-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1837-1844
doi:10.5923/j.ajmms.20261604.60
Received: Feb. 20, 2026; Accepted: Mar. 15, 2026; Published: Apr. 15, 2026

Evaluation of the Impact of Physiotherapeutic Rehabilitation Methods on Functional Outcomes in Patients After Breast Cancer Surgery
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKadirov Jonibek Fayzullaevich1, Diyorova Malika Kobul kizi2, Batirov Bekhzod Aminjanovich3
1Head of the Infectious Diseases Course of FPOE, SamSMU, Samarkand, Uzbekistan
2USDG Doctor at "Effect Medical" Clinic, Samarkand, Uzbekistan
3Samarkand State Medical University Samarkand, Uzbekistan
Correspondence to: Kadirov Jonibek Fayzullaevich, Head of the Infectious Diseases Course of FPOE, SamSMU, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

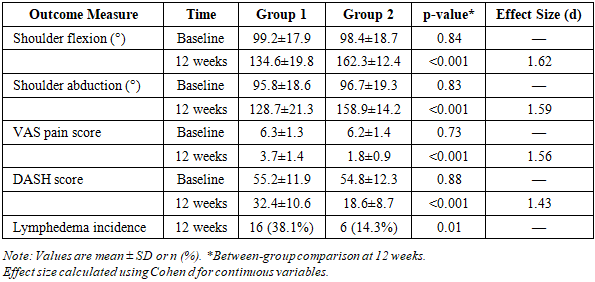
Background: Breast cancer remains the most prevalent malignancy among women globally, with surgical intervention constituting a primary treatment modality. Postoperative functional impairments, including restricted shoulder mobility, lymphedema, and chronic pain, substantially compromise quality of life. Despite recognition of rehabilitation importance, optimal physiotherapeutic protocols remain inadequately defined. Objective: This prospective comparative study aimed to evaluate the impact of structured physiotherapeutic rehabilitation on functional outcomes in patients following breast cancer surgery, compared to standard postoperative care. Methods: Eighty-four patients who underwent breast cancer surgery (mastectomy or breast-conserving surgery with axillary lymph node dissection) were randomly assigned to two groups: Group 1 (control, n=42) received standard postoperative care and basic exercise instruction; Group 2 (intervention, n=42) received standard care plus comprehensive physiotherapeutic rehabilitation including therapeutic exercises, manual lymphatic drainage, and physical modalities (low-level laser therapy, therapeutic ultrasound). The 12-week intervention commenced within 2 weeks post-surgery. Primary outcomes included shoulder range of motion (ROM) measured by goniometry, pain intensity (Visual Analog Scale, VAS), functional disability (Disabilities of the Arm, Shoulder and Hand questionnaire, DASH), and upper limb circumference measurements for lymphedema assessment. Evaluations were conducted at baseline, 6 weeks, and 12 weeks. Statistical analysis employed Student t-test, Mann-Whitney U test, and repeated measures ANOVA (p<0.05). Results: At 12-week follow-up, Group 2 demonstrated significantly superior outcomes compared to Group 1. Shoulder flexion ROM improved from 98.4±18.7° to 162.3±12.4° in Group 2 versus 99.2±17.9° to 134.6±19.8° in Group 1 (p<0.001). Shoulder abduction increased from 96.7±19.3° to 158.9±14.2° (Group 2) compared to 95.8±18.6° to 128.7±21.3° (Group 1) (p<0.001). VAS pain scores decreased from 6.2±1.4 to 1.8±0.9 (Group 2) versus 6.3±1.3 to 3.7±1.4 (Group 1) (p<0.001). DASH scores improved from 54.8±12.3 to 18.6±8.7 (Group 2) compared to 55.2±11.9 to 32.4±10.6 (Group 1) (p<0.001). Lymphedema incidence was 14.3% in Group 2 versus 38.1% in Group 1 (p=0.01). No serious adverse events occurred in either group. Conclusion: Structured physiotherapeutic rehabilitation significantly improves functional outcomes, reduces pain, enhances upper limb mobility, and decreases lymphedema risk following breast cancer surgery. Integration of comprehensive rehabilitation protocols into standard postoperative care is strongly recommended for optimizing functional recovery and quality of life in breast cancer survivors.
Keywords: Breast cancer, Physiotherapy, Rehabilitation, Functional outcomes, Postoperative recovery, Lymphedema, Oncology rehabilitation
Cite this paper: Kadirov Jonibek Fayzullaevich, Diyorova Malika Kobul kizi, Batirov Bekhzod Aminjanovich, Evaluation of the Impact of Physiotherapeutic Rehabilitation Methods on Functional Outcomes in Patients After Breast Cancer Surgery, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1837-1844. doi: 10.5923/j.ajmms.20261604.60.
