-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1780-1781
doi:10.5923/j.ajmms.20261604.48
Received: Mar. 12, 2026; Accepted: Apr. 6, 2026; Published: Apr. 13, 2026

Predictive Value of Cystatin C and VEGF Biomarkers in Pregnant Women with a History of Severe Preeclampsia and Pyelonephritis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSaporbayeva Inoyat Ravshanbek qizi1, Babajanova Guljakhan Sattarovna2
1Tashkent State Medical University, Tashkent, Uzbekistan
2Professor, Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Severe preeclampsia and pyelonephritis are major causes of maternal and perinatal morbidity. Early prediction of complications is essential for improving outcomes. Biomarkers such as cystatin C and VEGF may provide critical diagnostic and prognostic information. Objective: To evaluate the clinical and predictive significance of cystatin C and VEGF in pregnant women with severe preeclampsia and pyelonephritis. Methods: A retrospective cohort study included 110 pregnant women: 65 with severe preeclampsia (Group 1) and 45 with severe preeclampsia complicated by pyelonephritis (Group 2). Group 2 was subdivided into women who received pregravid preparation (2A, n=30) and those who did not (2B, n=15). Serum cystatin C and VEGF levels were measured by ELISA. Statistical comparisons were performed between groups. Results: Women in Group 2 showed significantly higher cystatin C levels (p<0.01) and lower VEGF levels (p<0.01) compared with Group 1. Pregravid preparation was associated with more favorable biomarker profiles, indicating reduced risk of adverse pregnancy outcomes. Conclusion: Cystatin C and VEGF are valuable predictive biomarkers for pregnancy complications in women with severe preeclampsia and pyelonephritis. Pregravid preparation may mitigate biomarker abnormalities and associated risks.
Keywords: Preeclampsia, Pyelonephritis, Pregnancy complications, Cystatin С, VEGF, Biomarkers, Pregravid preparation
Cite this paper: Saporbayeva Inoyat Ravshanbek qizi, Babajanova Guljakhan Sattarovna, Predictive Value of Cystatin C and VEGF Biomarkers in Pregnant Women with a History of Severe Preeclampsia and Pyelonephritis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1780-1781. doi: 10.5923/j.ajmms.20261604.48.
1. Introduction
- Hypertensive disorders of pregnancy affect approximately 5–10% of all pregnancies worldwide and remain a leading cause of maternal and perinatal morbidity and mortality. Among them, Preeclampsia complicates about 2–8% of pregnancies, with severe forms accounting for nearly 25–30% of cases. According to global estimates, preeclampsia is responsible for up to 10–15% of maternal deaths and contributes significantly to adverse perinatal outcomes, including intrauterine growth restriction, preterm birth, and perinatal mortality rates reaching 20–25% in low-resource settings [1,2], nm jm.Severe preeclampsia is characterized by systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg, along with signs of target organ damage such as proteinuria (>300 mg/24 hours), renal insufficiency, or hepatic dysfunction. The condition is strongly associated with endothelial dysfunction, impaired placental perfusion, and systemic inflammatory response, which together increase the risk of complications such as eclampsia, HELLP syndrome, and acute kidney injury in up to 30–40% of severe cases [3,4].Infectious complications, particularly Pyelonephritis, further aggravate the clinical course of pregnancy. Acute pyelonephritis occurs in approximately 1–2% of pregnancies and is one of the leading causes of non-obstetric hospitalization among pregnant women. It is associated with serious complications, including urosepsis in 10–20% of cases and preterm labor in 20–50% of affected pregnancies [5,6]. When pyelonephritis coexists with severe preeclampsia, the risk of adverse maternal outcomes increases by nearly 1.5–2 times due to overlapping mechanisms such as systemic inflammation and renal dysfunction [7].In recent years, increasing attention has been paid to early predictive biomarkers that could improve risk stratification in high-risk pregnancies. One such marker is Cystatin C, a low-molecular-weight protein produced by all nucleated cells and freely filtered by the glomeruli. Serum cystatin C levels above 1.0–1.2 mg/L have been associated with a 2–3-fold increased risk of severe preeclampsia and renal impairment [8,9].Another important biomarker is Vascular Endothelial Growth Factor, a key regulator of angiogenesis and endothelial integrity. In preeclampsia, circulating VEGF levels are reduced by approximately 30–50% compared to normal pregnancy, contributing to placental insufficiency and endothelial dysfunction [10].Despite evidence supporting the individual roles of cystatin C and VEGF, limited data exist regarding their combined predictive value in pregnant women with both severe preeclampsia and pyelonephritis. Given that both conditions independently increase maternal and perinatal risks, their coexistence necessitates improved predictive strategies. Therefore, this study aims to evaluate the predictive value of cystatin C and VEGF biomarkers in pregnant women with severe preeclampsia complicated by pyelonephritis, with the goal of improving early diagnosis and reducing adverse outcomes.
2. Materials and Methods
- A retrospective cohort study including 110 pregnant women. Group 1: 65 women with severe preeclampsia. Group 2: 45 women with severe preeclampsia and pyelonephritis. Group 2A (n=30): received pregravid preparation. Group 2B (n=15): no pregravid preparation. Serum cystatin C and VEGF levels were measured by ELISA. Statistical analysis included t-test and chi-square. P-values <0.05 considered significant.
3. Results
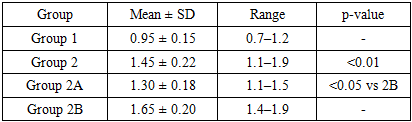
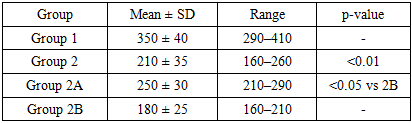
- Cystatin C levels were significantly higher in Group 2 vs Group 1 (p<0.01). VEGF levels were significantly lower in Group 2 vs Group 1 (p<0.01). Pregravid preparation (2A) was associated with lower cystatin C and higher VEGF compared with 2B (p<0.05).
|
|
4. Discussion
- This study demonstrates that severe preeclampsia with pyelonephritis is associated with elevated cystatin C and reduced VEGF, reflecting renal impairment and impaired placental angiogenesis. Pregravid preparation appears to improve biomarker profiles and may reduce the risk of adverse pregnancy outcomes. These findings align with previous literature on predictive value of cystatin C and VEGF. Limitations include retrospective design, single-center data, and small subgroup sample size. Further prospective multicenter studies are recommended.
5. Conclusions
- Cystatin C and VEGF biomarkers are valuable predictive indicators for pregnancy complications in women with severe preeclampsia and pyelonephritis. Pregravid preparation may normalize biomarker profiles and improve maternal-fetal outcomes.