eastern European ICUs suggest that resistance rates in this region may exceed those reported in Western Europe, highlighting the importance of region-specific surveillance [27].Under these conditions, local microbiological surveillance is essential for rational antibiotic stewardship. Determining the current spectrum of pathogens and their resistance mechanisms is necessary both for appropriate treatment selection and for effective infection-control planning. This study provides updated surveillance data through 2025, capturing the post-pandemic microbiological landscape in a pediatric tertiary-care ICU in Uzbekistan.
2. Aim of the Study
- The aim of this study was to determine the spectrum, colonization dynamics, and antibiotic resistance patterns—including the principal carbapenem resistance mechanisms—in tracheal aspirate microbiota of children receiving prolonged mechanical ventilation in a pediatric intensive care unit.
3. Materials and Methods
3.1. Study Design
- This was a prospective observational cohort study conducted at the National Children’s Medical Center (NCMC), Tashkent, Uzbekistan, from January 2023 to December 2025. The study was approved by the institutional ethics committee and conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from the legal guardians of all participating patients.
3.2. Inclusion and Exclusion Criteria
- Patients were eligible for inclusion if they: (1) were admitted to the NCMC PICU; (2) required invasive mechanical ventilation for ≥7 days; and (3) had at least one tracheal aspirate culture obtained during the observation period. Patients were excluded if they: (1) had a previously confirmed active respiratory infection at PICU admission that was being treated with targeted antibiotic therapy; (2) received mechanical ventilation for fewer than 3 days; or (3) had incomplete microbiological records. A total of 48 patients met the inclusion criteria.
3.3. Sample Size Justification
- Based on the expected prevalence of carbapenem-resistant Gram-negative organisms of approximately 40–60% in comparable ICU settings [8,9], a sample of 48 patients provided sufficient precision to estimate resistance frequencies with a 95% confidence interval width of ±15%. Although this sample size limits the power of subgroup analyses, it is representative of the single-center PICU capacity over the study period and is consistent with comparable microbiological surveillance studies in pediatric critical care [28].
3.4. Observation Stages and Sampling
- Tracheal aspirate samples were collected prospectively at three predefined time points: Stage I (days 1–3 after PICU admission), Stage II (days 4–6), and Stage III (days 7–9). The three-stage protocol was designed to capture the temporal dynamics of respiratory colonization, distinguishing community-acquired or inter-hospital flora (Stage I) from early and late ICU-acquired organisms (Stages II–III). The underlying diagnoses of enrolled patients included brain tumors (n = 24), metabolic coma (n = 12), and viral encephalomyelitis (n = 12).
3.5. Definitions
- Colonization was defined as the recovery of a microorganism from a tracheal aspirate without clinical or radiological signs of infection. Infection (VAP) was defined according to the CDC/NHSN criteria: new or progressive radiological infiltrate plus at least two of the following: fever (>38.0°C) or hypothermia (<36.0°C), leukocytosis (>12×10⁹/L) or leukopenia (<4×10⁹/L), and purulent tracheal secretions. Multidrug resistance (MDR) was defined as non-susceptibility to at least one agent in three or more antimicrobial categories according to the Magiorakos et al. (2012) consensus criteria [29].
3.6. Microbiological Methods
- Microorganisms were identified using the Vitek 2 Compact analyzer (bioMérieux, France) and MALDI-TOF mass spectrometry (Microflex, Bruker Daltonics, Germany). Antibiotic susceptibility was assessed using the Vitek 2 Compact system and the disk-diffusion method on Mueller-Hinton agar. MICs for meropenem and imipenem were determined using E-tests. Results were interpreted according to EUCAST 2023 breakpoints.Metallo-beta-lactamase (MBL) production was evaluated using the double-disk synergy method. Carbapenemase production in K. pneumoniae isolates was assessed using the modified Hodge test. Genes encoding carbapenem resistance (blaKPC, blaOXA-48, blaNDM, blaVIM, blaIMP) were detected by real-time PCR using a CFX 1000 amplifier (Bio-Rad, USA) with commercial test systems. To characterize carbapenemase types, 65 carbapenem-resistant Gram-negative isolates collected between 2021 and 2024 were additionally studied, comprising 20 P. aeruginosa, 14 K. pneumoniae, and 31 A. baumannii isolates recovered from tracheal aspirates, CSF, blood, and other biological materials.