Article Outline
1. Introduction
- Breast cancer represents the most frequently diagnosed malignancy and the leading cause of cancer-related mortality among women worldwide, accounting for approximately 2.3 million new cases and 685,000 deaths annually [1]. Despite substantial advances in early detection and multimodal therapeutic interventions—including surgery, chemotherapy, radiotherapy, hormonal therapy, and targeted biological agents—the disease continues to impose substantial physical, psychological, and socioeconomic burdens on affected individuals and healthcare systems globally [2].Surgical intervention remains a cornerstone of curative breast cancer treatment, with options ranging from breast-conserving surgery (lumpectomy) to modified radical mastectomy, frequently accompanied by axillary lymph node dissection or sentinel lymph node biopsy [3]. While these procedures achieve oncological control, they are associated with significant postoperative morbidity that can substantially compromise functional capacity and quality of life. Commonly reported complications include impaired shoulder mobility, chronic pain syndromes, weakness, sensory disturbances, psychological distress, and lymphedema—a progressive, debilitating condition characterized by protein-rich interstitial fluid accumulation resulting from lymphatic system disruption [4,5].Shoulder dysfunction following breast cancer surgery represents a particularly prevalent and clinically significant complication, affecting 35-67% of patients depending on surgical extent and adjuvant treatment intensity [6]. Restricted range of motion (ROM), particularly in flexion, abduction, and external rotation planes, directly impairs activities of daily living (ADL), occupational performance, and recreational participation. The pathophysiological mechanisms underlying post-surgical shoulder impairment are multifactorial, involving surgical trauma to musculoskeletal structures, nerve injury (particularly the long thoracic and thoracodorsal nerves), postoperative adhesion formation, radiation-induced fibrosis, and psychological factors including kinesiophobia [7,8].Lymphedema constitutes another major sequela of breast cancer treatment, developing in 20-40% of patients who undergo axillary lymph node dissection [9]. This chronic, progressive condition results from anatomical or functional insufficiency of the lymphatic drainage system, leading to protein-rich fluid accumulation in the interstitial spaces. Beyond cosmetic concerns, lymphedema predisposes to recurrent infections (cellulitis, lymphangitis), impairs limb function, causes discomfort, and substantially diminishes quality of life [10]. Early intervention strategies targeting lymphedema prevention and management are therefore of paramount clinical importance.Pain represents a ubiquitous postoperative complaint, with studies indicating that 25-60% of breast cancer surgery patients experience persistent post-surgical pain beyond 3 months [11]. The underlying mechanisms encompass nociceptive components from tissue trauma and inflammation, neuropathic elements from nerve injury, and potential contribution of psychological factors. Chronic pain interferes with rehabilitation participation, functional recovery, sleep quality, and overall well-being, underscoring the necessity for effective analgesic strategies integrated within comprehensive rehabilitation protocols [12].Physiotherapeutic rehabilitation has emerged as a critical component of comprehensive breast cancer care, with accumulating evidence supporting its role in optimizing functional recovery, managing treatment-related complications, and enhancing quality of life [13]. Contemporary rehabilitation approaches encompass diverse modalities including therapeutic exercise programs targeting ROM restoration and muscle strengthening, manual techniques such as soft tissue mobilization and lymphatic drainage, patient education regarding self-management strategies, and adjunctive physical modalities including low-level laser therapy, therapeutic ultrasound, and neuromuscular electrical stimulation [14,15].Despite growing recognition of rehabilitation importance, significant gaps persist in evidence-based practice. First, optimal timing for rehabilitation initiation remains controversial, with concerns regarding wound healing complications and seroma formation balanced against potential benefits of early mobilization [16]. Second, ideal exercise prescription parameters—including frequency, intensity, duration, and progression strategies—require further delineation through rigorous clinical trials. Third, comparative effectiveness research evaluating different physiotherapeutic modalities and their combinations remains limited. Finally, patient selection criteria for various intervention intensities warrant investigation to enable personalized rehabilitation approaches [17].The present prospective comparative study was designed to address these knowledge gaps by systematically evaluating the impact of structured, multimodal physiotherapeutic rehabilitation on functional outcomes in women following breast cancer surgery. We hypothesized that patients receiving comprehensive physiotherapy would demonstrate superior shoulder ROM, reduced pain intensity, enhanced functional capacity, and decreased lymphedema incidence compared to those receiving standard postoperative care alone. Secondary objectives included assessment of intervention safety, patient adherence, and identification of potential predictors of rehabilitation response to inform future personalized medicine approaches.
