-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1734-1740
doi:10.5923/j.ajmms.20261604.39
Received: Mar. 14, 2026; Accepted: Mar. 27, 2026; Published: Apr. 9, 2026

Contemporary Approaches to Carotid Artery Stenting in the Prevention of Ischemic Stroke: A Comprehensive Literature Review
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLZufarov M. M.1, Sultanov M. A.1, Mardonov J. N.1, 2, Makhmudov K. A.1, 2
1Republican Specialized Scientific and Practical Medical Center of Surgery named after Academician V. Vakhidov, Tashkent, Uzbekistan
2Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Mardonov J. N., Republican Specialized Scientific and Practical Medical Center of Surgery named after Academician V. Vakhidov, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Ischemic stroke remains one of the leading causes of mortality and long-term disability worldwide. Atherosclerotic stenosis of the carotid arteries plays a major role in the development of cerebrovascular ischemic events. Over the past decades, carotid artery stenting has emerged as an important minimally invasive alternative to carotid endarterectomy in selected patients with significant carotid artery stenosis. The present study provides a comprehensive analysis of contemporary literature regarding the effectiveness, safety, and technological evolution of carotid artery stenting. Particular attention is given to patient selection, procedural techniques, embolic protection systems, and modern stent designs. Current evidence indicates that carotid artery stenting demonstrates comparable long-term outcomes with surgical treatment when performed in appropriately selected patients and experienced centers. Continuous technological development and improved risk stratification strategies are expected to further enhance the safety and effectiveness of this procedure.
Keywords: Carotid artery stenosis, Carotid artery stenting, Ischemic stroke, Carotid endarterectomy, Embolic protection devices
Cite this paper: Zufarov M. M., Sultanov M. A., Mardonov J. N., Makhmudov K. A., Contemporary Approaches to Carotid Artery Stenting in the Prevention of Ischemic Stroke: A Comprehensive Literature Review, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1734-1740. doi: 10.5923/j.ajmms.20261604.39.
Article Outline
1. Introduction
- Ischemic stroke remains one of the leading causes of mortality and long-term disability worldwide and represents a major public health problem. According to global epidemiological studies, cerebrovascular diseases account for a significant proportion of cardiovascular mortality and are responsible for a substantial socioeconomic burden for healthcare systems in both developed and developing countries [1,2]. It is estimated that ischemic stroke accounts for approximately 80-85% of all cerebrovascular events and is frequently associated with atherosclerotic lesions of major extracranial arteries supplying the brain.Atherosclerotic stenosis of the carotid arteries plays a critical role in the pathogenesis of ischemic stroke. Numerous studies have demonstrated that carotid artery disease is responsible for approximately 15-20% of all ischemic strokes, particularly in elderly populations and in patients with multiple cardiovascular risk factors [3,4]. The main mechanisms leading to cerebral ischemia in patients with carotid artery stenosis include embolization of atherosclerotic plaque fragments, progressive narrowing of the arterial lumen with subsequent reduction of cerebral perfusion, and instability of vulnerable plaques prone to rupture [5]. Therefore, early detection and adequate treatment of hemodynamically significant carotid artery stenosis are essential components of modern stroke prevention strategies.For several decades, carotid endarterectomy (CEA) has been considered the standard surgical treatment for patients with significant carotid artery stenosis. The effectiveness of this procedure was confirmed in large randomized controlled trials, including the North American Symptomatic Carotid Endarterectomy Trial (NASCET) and the European Carotid Surgery Trial (ECST), which demonstrated a significant reduction in the risk of recurrent stroke in patients with symptomatic carotid stenosis greater than 70% compared with conservative medical therapy [6,7]. According to the results of these studies, surgical revascularization significantly decreases the incidence of disabling and fatal stroke in appropriately selected patients. Nevertheless, carotid endarterectomy remains associated with certain perioperative risks, including myocardial infarction, cranial nerve injury, wound complications, and systemic cardiovascular events.The rapid development of endovascular technologies over the past decades has led to the introduction of carotid artery stenting (CAS) as a minimally invasive alternative to open surgical revascularization. The first clinical experience with carotid angioplasty and stenting was reported in the 1990s, and subsequent technological improvements have significantly expanded the clinical use of this procedure [8,9]. Compared with open surgery, carotid artery stenting is associated with shorter hospital stay, reduced surgical trauma, and faster postoperative recovery.Several large randomized trials have compared carotid artery stenting with carotid endarterectomy in terms of efficacy and safety. The Carotid Revascularization Endarterectomy versus Stenting Trial (CREST) demonstrated that both treatment strategies provide comparable long-term outcomes for stroke prevention, although differences in the pattern of perioperative complications were observed [10,11]. In particular, carotid artery stenting was associated with a slightly higher risk of periprocedural stroke, whereas carotid endarterectomy was associated with a higher incidence of myocardial infarction during the early postoperative period. Similar findings were reported in the International Carotid Stenting Study (ICSS), which confirmed comparable long-term neurological outcomes between the two treatment modalities [7,8].Recent studies emphasize that the success of carotid artery stenting depends on several key factors, including appropriate patient selection, anatomical characteristics of the vascular system, operator experience, and the use of modern embolic protection systems [20,24]. Technological innovations, such as improved stent designs and advanced embolic protection devices, have significantly reduced the risk of cerebral embolization during endovascular interventions and improved procedural safety [18,21].Despite these advances, the optimal indications and patient selection criteria for carotid artery stenting remain subjects of ongoing scientific discussion. Therefore, comprehensive analysis of contemporary literature is necessary to better understand the clinical effectiveness, risk factors, and technological innovations associated with carotid artery stenting.The aim of this review was to analyze current scientific evidence regarding carotid artery stenting and to evaluate modern strategies for optimizing its application in the treatment of patients with carotid artery stenosis.Atherosclerotic stenosis of the carotid arteries leads to cerebral ischemia through embolization of plaque fragments and reduction of cerebral blood flow (Figure 1).