3.7. Patient Groups and Statistical Analysis
- For analysis of colonization dynamics, patients were divided into two groups: Group 1 consisted of 21 patients primarily admitted to the NCMC (community-admitted), and Group 2 consisted of 27 patients transferred from other medical institutions (inter-hospital transfers). Differences between proportions were assessed using Student’s t-test and Fisher’s exact test where appropriate. Logistic regression analysis was performed to identify independent predictors of carbapenem-resistant organism acquisition, with variables including group (primary vs. transferred), observation stage, duration of prior antibiotic exposure, and underlying diagnosis. All analyses were performed using SPSS version 26.0 (IBM, USA). A p-value of <0.05 was considered statistically significant.
4. Results
4.1. Overall Microbiological Findings
- A total of 327 isolates representing 27 microbial species were recovered from 159 tracheal aspirate samples obtained from 48 patients. The four predominant organisms were K. pneumoniae, A. baumannii, P. aeruginosa, and S. aureus, together accounting for the majority of clinically relevant isolates. The number of isolates per patient increased progressively with longer PICU stay in both groups, reflecting a growing tendency toward polymicrobial colonization during prolonged ventilation.
4.2. Colonization Dynamics
- In Group 1 (primarily admitted patients), only sparse isolates were recovered during Stage I (days 1–3). By Stage II (days 4–6), nosocomial flora had clearly emerged, including A. baumannii and P. aeruginosa, and recovery of K. pneumoniae and S. aureus increased markedly. Stage III (days 7–9) showed persistence and further enrichment of organisms acquired in Stage II. In Group 2 (transferred patients), hospital-associated microorganisms including K. pneumoniae and A. baumannii were already present at Stage I and remained frequent throughout follow-up. P. aeruginosa increased progressively, and Stenotrophomonas maltophilia appeared in later stages. These patterns confirm that transferred patients arrive pre-colonized with MDR flora, whereas primarily admitted patients acquire ICU-specific pathogens after days 4–6.
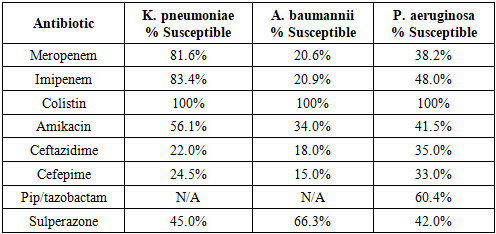
4.3. Antibiotic Resistance Patterns
- Carbapenem resistance rates were notably high across the major pathogens. Detailed susceptibility data for the key organisms are presented in Table 1. Among P. aeruginosa isolates, resistance to meropenem was detected in 61.8% and to imipenem in 52.0% of strains. Among A. baumannii, susceptibility to meropenem and imipenem was observed in only 20.6% and 20.9% of strains, respectively, equating to carbapenem resistance exceeding 79%. In K. pneumoniae, meropenem and imipenem resistance were detected in 18.4% and 16.6% of isolates, respectively. Colistin retained full activity against all tested isolates of all three species. Among aminoglycosides tested against K. pneumoniae, amikacin demonstrated the highest activity (susceptibility in 56.1% of isolates).
|
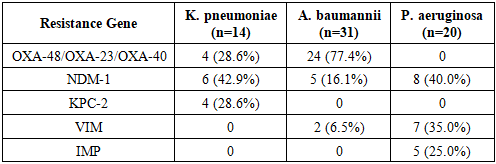
4.4. Carbapenem Resistance Mechanisms
- Among the 65 carbapenem-resistant Gram-negative isolates subjected to molecular characterization, OXA-type carbapenemases (OXA-23, OXA-40, OXA-51) were the predominant mechanism in A. baumannii. NDM-type metallo-beta-lactamases were detected in K. pneumoniae and P. aeruginosa isolates. KPC-type carbapenemases were identified in a subset of K. pneumoniae strains (Table 2). The co-occurrence of multiple resistance genes in single isolates was observed, particularly in A. baumannii, consistent with international reports of high-risk clonal lineages in ICU settings [14,30].
|
5. Discussion
5.1. Colonization and Infection Patterns
- The present study demonstrates that ICU-associated colonization of the respiratory tract with MDR Gram-negative pathogens occurs rapidly in mechanically ventilated children, typically emerging by days 4–6 in primarily admitted patients. This timeline is consistent with reports from European and Asian PICUs indicating that early-onset VAP (before day 5) is often caused by community-acquired organisms, whereas late-onset VAP reflects ICU-specific flora with higher resistance rates [4,24,31]. The finding that transferred patients were already colonized at Stage I underscores the inter-hospital spread of MDR organisms and the importance of active surveillance cultures at admission.The distinction between colonization and true VAP is clinically critical. In this cohort, the majority of positive tracheal aspirate cultures at Stage I in primarily admitted patients likely represented colonization rather than infection, given the absence of clinical signs of VAP. Applying CDC/NHSN VAP criteria to future studies at this center would allow more precise determination of infection rates and the attributable morbidity of specific pathogens. In the present study, the absence of formal VAP diagnosis is acknowledged as a limitation; however, the microbiological data still provide valid surveillance information on the dynamics of pathogen acquisition.