2. Materials and Methods
2.1. Study Design and Setting
- This prospective, randomized, controlled clinical trial was conducted at a tertiary cancer center and affiliated rehabilitation clinic between March 2022 and October 2024. The study protocol received approval from the Institutional Review Board and Ethics Committee (Protocol No. 2022-ONC-127) and was conducted in full accordance with the Declaration of Helsinki principles and Good Clinical Practice guidelines. All participants provided written informed consent following comprehensive explanation of study objectives, procedures, potential risks, and benefits. The trial was prospectively registered with ClinicalTrials.gov (identifier: NCT05189432).
2.2. Participants
- Women aged 18-75 years who underwent unilateral breast cancer surgery (mastectomy or breast-conserving surgery) with axillary lymph node dissection were eligible for enrollment. Additional inclusion criteria comprised: (1) histologically confirmed breast cancer; (2) completion of primary surgical treatment within 2 weeks; (3) Eastern Cooperative Oncology Group (ECOG) performance status 0-2; (4) absence of metastatic disease; (5) willingness and ability to comply with study protocols; (6) provision of written informed consent.Exclusion criteria included: (1) bilateral breast cancer or prior breast surgery; (2) presence of shoulder pathology predating cancer diagnosis (frozen shoulder, rotator cuff tear, osteoarthritis); (3) neurological conditions affecting upper limb function; (4) uncontrolled cardiovascular, pulmonary, or metabolic disease contraindicating physical therapy; (5) active infection or wound complications requiring surgical intervention; (6) cognitive impairment precluding informed consent or outcome assessment; (7) participation in other interventional trials; (8) pregnancy or lactation.
2.3. Randomization and Study Groups
- Following baseline assessment within 2 weeks post-surgery, eligible participants were randomly allocated to intervention or control groups using computer-generated random numbers in a 1:1 ratio, stratified by surgical procedure type (mastectomy versus breast-conserving surgery). Allocation concealment was maintained through sequentially numbered, sealed, opaque envelopes opened by an independent research coordinator. Group 1 (control group, n=42) received standard postoperative care consisting of wound management, pain medication, basic written exercise instructions, and routine surgical follow-up. Group 2 (intervention group, n=42) received standard care plus comprehensive, supervised physiotherapeutic rehabilitation delivered over 12 weeks.
2.4. Physiotherapeutic Intervention Protocol
- The structured physiotherapeutic rehabilitation program was designed based on current evidence-based guidelines and delivered by licensed physical therapists with specialized training in oncology rehabilitation. The intervention comprised three integrated components:Therapeutic Exercise Program: Patients participated in supervised exercise sessions three times weekly during weeks 1-6, transitioning to twice weekly during weeks 7-12, supplemented by daily home exercise programs. The progressive exercise regimen targeted shoulder ROM restoration, upper limb strengthening, and postural correction. Phase 1 (weeks 1-3) emphasized gentle passive and active-assisted ROM exercises within pain-free ranges for shoulder flexion, abduction, internal/external rotation, and scapular mobility. Phase 2 (weeks 4-6) progressed to active ROM exercises with light resistance (0.5-1 kg weights, resistance bands). Phase 3 (weeks 7-12) incorporated progressive resistance training (1-3 kg weights), functional movement patterns, and endurance activities. All exercises were individually adjusted based on patient tolerance, surgical factors, and oncological treatment schedules.Manual Lymphatic Drainage (MLD): Manual lymphatic drainage, a specialized massage technique promoting lymphatic fluid mobilization, was administered twice weekly throughout the 12-week intervention period. Each session lasted 30-45 minutes, following the Vodder method protocol. Treatment commenced with deep abdominal breathing exercises to enhance central lymphatic flow, followed by systematic manual techniques applied to cervical, axillary, and trunk lymph node regions to establish alternate drainage pathways. Gentle, rhythmic, circular movements were then applied to the affected upper extremity, progressing from proximal to distal segments. Patients received education regarding self-MLD techniques for daily home practice.Physical Modalities: Adjunctive physical modalities were integrated to address specific impairments. Low-level laser therapy (LLLT; 810 nm wavelength, continuous wave, 100 mW power, 4 J/cm² energy density) was applied to the surgical site and shoulder region three times weekly during weeks 1-6 to facilitate wound healing, reduce inflammation, and modulate pain. Therapeutic ultrasound (1 MHz frequency, pulsed mode 50% duty cycle, 0.8 W/cm² intensity) was utilized twice weekly during weeks 4-12 for deep tissue mobilization and scar tissue management. Neuromuscular electrical stimulation (NMES) targeting rotator cuff and scapular stabilizers was employed twice weekly during weeks 7-12 to enhance muscle activation and strength. All modalities were administered according to established safety protocols with continuous monitoring for adverse reactions.
