-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1764-1768
doi:10.5923/j.ajmms.20261604.45
Received: Mar. 13, 2026; Accepted: Apr. 7, 2026; Published: Apr. 11, 2026

Immunohistochemical Characteristics of Changes Occurring in the Acute Coronary Arteries After Atherosclerosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMuydinov Javlonbek Ibrokhimovich1, Eshbaev Erkin Abdukhalimovich2
1PhD, Associate Professor, Department of Pathophysiology and Pathological Anatomy, Fergana Public Health Medical Institute, Fergana, Uzbekistan
2DSc in Doctor of Medical Sciences, Professor, Department of Pathological Anatomy, Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In immunohistochemical examinations of coronary arteries affected by acute coronary syndrome, paraffin-embedded materials were analyzed using standard immunohistochemical methods with the help of monoclonal antibodies. CD31 serves as a marker for detecting endothelial cells of blood vessels and the proliferation of mesenchymal cells, whereas VEGFR-1 is used to directly identify vascular endothelial growth factors associated with endothelial cell proliferation, as well as the process of neoangiogenesis and neovascularization of small-caliber vessels in the damaged area. This allows for a clearer understanding and precise assessment of vascular changes in atherosclerosis.
Keywords: Immunohistochemical examination, Chronic coronary syndrome, Ischemia, Myocardium, Stenosis, Necrobiosis, Dystrophy
Cite this paper: Muydinov Javlonbek Ibrokhimovich, Eshbaev Erkin Abdukhalimovich, Immunohistochemical Characteristics of Changes Occurring in the Acute Coronary Arteries After Atherosclerosis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1764-1768. doi: 10.5923/j.ajmms.20261604.45.
Article Outline
1. Introduction
- Worldwide, multifocal atherosclerosis causes damage to elastic and muscular-elastic type arteries in approximately 126 million people. About 16–18% of global mortality is directly associated with coronary artery insufficiency. In terms of mortality rate, this condition ranks first and is characterized by severe lethal outcomes such as infarction and stroke affecting vital organs.The arteries most frequently affected by atherosclerosis are the cardiac (coronary) arteries. Globally, atherosclerotic lesions of the coronary arteries are detected in an average of 1.97 billion individuals aged 45–55 years [1]. This disease is the leading pathological factor in the development of coronary artery stenosis and currently represents a major challenge in endovascular surgical practice.On average, more than 157 million coronary artery stenting procedures are performed annually worldwide. [3] In the United States, 18.8% of total deaths are attributed to coronary artery atherosclerosis, whereas in the Russian Federation this figure reaches 28.4%. In European countries, Australia, and Canada, the average rate is 21.2%. Among Asian countries such as China, Japan, and Korea, 14.4% of the population die from ischemic heart disease (IHD), while in Central Asian countries this indicator accounted for 28.2% of total deaths in 2022. This suggests that IHD demonstrates an earlier onset and higher prevalence among younger age groups compared to many other regions. [2]Globally, more than 10.8 million coronary artery bypass graft (CABG) surgeries are performed annually. Mortality rates from coronary artery disease per 100,000 population are 117.1 in the United States, 781.4 in the Russian Federation, and 137.5 in the European Union, whereas in Central Asian countries this показатель averages 816.5 per 100,000 population. [4]Worldwide, multifocal atherosclerosis causes damage to elastic and muscular-elastic type arteries in approximately 126 million people. About 16–18% of global mortality is directly associated with coronary artery insufficiency. In terms of mortality rate, this condition ranks first and is characterized by severe lethal outcomes such as infarction and stroke affecting vital organs. The arteries most frequently affected by atherosclerosis are the cardiac (coronary) arteries. Globally, atherosclerotic lesions of the coronary arteries are detected in an average of 1.97 billion individuals aged 45–55 years (Povzun S.N., 2015). This disease is the leading pathological factor in the development of coronary artery stenosis and currently represents a major challenge in endovascular surgical practice. [7] On average, more than 157 million coronary artery stenting procedures are performed annually worldwide. In the United States, 18.8% of total deaths are attributed to coronary artery atherosclerosis, whereas in the Russian Federation this figure reaches 28.4%. In