5.2. Carbapenem Resistance and Therapeutic Implications
- The very high carbapenem resistance rates observed in A. baumannii (>79%) and P. aeruginosa (>52% for imipenem, >61% for meropenem) are alarming and reflect a pattern increasingly described in Central Asian ICUs [27,32]. These rates markedly exceed the WHO’s warning thresholds for last-resort antibiotic use, and they have direct implications for empirical antibiotic prescribing. Critically, colistin retained activity against all tested isolates—an important finding given the limited therapeutic alternatives in pediatric patients, where drugs such as tigecycline and newer beta-lactamase inhibitor combinations have restricted approval [25,33].Amikacin demonstrated the highest activity among aminoglycosides against K. pneumoniae (56.1% susceptibility), consistent with its preferential use in pediatric infections where gentamicin resistance is common [34]. The detection of NDM and OXA carbapenemases—the dominant mechanisms identified in this cohort—aligns with global surveillance data showing the spread of NDM-producing Enterobacteriaceae and OXA-23/40-producing A. baumannii in Eastern European and Central Asian regions [35]. The co-existence of multiple carbapenemase genes in individual A. baumannii isolates is particularly concerning, as it severely limits therapeutic options and complicates infection control.
5.3. Empirical vs. Targeted Therapy and Antibiotic Stewardship
- Given the high rates of carbapenem resistance observed, empirical broad-spectrum carbapenem therapy is unlikely to provide adequate coverage for the majority of A. baumannii and P. aeruginosa infections in this unit. Conversely, unnecessary empirical carbapenem use further drives resistance selection. The current data strongly support a two-pronged approach: (1) use of local antibiograms to guide empirical therapy by time of admission (primary vs. transfer) and stage of ventilation; and (2) early microbiological sampling at admission followed by targeted, culture-directed therapy as soon as results are available (typically within 48–72 hours).De-escalation protocols—whereby initial broad-spectrum coverage is narrowed once culture and sensitivity results are available—are endorsed by international antimicrobial stewardship guidelines [36,37]. At this center, implementing structured de-escalation rounds and regular review of antibiotic prescriptions against microbiological data would reduce selective pressure and help preserve the activity of last-resort agents such as colistin. Combination therapy (e.g., colistin plus a carbapenem or sulperazone) may be considered for extensively drug-resistant (XDR) A. baumannii infections, though clinical outcome data from pediatric patients remain limited [33].
5.4. Limitations
- Several limitations of this study should be acknowledged. First, the single-center design at a tertiary referral center in Tashkent limits the generalizability of resistance rates to other institutions or regions. Second, the sample size (48 patients), although appropriate for a single-center surveillance study, restricts the power of subgroup and regression analyses. Third, formal VAP diagnoses were not systematically applied, preventing precise quantification of infection-attributable outcomes. Fourth, detailed data on pre-ICU antibiotic exposure and clinical outcomes (ICU mortality, length of stay) were not fully captured in the current dataset and should be incorporated in future prospective studies at this center. Finally, the EUCAST interpretive criteria used were updated to the 2023 version during data analysis; results originally interpreted using 2014 criteria were re-evaluated accordingly.
6. Conclusions
- Children receiving prolonged mechanical ventilation in the PICU are rapidly colonized and infected by MDR Gram-negative nosocomial pathogens, predominantly K. pneumoniae, A. baumannii, and P. aeruginosa. Colonization with ICU-specific flora emerges by days 4–6 in primarily admitted patients and is already established at admission in patients transferred from other facilities.Carbapenem resistance is extremely prevalent, particularly in A. baumannii (>79%) and P. aeruginosa (>52–61%), rendering empirical carbapenem monotherapy insufficient for a large proportion of infections. Colistin remains the most consistently active agent against these pathogens, while amikacin offers the best aminoglycoside activity against K. pneumoniae. NDM and OXA carbapenemases are the dominant resistance mechanisms.These findings emphasize the urgent need for individualized, microbiology-guided antibiotic therapy, implementation of antimicrobial stewardship programs incorporating local antibiograms and structured de-escalation, and active surveillance for MDR organisms at admission. Future studies should incorporate formal VAP diagnostic criteria, clinical outcome data, and antibiotic exposure histories to fully characterize the clinical impact of ICU-acquired MDR infections in this population.