-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1853-1857
doi:10.5923/j.ajmms.20261604.62
Received: Mar. 3, 2026; Accepted: Mar. 25, 2026; Published: Apr. 15, 2026

Efficiency of Combined Plastic Surgery Methods in Treating Scar Deformities of the Dorsal Foot
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMadazimov M. M., Ergashev K. N., Askhanov Z. P., Turgunov B. A.
Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Madazimov M. M., Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Post-burn scar deformities of the dorsal surface of the foot and toe contractures significantly limit daily activities and reduce quality of life. Surgical correction of extensive and deep burn scars, while preserving interdigital folds and preventing syndactyly, is challenging. This study evaluates a combined plastic surgery technique using full-thickness skin grafts (FTSG) and “P”-shaped flaps from interdigital folds. Between 2015 and 2024, 32 patients with extensive dorsal foot burn scars underwent this procedure. Scar areas ranged from 53 to 105 cm² (mean 78.1 ± 3.2 cm²). The technique included scar excision, flap preparation and fixation, FTSG harvesting from the proximal thigh or hypogastric region, and precise graft placement with “L”-shaped sutures to preserve vascularization. Postoperative monitoring involved thermography, transcutaneous oxygen tension (PtcO₂), and hypothermia therapy for 1–7 days to support graft adaptation. Early complications occurred in 9.4% of cases, including partial graft lysis, hematoma, or wound infection, all resolved conservatively. Long-term follow-up showed persistent complications in 9.4% (hyperpigmentation or hypertrophic scars), treated with physiotherapy and topical therapy. No cases of flap necrosis or secondary graft contracture were observed. Overall, the method demonstrated 90.6% effectiveness, ensuring reliable restoration of skin integrity, functional preservation of toes, and favorable cosmetic outcomes. The approach provides single-stage correction, reduces postoperative risks, and optimizes both functional and aesthetic results. This method is protected by Uzbekistan patent IAP 8123 (2025).
Keywords: Burn scar deformity, Full-thickness skin graft, Combined plastic surgery, Toe contracture, Syndactyly, Dorsal foot
Cite this paper: Madazimov M. M., Ergashev K. N., Askhanov Z. P., Turgunov B. A., Efficiency of Combined Plastic Surgery Methods in Treating Scar Deformities of the Dorsal Foot, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1853-1857. doi: 10.5923/j.ajmms.20261604.62.
Article Outline
1. Introduction
- Burn scar contractures remain a significant clinical challenge due to their impact on patients’ functional abilities, aesthetic outcomes, and quality of life [1,2]. The incidence of contracture formation is particularly high in low- and middle-income countries, where access to timely burn care and rehabilitation is limited, resulting in prolonged disability and social isolation [1,3]. Post-burn contractures frequently affect joint mobility, leading to severe limitations in activities of daily living and occupational performance [4,5].Despite advances in reconstructive surgery, recurrence rates remain substantial, especially in complex anatomical regions such as the axilla, neck, and extremities [6,7]. The development of contractures is influenced by multiple factors including depth and extent of the burn, delayed wound healing, inadequate early physiotherapy, and the use of inappropriate surgical techniques [2,8,9]. Functional impairment due to contractures not only increases dependency but also contributes to psychological distress and diminished quality of life [10,11].Early and effective management, including surgical release, skin grafting, flap reconstruction, and post-operative rehabilitation, is critical for restoring function and minimizing long-term disability [12,13]. However, limited standardized protocols and variability in surgical outcomes pose ongoing challenges to clinicians [14]. Recent systematic reviews and multicenter studies emphasize the urgent need for optimized strategies combining surgical, physiotherapeutic, and preventive approaches to improve patient-centered outcomes [5,15].Overall, the persistent prevalence of burn scar contractures, their functional and psychosocial consequences, and the high recurrence rates underscore the clinical and public health relevance of this problem, necessitating continued research and evidence-based intervention strategies [1,15].
2. Purpose of the Study
- To evaluate the efficacy of a combined reconstructive surgical technique, developed by the author, employing a full-thickness skin graft (FTSG) together with “P”-shaped dermal-fat flaps harvested from the interdigital spaces, for the simultaneous correction of extensive scar deformities on the dorsal surface of the foot and contractures of the toes.
3. Materials and Methods
- The study was conducted from 2015 to 2024 at the Republican Scientific Center for Emergency Medical Care and included patients treated at the Andijan Regional Multidisciplinary Medical Center, Department of Trauma Sequelae and Orthopedics, as well as at the private MCM Med Clinic. In the main group, out of 99 patients, 32 (32.3%) presented with scar deformities on the dorsal surface of the foot and flexion contractures of the toes. These deformities were corrected using a combination of Z-plasty and “P”-shaped flap techniques. The scarred areas ranged from 53 cm² to 105 cm², with a mean of 78.1 ± 3.2 cm². Statistical analysis showed a chi-square (χ²) value of 54.09 with 35 degrees of freedom (df) and a P-value of 0.012, confirming the statistical reliability of the selected patient groups.The surgical procedure included the following steps:1. Excision of scar tissue from the tarsal joint to the distal phalanx of the toes;2. Creation of “P”-shaped skin-fat flaps from intact interdigital web spaces;3. Formation of commissures by securing the flap tips between the metacarpal bones;4. Harvesting full-thickness skin grafts from the donor site 87.5% from the proximal third of the thigh and 12.5% from the hypogastric region of the abdomen using a specialized roller;5. Adaptation and suturing of the graft to the defect, with placement of “L”-shaped sutures at the corners connecting the “P”-shaped flaps.During donor site preparation, alcoholic antiseptics were avoided, and 25% chlorhexidine or hexamidine solutions were used. Postoperatively, hypothermia was applied during days 1–7. The condition of the grafts was monitored using skin thermometry and transcutaneous oximetry (PtcO₂).