European countries, Australia, and Canada, the average rate is 21.2%. Among Asian countries such as China, Japan, and Korea, 14.4% of the population die from ischemic heart disease (IHD), while in Central Asian countries this indicator accounted for 28.2% of total deaths in 2022. This suggests that IHD demonstrates an earlier onset and higher prevalence among younger age groups compared to many other regions. [6] Globally, more than 10.8 million coronary artery bypass graft (CABG) surgeries are performed annually. Mortality rates from coronary artery disease per 100,000 population are 117.1 in the United States, 781.4 in the Russian Federation, and 137.5 in the European Union, whereas in Central Asian countries this показатель averages 816.5 per 100,000 population. [5]One of the most serious and persistent complications in cardiac surgery is myocardial fibrillation, which occurs in 10–65% of cases and accounts for 16% of mortality. In the United States, during the postoperative period following cardiac surgery, myocardial fibrillation is observed on average in 16–50% of patients; the mortality rate among men reaches 20%, while in women it ranges from 13% to 21%. [11]One of the most serious and persistent complications in cardiac surgery is myocardial fibrillation, which occurs in 10–65% of cases and accounts for approximately 16% of overall mortality. In the United States, myocardial fibrillation develops during the postoperative period in an average of 16–50% of patients undergoing cardiac surgery. (10) The mortality rate associated with this complication reaches up to 20% in men, while in women it ranges between 13% and 21%. [8,9]
2. Materials and Methods
- The study utilized clinical-anamnestic analysis, immunohistochemical staining techniques, and statistical research methods. [12]
3. Objective of the Study
- The aim of this study was to investigate the specific features of immunohistochemical examinations in the diagnosis of coronary artery stenosis and myocardial changes in atherosclerosis, as well as to develop practical recommendations for treatment planning. [13]
4. Results and Discussion
- In cases of acute coronary syndrome, coronary artery specimens were subjected to immunohistochemical examination. Paraffin-embedded materials were analyzed using standard immunohistochemical techniques with the application of monoclonal antibodies. CD31 was used as a marker, demonstrating endothelial cell activity and mesenchymal cell proliferation. Its expression was observed at varying levels during all active phases of the cell cycle, including G0, G1, G2, and M phases.When a cell transitions to the post-mitotic G0 phase, the Ki-67 marker is degraded through proteasome-mediated processes and undergoes complete catabolism. [14,15] As a result, it shows negative expression in interphase cells. Since this marker reflects proliferative activity, it is considered important for determining the activity coefficient of vascular structures.VEGFR-1, based on this marker, is directly associated with vascular endothelial growth factors and plays a key role in the processes of neoangiogenesis and neovascularization of small-caliber vessels in damaged areas. It is used to assess any changes in endothelial cell proliferation and, through its positive expression, indicates tissue vascularization, the severity of damage in affected areas, focal endothelial injury, vessels denuded of endothelium, and the progression of thrombosis. For these reasons, VEGFR-1 was utilized as a key factor in our study. [16]CD34 is a membrane protein expressed in many tissue cells and serves as an intercellular adhesion molecule involved in the early stages of hematopoiesis. It plays an important role in evaluating the consequences of vascular diseases, including dystrophic conditions, inflammation, immune disorders, tumors, as well as morphological adaptation and reparative regeneration during intravascular metabolic processes (cell-to-cell adhesion). CD34 serves as an immunohistochemical marker of vascular endothelium and is examined to assess the degree of angiogenesis. In this study, CD34 was used specifically to evaluate angiogenesis. [17]Sections 4 µm thick were prepared from paraffin-embedded blocks, mounted on glass slides, and dried at room temperature for 24 hours. Before staining, the sections were placed vertically in a thermostat at 55 °C for 60 minutes.Afterwards, deparaffinization is performed in xylene (two baths, 10 minutes each), followed by rehydration in decreasing concentrations of ethanol (three baths, 3 minutes each), and rinsing in distilled water. The slide with the section is then heated, placed in a demasking buffer, and