-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1750-1753
doi:10.5923/j.ajmms.20261604.42
Received: Mar. 12, 2026; Accepted: Apr. 3, 2026; Published: Apr. 11, 2026

Clinical and Diagnostic Aspects of Acute Adhesive Intestinal Obstruction in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLZh. B. Sattarov1, D. A. Askarov2, N. S. Khaidarov3
1Tashkent State Medical University, Tashkent, Uzbekistan
2Andijan State Medical Institute, Andijan, Uzbekistan
3Fergana Medical Institute of Public Health, Fergana, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents the results of a clinical and diagnostic evaluation conducted in 154 children diagnosed with acute adhesive intestinal obstruction (AAIO). The study analyzes the characteristic features of the clinical course of the disease and identifies the diagnostic challenges encountered during the preoperative stage. The prevalence of different forms of AAIO was determined, and the principal clinical manifestations of intestinal obstruction in pediatric patients were characterized. The diagnostic significance of instrumental investigation methods used in the identification of this pathology, including radiological, ultrasonographic, and minimally invasive techniques, is also discussed.
Keywords: Acute adhesive intestinal obstruction, Children, Diagnosis, Clinical course
Cite this paper: Zh. B. Sattarov, D. A. Askarov, N. S. Khaidarov, Clinical and Diagnostic Aspects of Acute Adhesive Intestinal Obstruction in Children, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1750-1753. doi: 10.5923/j.ajmms.20261604.42.
Article Outline
1. Introduction
- Despite significant advances in modern surgery, the problem of postoperative adhesion formation in the abdominal cavity remains highly relevant. Even when surgical procedures are performed by highly qualified specialists, the development of adhesions continues to be regarded as one of the most complex and difficult-to-prevent complications of abdominal surgery [4,13]. The presence of postoperative adhesions negatively affects not only the immediate outcomes of surgical treatment but also significantly influences the long-term quality of life of patients by limiting functional capacity and increasing the risk of recurrent complications [9].According to published studies, the incidence of adhesion formation after abdominal surgery reaches 60–80% [2,5,10]. Despite the development of various preventive measures aimed at reducing adhesion formation, a substantial decrease in the prevalence of this pathology has not yet been achieved. In the majority of patients adhesions remain clinically asymptomatic; however, approximately 3–20% of patients develop complications related to adhesive disease within five years after surgery, often leading to repeated hospitalization [1,4,11].Approximately one quarter of patients require reoperation within the first year after the initial surgical intervention. Among patients who received conservative treatment, about 12% are rehospitalized during the first year of follow-up, whereas after five years this figure may increase to 20% [3,7]. One of the most common complications after abdominal surgery is impairment of intestinal passage. According to various studies, such a condition develops in approximately 8% of patients during the first year after surgery and may reach 16% after five years [5,8,14].Based on the analysis of contemporary scientific publications, acute adhesive intestinal obstruction can be considered one of the most significant and challenging problems in modern abdominal surgery. Addressing this issue requires improvement of postoperative preventive strategies, enhancement of diagnostic accuracy, and implementation of modern treatment approaches [1,6,12]. A deeper understanding of the mechanisms underlying adhesion formation and the development of novel preventive strategies, including minimally invasive technologies and biological agents, is of considerable importance for reducing the incidence of postoperative complications [7,9,15].AimThe aim of the study was to improve the diagnostic quality of acute adhesive intestinal obstruction in children through optimization of diagnostic algorithms and systematization of clinical observations.
2. Materials and Methods
- The study was designed as a retrospective comparative cohort analysis conducted between 2020 and 2025. A total of 2,681 children hospitalized with acute surgical diseases of the abdominal cavity were analyzed.Inclusion criteria comprised children aged from 3 months to 18 years with a confirmed diagnosis of acute adhesive intestinal obstruction (AAIO) developing after previous abdominal surgery. Exclusion criteria included patients with paralytic ileus, congenital intestinal anomalies without prior surgical intervention, and incomplete clinical data.A separate clinical cohort included 154 patients (5.7%) diagnosed with AAIO. Diagnosis was established based on clinical presentation, radiological findings, and, when applicable, intraoperative verification.Patients were divided into two groups depending on the treatment strategy and observation period. The comparison group (CG) included 68 patients treated between 2020 and 2022 using a conventional management approach. The main group (MG) consisted of 86 patients treated between 2023 and 2025 using a structured diagnostic and treatment algorithm.All patients underwent standardized diagnostic evaluation, including clinical examination, laboratory tests, abdominal radiography, ultrasonography, and, when indicated, computed tomography (CT) or multislice CT (MSCT).Statistical analysis was performed using standard methods of medical statistics. Quantitative variables were expressed as mean ± standard error (M ± m). Comparative analysis between groups was performed using Student’s t-test and chi-square (χ²) test. Differences were considered statistically significant at p < 0.05.The study protocol was approved by the institutional ethics committee.Treatment OutcomesA comparative analysis of treatment outcomes demonstrated that the implementation of the proposed diagnostic and treatment algorithm in the main group was associated with improved clinical results.In the main group, a reduction in postoperative complications was observed compared to the comparison group. In addition, the duration of hospital stay was shorter in patients managed according to the structured algorithm.The need for emergency surgical intervention was also lower in the main group due to earlier and more accurate diagnosis. The rate of repeated surgical interventions and recurrence of intestinal obstruction showed a decreasing trend.Overall, the application of the algorithm contributed to optimization of treatment strategy and improved clinical outcomes. The observed differences between groups reached statistical significance (p < 0.05).Diagnostic and Treatment AlgorithmThe proposed diagnostic and treatment algorithm includes several sequential stages.At the initial stage, clinical assessment and stabilization of the patient’s condition are performed, including nasogastric decompression and correction of fluid-electrolyte imbalance.At the second stage, instrumental diagnostics are carried out. Ultrasonography and abdominal radiography are used as primary screening methods. In diagnostically unclear cases, computed tomography is performed to clarify the level and nature of intestinal obstruction.At the third stage, the treatment strategy is determined. In the absence of signs of strangulation or peritonitis, conservative therapy is initiated, including decompression, infusion therapy, and dynamic observation.Indications for surgical intervention include lack of clinical improvement, progression of symptoms, or evidence of complicated intestinal obstruction.The choice of surgical approach (laparoscopy or laparotomy) is determined individually based on clinical and instrumental findings.The age of the patients ranged from 3 months to 18 years. Analysis of sex distribution showed that the study population included 51 girls (33.1%) and 103 boys (66.9%).