4. Results
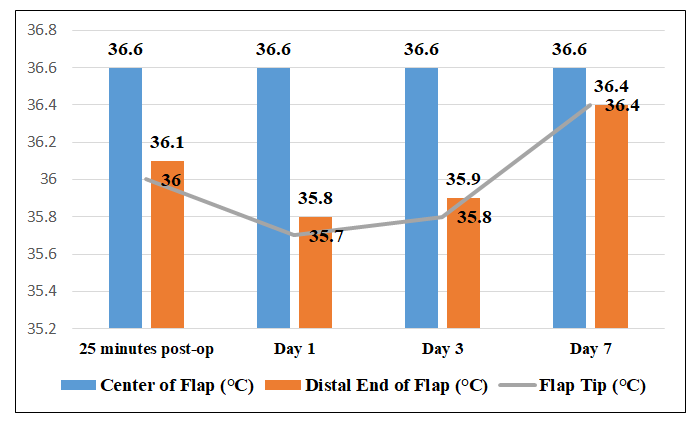
- Surgical Technique. After general anesthesia, the surgical field was disinfected three times using an alcohol–povidone-iodine–alcohol sequence. Scar tissue was excised along the intermediate layer from the tarsal joint to the dorsal surface of the distal phalanges of the toes using a scalpel in a sequential manner. Care was taken to preserve the venous network of the dorsal surface of the foot during excision.Redression. To prevent long-term complications following syndactyly release, “P”-shaped skin-fat flaps were created from the intact interdigital web spaces and the medial surfaces of the proximal phalanges. The tips of these flaps were mobilized for subsequent positioning.Hemostasis. Hemostasis was achieved as needed. The bases of the flaps measured at least 1 cm, the distal tips approximately 0.4–0.8 cm, with angles of 90°. The flap tips were secured in the anatomical space between the heads or inner edges of the metacarpal bones using two non-traumatic sutures, thereby forming interdigital commissures. Each distal phalanx was temporarily fixed with a suture taken from the nail region, and the toes were hypercorrected and sutured to the dorsal surface of the foot.Full-thickness skin grafts were harvested from the donor site using a specialized roller and scalpel: in 28 cases (87.5%) from the proximal third of the anterior thigh, and in 4 cases (12.5%) from the hypogastric region of the abdomen. The grafts were applied to the defect, and the wound edges were secured with 3.0–4.0 non-traumatic interrupted sutures. To prevent necrosis at the corners where the “P”-shaped flaps met the graft, two “L”-shaped sutures were placed at each corner. The “L”-shaped suture differs from conventional interrupted sutures in that the needle first passes through the graft over the metatarsal heads, then subdermally through the free edge of the flap, and exits parallel to the first pass. The contralateral corner of the flap is sutured in the same manner.The graft was then covered with sterile gauze moistened with physiological saline, and a pressure dressing (“Pelotte”) was applied. The procedure was completed with an aseptic dressing and a contralateral plaster splint.Donor Site Preparation. Alcohol and iodine were avoided during donor site preparation due to previous observations of chemical burns leading to partial epidermal graft loss in 25–37% of cases. Instead, 0.05–25% chlorhexidine or hexamidine solutions were used. The donor wound edges were mobilized, approximated, and secured with interrupted sutures.Postoperative Care. To facilitate gradual restoration of microcirculation, local hypothermia was applied for 1–7 days postoperatively. All sutures were removed on postoperative days 11–12. Graft viability was monitored using skin thermometry and transcutaneous oximetry (PtcO₂).Intellectual Property. The proposed method was patented by the Intellectual Property Agency under the Ministry of Justice of the Republic of Uzbekistan on May 27, 2025 (Patent No. IAP 8123) under the title: “Method for simultaneous correction of post-burn scar deformities of the dorsal surface of the foot.”Instrumental Monitoring of Graft Condition. According to skin thermometry results, the temperature of the grafts gradually changed during the postoperative period in accordance with the stepwise restoration of microcirculation. Although the temperature was relatively low at 25 minutes post-surgery, it progressively normalized on days 1, 3, and 7 (see Figure 1).