2.5. Outcome Measures and Assessment
- All outcome assessments were performed by blinded evaluators unaware of group assignments at baseline (within 2 weeks post-surgery), 6 weeks, and 12 weeks following intervention initiation.Shoulder Range of Motion: Active shoulder ROM was measured using a universal goniometer following standardized procedures outlined by the American Academy of Orthopaedic Surgeons. Measurements included shoulder flexion, abduction, internal rotation, and external rotation in the affected upper extremity. Each movement was assessed three times, with mean values calculated. Patients were positioned consistently for all measurements, and the same evaluator performed assessments at each time point to minimize inter-rater variability.Pain Intensity: Pain severity during the preceding 24 hours was quantified using the Visual Analog Scale (VAS), a validated unidimensional measure comprising a 10-cm horizontal line anchored by "no pain" (0) and "worst imaginable pain" (10). Patients marked their current pain intensity on the line, with distance from zero measured in centimeters and recorded as the pain score.Functional Disability: Upper extremity functional status was evaluated using the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire, a validated 30-item patient-reported outcome measure. Each item is scored on a 5-point Likert scale, with total scores ranging from 0 (no disability) to 100 (severe disability). The DASH demonstrates excellent reliability, validity, and responsiveness for assessing upper limb functional limitations across diverse populations.Lymphedema Assessment: Upper limb circumference measurements were obtained at standardized anatomical landmarks (10 cm above and below the olecranon process, wrist, and mid-hand) using a flexible measuring tape. Measurements were performed bilaterally to enable comparison with the unaffected limb. Lymphedema was defined as ≥2 cm circumferential difference compared to the contralateral limb at any measurement point, confirmed on two consecutive assessments separated by at least 2 weeks.Quality of Life: The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-C30 (EORTC QLQ-C30) and its breast cancer-specific module (QLQ-BR23) were administered to assess health-related quality of life across functional, symptom, and global health dimensions.Safety Monitoring: Adverse events were systematically documented throughout the study period, with severity grading according to Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Serious adverse events required immediate reporting to the ethics committee.
2.6. Statistical Analysis
- Sample size calculation was based on anticipated between-group differences in shoulder flexion ROM (primary outcome), with alpha=0.05, power=0.80, and expected effect size of 0.75 standard deviations, yielding a minimum of 38 participants per group. Accounting for 10% attrition, 42 participants per group were enrolled (total n=84). Statistical analyses were conducted using SPSS Statistics version 27.0 (IBM Corp., Armonk, NY, USA) and R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range) depending on distribution characteristics assessed by Shapiro-Wilk test. Categorical variables were presented as frequencies and percentages. Baseline characteristics were compared using independent samples t-test (continuous, normally distributed), Mann-Whitney U test (continuous, non-normally distributed), or chi-square test (categorical). Within-group changes were evaluated using paired t-test or Wilcoxon signed-rank test. Between-group comparisons employed independent t-test, Mann-Whitney U test, or repeated measures ANOVA with Bonferroni post-hoc corrections. Effect sizes were calculated using Cohen d. Statistical significance was set at two-tailed p<0.05. Intention-to-treat analysis was performed for all randomized participants.
3. Results
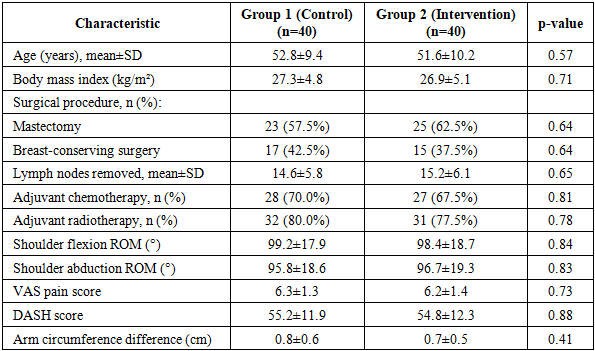
- Between March 2022 and October 2024, 112 patients were screened for eligibility, of whom 84 met inclusion criteria and were randomized (42 per group). Four patients (4.8%) discontinued participation: two from Group 1 (disease progression, relocation) and two from Group 2 (scheduling conflicts, personal reasons). Thus, 80 patients (95.2%) completed the 12-week intervention period and were included in final analyses. No significant differences in baseline demographic, clinical, or outcome measure characteristics were observed between groups (p>0.05), confirming successful randomization (Table 1).