|
3. Results
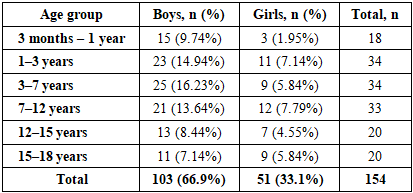
- Analysis of clinical material demonstrated a predominance of male patients. Among 154 observed cases, 103 (66.9%) occurred in boys and 51 (33.1%) in girls, indicating a higher prevalence of the pathology among male pediatric patients.The highest incidence was observed in children of early and preschool age. The age groups of 1–3 years and 3–7 years each included 34 patients (22.1%). In the 7–12-year age group, 33 cases (21.4%) were recorded.Among younger children aged 3 months to 1 year, the disease was diagnosed in 18 patients (11.7%). In older age groups (12–15 years and 15–18 years), the incidence was somewhat lower, with 20 cases (12.9%) in each group.These findings indicate that acute adhesive intestinal obstruction may occur in children of any age; however, it is most frequently observed during preschool and early school age.Diagnostic ApproachUpon admission, children presenting with signs suggestive of acute adhesive intestinal obstruction underwent a comprehensive diagnostic examination. This included assessment of the patient’s general condition, clinical evaluation, and a complete physical examination. For gastric decompression, a nasogastric tube was routinely inserted.Instrumental diagnostic methods included abdominal and chest radiography, ultrasonographic examination, and, when indicated, computed tomography (CT) or multislice computed tomography (MSCT). Laboratory investigations of blood and urine were also performed together with monitoring of acid–base balance.
4. Discussion
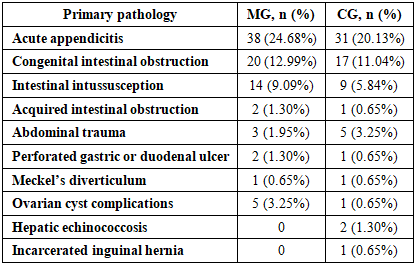
- All patients were divided into two clinical groups depending on the treatment strategy and observation period.The comparison group (CG) included 68 patients (44.2%) treated between 2020 and 2022 using the traditional management strategy. Initially, conservative therapy aimed at relieving intestinal obstruction was administered. In cases where no positive clinical dynamics were observed, emergency surgical intervention (laparotomy with adhesiolysis) was performed.The main group (MG) consisted of 86 patients (55.8%) treated between 2023 and 2025 using a diagnostic and treatment algorithm developed in the clinic. The implementation of this approach improved patient management and increased the effectiveness of therapeutic and surgical interventions.Analysis of anamnestic data showed that all children had a history of previous abdominal surgery, confirming the significant role of postoperative adhesion formation in the development of intestinal obstruction.Among diagnostic methods, computed tomography and diagnostic laparoscopy demonstrated the highest diagnostic value. CT provides detailed visualization of abdominal organs and allows identification of intestinal obstruction, while diagnostic laparoscopy enables direct evaluation of the abdominal cavity and the adhesive process.
|
5. Limitations
- The present study has several limitations. It is retrospective in nature and conducted at a single center, which may limit the generalizability of the results.In addition, the absence of randomized group allocation may introduce selection bias. Further prospective multicenter studies are required to validate the effectiveness of the proposed diagnostic and treatment algorithm.The use of a structured diagnostic and treatment algorithm significantly improves the quality of diagnosis and management of acute adhesive intestinal obstruction in children.The implementation of this approach is associated with a reduction in postoperative complications, shorter hospital stay, and decreased need for repeated surgical interventions compared to conventional treatment strategies (p < 0.05).A comprehensive diagnostic approach combining clinical assessment with modern imaging techniques remains essential for timely diagnosis and optimal treatment outcomes.
6. Conclusions
- The analysis of clinical material made it possible to identify the principal features of the development and clinical course of acute adhesive intestinal obstruction in children. The pathology may occur in patients of different age groups; however, the highest incidence was observed among children of early childhood and primary school age. In addition, a predominance of male patients was identified.Accurate diagnosis of suspected acute adhesive intestinal obstruction requires a comprehensive diagnostic approach. Clinical manifestations alone are insufficient for reliable diagnosis; therefore, instrumental diagnostic methods play a decisive role.Among them, radiological imaging and minimally invasive surgical technologies are the most informative.The implementation of modern diagnostic technologies and rational treatment strategies can significantly improve the effectiveness of medical care and reduce the risk of postoperative complications in pediatric patients.