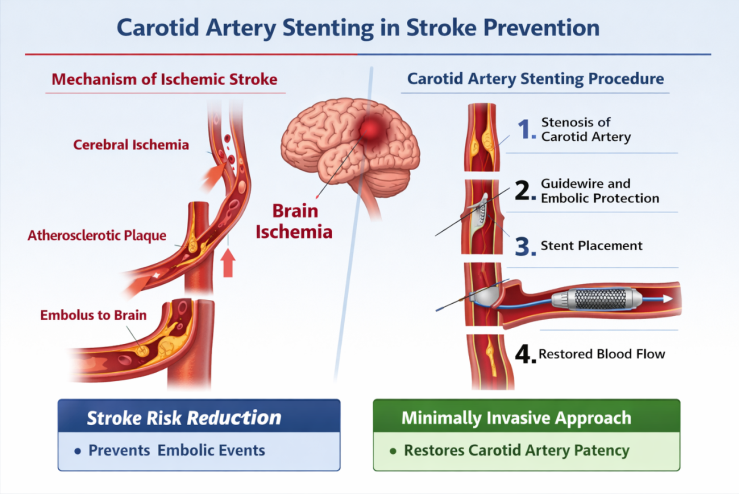 | Figure 1. Pathophysiological mechanism of ischemic stroke associated with carotid artery stenosis and the principle of carotid artery stenting (CAS) |
2. Materials and Methods
- This study was designed as a narrative literature review aimed at analyzing contemporary evidence regarding carotid artery stenting and its role in the management of carotid artery stenosis.A comprehensive search of the scientific literature was performed using major biomedical databases including PubMed, Scopus, and Web of Science. The search strategy included combinations of the following keywords: carotid artery stenosis, carotid artery stenting, carotid endarterectomy, ischemic stroke prevention, endovascular treatment, and embolic protection devices. Particular attention was paid to studies evaluating procedural outcomes, risk factors, technological developments, and comparative effectiveness of carotid revascularization methods.The literature search primarily focused on publications from 2000 to 2024, although several earlier landmark studies were also included because of their historical significance in the development of carotid revascularization strategies, such as the NASCET and ECST trials [6,7]. These trials established the fundamental role of surgical intervention in preventing recurrent ischemic stroke in patients with symptomatic carotid artery stenosis.The inclusion criteria for the analysis were:• randomized controlled trials comparing carotid artery stenting and carotid endarterectomy• systematic reviews and meta-analyses evaluating clinical outcomes of carotid revascularization• observational cohort studies analyzing predictors of complications after carotid artery stenting• international clinical guidelines and consensus statements on the management of carotid artery disease [6,12,24]Studies were excluded if they involved small case series, lacked adequate methodological description, or focused exclusively on experimental models without clinical relevance.Special emphasis was placed on major multicenter trials and large meta-analyses that significantly influenced current clinical practice. These included the CREST trial, the International Carotid Stenting Study (ICSS), and other large comparative studies evaluating the effectiveness and safety of carotid artery stenting and carotid endarterectomy [1,7,11]. In addition, several observational studies investigating patient-related and anatomical predictors of complications were analyzed in order to identify factors influencing procedural outcomes [4,25].After screening the available literature, 30 representative sources were selected for detailed analysis. These studies were chosen based on their scientific relevance, methodological quality, and impact on current clinical guidelines.The selected publications were systematically analyzed to identify key aspects of carotid artery stenting, including:• clinical effectiveness and safety of the procedure• comparison of carotid artery stenting with carotid endarterectomy• patient-related risk factors influencing procedural outcomes• anatomical predictors of complications• technological innovations in embolic protection systems and stent designThe collected data were synthesized using a qualitative analytical approach, allowing identification of major trends in the development of endovascular treatment strategies for carotid artery disease.