 | Figure 1 |
 | Figure 2 |
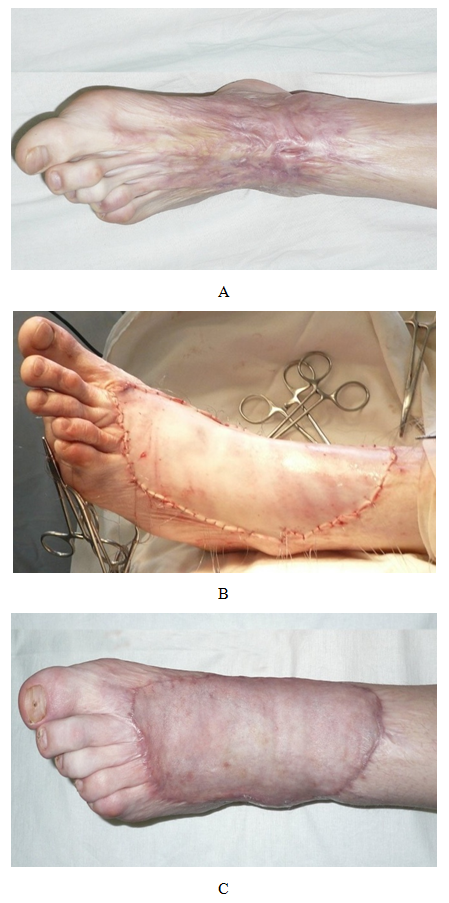 | Figure 3. A. Post-burn scar deformity of the left lower leg, ankle joint, and dorsal surface of the foot. B. Wound covered with a full-thickness skin graft. C. Long-term postoperative outcome |
5. Discussion
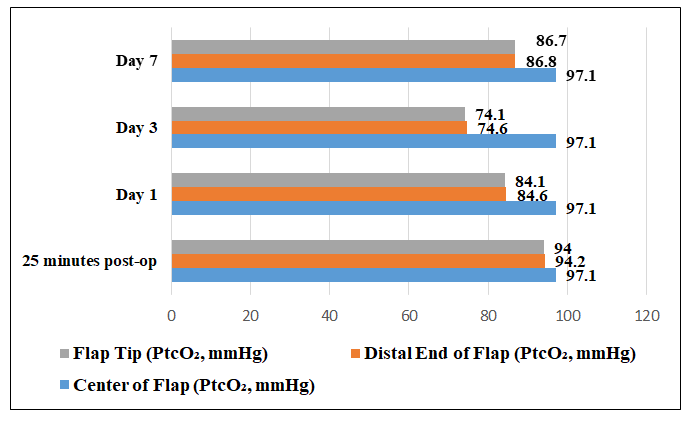
- The results of this study indicate that the choice of a plastic reconstructive surgical method for treating post-burn scar deformities of the dorsal surface of the foot depends on the size, depth, and proximity of the deformity to functionally active zones.In cases of large post-burn scar deformities, particularly when the interdigital web spaces were involved, a combination of full-thickness skin grafting with flap-based plastic reconstruction proved most effective, yielding a 90.6% positive outcome. The main advantages of this approach include:1. The ability to simultaneously cover the scar defect and reconstruct the interdigital commissures;2. Prevention of syndactyly complications using “P”-shaped flaps;3. Preservation of blood circulation at the flap corners via “L”-shaped sutures;4. High elasticity and minimal hyperpigmentation of the full-thickness skin grafts.Avoiding alcohol-based antiseptics and using 0.05% chlorhexidine solution for donor site preparation completely prevented epidermal detachment due to chemical burns. This simple yet critical modification significantly improved donor site healing. Postoperative hypothermia facilitated the gradual restoration of microcirculation in the grafts. The observed decrease in PtcO₂ until day 3, followed by normalization, confirms the protective effect of hypothermia. This method facilitated graft adaptation and contributed to complete wound healing. The observed complication rates were relatively low (9.4% in the short term and 9.4% in the long term) and were successfully managed with conservative therapy. Importantly, no serious complications such as flap tip necrosis or graft twisting were observed in patients treated with the proposed methods. Comparative analysis demonstrated that the effectiveness of plastic reconstructive surgery decreases as scar depth and size increase. This finding highlights the importance of a differential approach and careful selection of surgical technique based on the severity of the scar deformity.
6. Conclusions
- The combined plastic reconstructive approach, incorporating full-thickness skin grafts and “P”-shaped flaps for the interdigital web spaces, has proven highly effective for the treatment of extensive and deep post-burn scar deformities of the dorsal surface of the foot. This method allows for single-stage correction, minimizing the risk of postoperative complications such as syndactyly and flap tip necrosis, while providing favorable functional and aesthetic outcomes. Avoiding alcohol-based antiseptics and utilizing a 0.05% chlorhexidine solution for donor site preparation effectively prevents epidermal detachment caused by chemical burns, significantly enhancing donor site healing. Additionally, the application of postoperative hypothermia supports the gradual restoration of microcirculation within the grafts, facilitating complete graft integration and optimal tissue adaptation. Overall, this approach represents a reliable, safe, and functionally efficient strategy for reconstructing severe post-burn deformities of the dorsal foot, ensuring high patient satisfaction and minimal complication rates.