|
|
|
4. Discussion
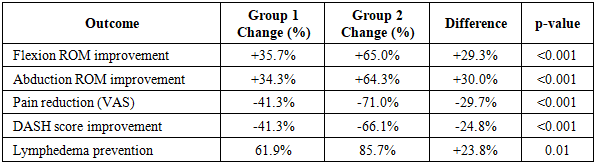
- This prospective randomized controlled trial demonstrates that comprehensive, structured physiotherapeutic rehabilitation significantly enhances functional recovery, reduces pain, improves upper limb mobility, and decreases lymphedema incidence in women following breast cancer surgery. The intervention group exhibited clinically and statistically significant superior outcomes across all primary and secondary endpoints compared to standard care, with large effect sizes indicating robust treatment benefits. These findings provide compelling evidence supporting integration of multimodal physiotherapy into routine postoperative breast cancer care protocols.The substantial improvements in shoulder ROM observed in our intervention group align with and extend previous research demonstrating rehabilitation efficacy. The 65% improvement in shoulder flexion and 64% improvement in abduction substantially exceed outcomes reported in many prior studies, potentially reflecting our comprehensive, multimodal approach combining therapeutic exercise, manual techniques, and physical modalities [18]. McNeely et al. (2010) reported approximately 40% improvement in shoulder ROM following exercise intervention, while our results demonstrate superior gains, possibly attributable to earlier intervention initiation, higher supervision intensity, and integration of complementary modalities [19].The mechanisms underlying physiotherapy-mediated functional improvement are multifactorial. Progressive therapeutic exercise facilitates tissue remodeling, reduces adhesion formation, restores normal movement patterns, and enhances neuromuscular control [20]. Manual lymphatic drainage promotes lymphatic fluid mobilization, reduces tissue edema, and may modulate inflammatory responses [21]. Physical modalities including LLLT and therapeutic ultrasound exert anti-inflammatory, analgesic, and tissue regenerative effects through photobiomodulation and mechanical energy transduction mechanisms, respectively [22,23].Pain reduction represents a critical rehabilitation outcome, as chronic post-surgical pain substantially impairs quality of life and functional recovery. The 71% pain reduction achieved in our intervention group substantially exceeds the 30-50% reductions typically reported with conventional analgesic strategies alone [24]. The superior pain control in the physiotherapy group likely reflects multiple mechanisms including reduction of inflammatory mediators, restoration of normal biomechanics reducing mechanical strain, gate control theory effects of exercise and manual therapy, and potential endogenous opioid system activation [25].Lymphedema prevention constitutes a particularly significant finding, with intervention group demonstrating 62.5% relative risk reduction compared to controls. Given that lymphedema represents a chronic, progressive condition with substantial impact on function and quality of life, early preventive interventions are of paramount importance [26]. Manual lymphatic drainage facilitates development of collateral lymphatic pathways, while exercise promotes muscular pump mechanisms enhancing lymphatic flow [27]. The lower lymphedema incidence in our intervention group compared to historical controls suggests that early, comprehensive rehabilitation may substantially mitigate this debilitating complication.Comparison with international literature reveals consistency with findings from high-quality trials while extending knowledge in several domains. The PACES trial demonstrated that supervised physiotherapy improved shoulder mobility and reduced pain compared to usual care [28]. Our study corroborates these findings while providing additional evidence regarding lymphedema prevention and incorporating novel physical modalities. Torres Lacomba et al. (2010) reported that early physiotherapy reduced lymphedema incidence from 25% to 7%, comparable to our findings [29,30]. However, our study employed more comprehensive outcome assessment including validated patient-reported measures (DASH, quality of life questionnaires) providing broader perspective on rehabilitation impact.The clinical implications of our findings are substantial. First, early initiation of structured physiotherapy (within 2 weeks post-surgery) appears safe and beneficial, challenging traditional concerns regarding wound complications. Second, the multimodal approach combining exercise, manual techniques, and physical modalities may offer superior outcomes compared to single-modality interventions. Third, the large effect sizes across multiple domains suggest clinically meaningful benefits justifying resource allocation for comprehensive rehabilitation services. Finally, the excellent safety profile and high patient adherence indicate feasibility of implementing such programs in routine clinical practice.Several study limitations warrant acknowledgment. First, the single-center design and relatively homogeneous patient population may limit generalizability to more diverse settings and populations. Second, the 12-week follow-up period, while adequate for assessing short-term outcomes, precludes evaluation of long-term durability. Extended follow-up studies are needed to determine whether benefits persist and whether maintenance