subjected to a water bath at 98 °C for 30–40 minutes.After the specimens were cooled to room temperature, they were rinsed in a Tris buffer solution (pH 7.5). To block endogenous peroxidase activity, the sections were treated with 3% H₂O₂ for 15 minutes. To reduce nonspecific binding and limit background staining, the specimens were further processed for 10 minutes.Before adding antibodies, the sections were treated with a special blocking solution to conserve reagents and prevent their runoff. Incubation with the primary antibody was carried out at room temperature for 60–120 minutes.Before direct application, 1 drop of diaminobenzidine (DAB) per 1 ml of azide buffer was used to prepare the working chromogen solution (5–10 minutes exposure, producing a brown color of varying intensity depending on the reaction). Afterwards, the sections were rinsed in distilled water, stained with hematoxylin using standard procedures, and mounted with Canada balsam. Tissue samples were fixed in neutral formalin using routine washing and paraffin embedding. Expression was evaluated in six observation fields (×400 magnification). Based on the intensity and distribution of immunohistochemical staining, the percentage of semi-quantitatively stained cells in six randomly selected fields was calculated (objective ×40). Tumor tissue pieces fixed in 10% neutralized formalin for 72 hours were washed in distilled water for 3–4 hours, dehydrated in graded alcohols (70%, 80%, 90%, 96%, 100%) and chloroform, embedded in paraffin with added wax, and blocks were prepared. [18]
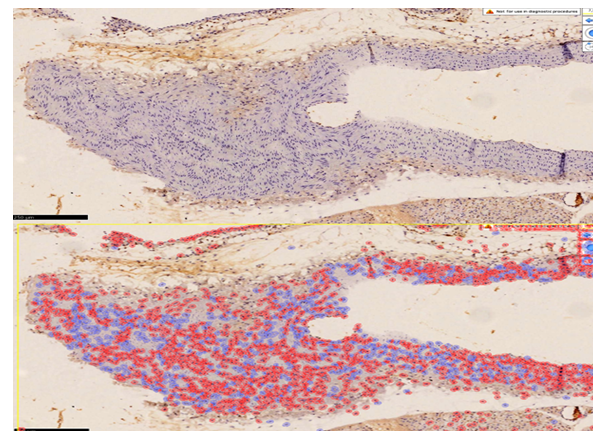 | Figure 1. Coronary artery of a deceased patient with acute ischemic heart disease (patient D, 35 years old). High positive expression of the CD34 marker. Staining: DAB chromogen. Magnification: ×40. Scanned and analyzed for expression level using QuPath 0.4.0. Positively expressing cells are shown in dark red |
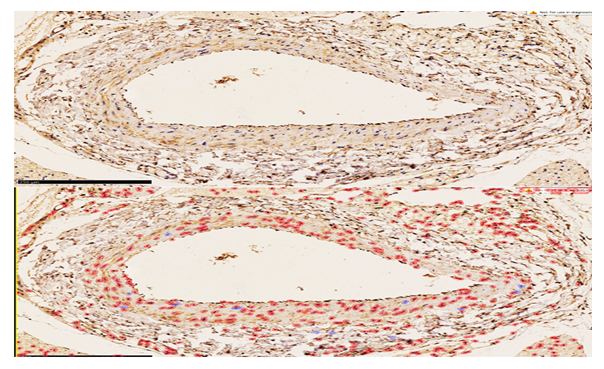 | Figure 2. Arterial vessel of the abdominal thigh region from Group 1, showing high positive expression of the CD34 marker. Staining: DAB chromogen. Magnification: ×40. Scanned and analyzed for expression level using QuPath 0.4.0. Positively expressing cells are shown in red |
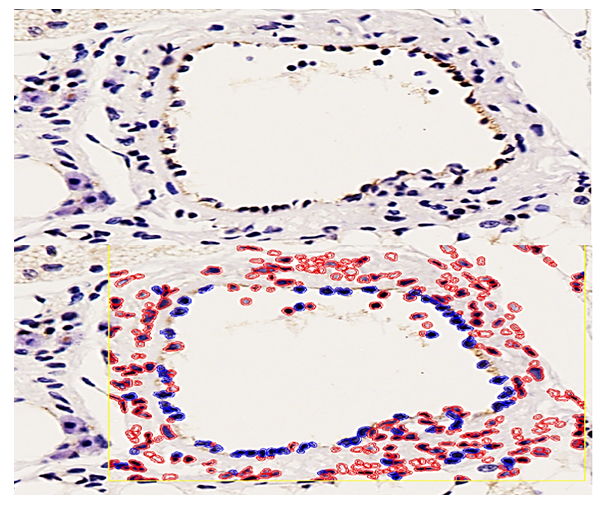 | Figure 3. Coronary artery tissue after treatment. In chronic ischemic heart disease, the arterial vessel wall shows low positive expression of the CD31 (PECAM-1) marker. Staining: DAB chromogen. Magnification: ×40. Scanned and analyzed for expression level using QuPath 0.4.0. Positively expressing cells are shown in blue |
5. Conclusions
- Thus, in the present study, the coronary artery wall’s endothelial cells were selectively damaged, with CD31 serving as an important signaling indicator, highlighting the scientific significance of our work.When the coronary endothelium is stained with the CD31 (PECAM-1) marker, it is manifested through the binding of glycoproteins, belonging to the immunoglobulin family, located at intercellular junctions of endothelial cells. This growth factor is reflected by high positive expression of the CD31 (PECAM-1) marker, indicating that, under mechanical stress on endothelial cells, impaired metabolic exchange, inflammation, and other processes causing acute vessel dilation, the glycoproteins at cell contacts have transitioned into a morphofunctionally active state. As a result, in place of endothelial cells, reparative regeneration in the intramural vessel wall occurs mainly via other mesenchymal cells, reflecting a marked reduction of endothelium and predominance of scarring. The positive reaction of the CD31 (PECAM-1) marker in this context, unlike in tumor growth, confirms that proliferative activity is primarily due to fibroblasts and macrophages in the vessel media and resident macrophages in the subendothelial layer. Clinically and morphologically, this explains the development of restenosis in coronary arteries after stenting in atherosclerosis. The main component of this process is the proliferation of intramural mesenchymal cells, leading to morphological changes such as recurrent critical stenosis, occlusion, or obliteration of the vessels (see Figure 1).Positive expression of the CD34 marker in the vessel wall during the post-atherosclerotic period reflects an increased proliferation of mesenchymal cells and an enhancement of reparative regeneration in the form of substitution. This indicates that positive CD34 expression does not represent true vascular restoration, but rather confirms that scarring predominates in the vessel wall, evidenced by the proliferation of fibroblasts, histiocytes, macrophages, and myocytes.