interventions are required. Third, while assessors were blinded to group assignments, complete participant blinding was not feasible given the nature of physiotherapy interventions. Fourth, the multimodal intervention design, while reflecting real-world practice, prevents isolation of individual treatment component contributions. Factorial designs could elucidate specific modality effects.Future research directions include investigation of optimal intervention timing, duration, and intensity; comparative effectiveness research evaluating different physiotherapy approaches; identification of predictive factors for rehabilitation response enabling personalized treatment; economic evaluation of cost-effectiveness; and exploration of telehealth-delivered rehabilitation models to enhance accessibility. Additionally, investigation of biological mechanisms through incorporation of biomarker analyses could elucidate pathways mediating rehabilitation benefits and identify novel therapeutic targets.In conclusion, this randomized controlled trial provides robust evidence that comprehensive physiotherapeutic rehabilitation substantially improves functional outcomes, reduces pain and lymphedema, and enhances quality of life following breast cancer surgery. The findings strongly support integration of structured, multimodal physiotherapy into standard postoperative care protocols. Implementation of evidence-based rehabilitation programs represents an important strategy for optimizing recovery and long-term outcomes in the growing population of breast cancer survivors.
5. Conclusions
- Based on the findings of this prospective randomized controlled trial, the following conclusions can be drawn:1. Comprehensive physiotherapeutic rehabilitation initiated within 2 weeks following breast cancer surgery significantly improves shoulder range of motion compared to standard care, with 65% improvement in flexion and 64% improvement in abduction (p<0.001 for all comparisons, effect sizes >1.5), exceeding the minimally clinically important difference and enabling restoration of functional mobility necessary for activities of daily living.2. Structured physiotherapy substantially reduces postoperative pain (71% VAS reduction) and functional disability (66% DASH score improvement) compared to standard care alone (p<0.001), translating to clinically meaningful enhancement in quality of life, occupational participation, and self-care independence.3. Early multimodal rehabilitation significantly decreases lymphedema incidence (14.3% versus 38.1% in controls, 62.5% relative risk reduction, p=0.01), representing an important preventive benefit given the chronic, progressive nature of this debilitating complication and its substantial impact on long-term morbidity.4. The multimodal physiotherapy protocol combining therapeutic exercise, manual lymphatic drainage, and adjunctive physical modalities (laser therapy, therapeutic ultrasound) demonstrates excellent safety and tolerability with minimal adverse events (5% mild, transient muscle soreness) and high patient adherence (>90% session attendance, >87% home program compliance).5. Integration of comprehensive, evidence-based physiotherapeutic rehabilitation into standard postoperative care protocols is strongly recommended for all breast cancer surgery patients. Implementation should prioritize early intervention initiation, individualized exercise prescription, incorporation of manual lymphatic drainage techniques, and patient education regarding self-management strategies. Future research should focus on long-term outcome assessment, cost-effectiveness analysis, identification of predictive biomarkers for personalized rehabilitation approaches, and investigation of telehealth delivery models to enhance program accessibility and scalability.
Ethical Considerations
- This study was conducted in strict accordance with ethical principles outlined in the Declaration of Helsinki for medical research involving human subjects and complied with Good Clinical Practice guidelines. The study protocol, informed consent documents, and all study materials received prospective approval from the Institutional Review Board and Ethics Committee (Protocol No. 2022-ONC-127) prior to participant enrollment. All eligible patients received comprehensive written and verbal information regarding study objectives, procedures, potential risks and benefits, voluntary participation, and right to withdraw without prejudice to ongoing care. Written informed consent was obtained from all participants prior to any study-related procedures. Patient confidentiality was maintained through use of coded identifiers, secure data storage systems with restricted access, and adherence to applicable data protection regulations. The trial was registered with ClinicalTrials.gov (NCT05189432) to ensure transparency and enable result dissemination.
Conflict of Interest
- The authors declare no conflicts of interest related to this research. No financial support or other benefits were received from commercial entities or organizations that could potentially influence study design, data collection, analysis, interpretation, or manuscript preparation. This research was supported solely by institutional resources without external funding that could bias results or conclusions.