3. Results
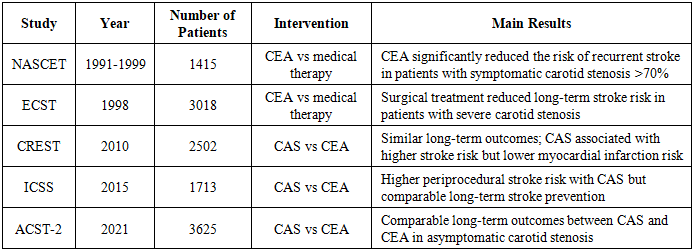
- Several large randomized clinical trials have compared carotid artery stenting and carotid endarterectomy in the prevention of ischemic stroke. The main characteristics and outcomes of these studies are summarized in Table 1.
|
3.1. Clinical Effectiveness of Carotid Artery Stenting
- Analysis of contemporary scientific literature demonstrates that carotid artery stenting (CAS) is an effective method of revascularization in patients with significant carotid artery stenosis. Over the past two decades, several large randomized clinical trials and meta-analyses have evaluated the comparative effectiveness of carotid artery stenting and carotid endarterectomy (CEA) in the prevention of ischemic stroke.One of the most influential studies in this field was the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST), which included more than 2500 patients with both symptomatic and asymptomatic carotid artery stenosis. The results demonstrated that the combined endpoint of stroke, myocardial infarction, or death did not differ significantly between CAS and CEA, indicating comparable long-term effectiveness of both treatment strategies [10,11,13].However, important differences in the pattern of perioperative complications were identified. In the CREST study, carotid artery stenting was associated with a slightly higher incidence of periprocedural stroke, whereas carotid endarterectomy showed a higher rate of myocardial infarction during the early postoperative period [10]. Similar findings were reported in the International Carotid Stenting Study (ICSS), which confirmed that long-term neurological outcomes after CAS and CEA were generally comparable [7,8].Subsequent meta-analyses combining data from multiple randomized trials also confirmed these results. In particular, pooled analyses demonstrated that carotid artery stenting is associated with comparable long-term stroke prevention but may present an increased risk of periprocedural stroke in elderly patients [27]. At the same time, the minimally invasive nature of CAS provides advantages such as shorter hospital stay, reduced surgical trauma, and faster postoperative recovery.
3.2. Patient-Related Risk Factors
- Several clinical factors have been shown to influence the outcomes of carotid artery stenting. Advanced age is considered one of the most significant predictors of procedural complications. Elderly patients frequently demonstrate severe atherosclerotic calcification of the aortic arch and carotid arteries, which increases the risk of embolic complications during endovascular manipulation [26-28].Diabetes mellitus is another important risk factor associated with adverse outcomes following carotid artery stenting. Hyperglycemia contributes to endothelial dysfunction, inflammatory activation, and accelerated atherosclerosis, which may increase the risk of restenosis and perioperative complications [10].Previous cerebrovascular events such as transient ischemic attack (TIA) or ischemic stroke also influence procedural outcomes. Patients with symptomatic carotid stenosis generally have a higher risk of recurrent stroke, making timely revascularization particularly important in this population [28].
3.3. Anatomical Predictors of Procedural Complexity
- Anatomical characteristics of the vascular system play a crucial role in determining the success of carotid artery stenting. Complex anatomical variations, including type III aortic arch configuration, severe vessel tortuosity, and heavily calcified plaques, may significantly increase the technical difficulty of the procedure [16].Calcification of the aortic arch has been associated with a higher risk of embolic complications due to increased manipulation of catheters and guidewires within the arch vessels [26]. Similarly, plaque morphology and instability are important determinants of embolic potential during carotid artery stenting.The length and severity of carotid artery stenosis also influence procedural outcomes. Long lesions or ulcerated plaques may increase the likelihood of distal embolization and procedural complications.
3.4. Procedural Factors and Operator Experience
- Operator experience and institutional procedural volume are important determinants of successful outcomes in carotid artery stenting. Studies have shown that complication rates are significantly lower in high-volume centers with experienced interventional specialists [20].The learning curve associated with carotid artery stenting plays an important role in procedural safety. Physicians performing a higher number of endovascular procedures demonstrate lower rates of perioperative complications compared with operators with limited experience.Alternative vascular access strategies, including radial access, have also demonstrated high procedural success and safety in carotid artery stenting [29].
3.5. Embolic Protection Systems
- One of the most important technological developments in carotid artery stenting has been the introduction of embolic protection devices. These systems are designed to prevent distal embolization of atherosclerotic debris during angioplasty and stent deployment.Two main categories of protection systems are currently used:• distal filter protection devices• proximal occlusion systemsSystematic reviews and meta-analyses have demonstrated that the use of embolic protection devices significantly reduces the incidence of periprocedural stroke during carotid artery stenting [5,18].Distal filter devices are widely used because they allow continuous cerebral perfusion during the procedure while capturing embolic particles released from atherosclerotic plaques. Proximal protection systems work by temporarily reversing blood flow within the carotid artery, thereby preventing embolic material from reaching the cerebral circulation.Although both methods have shown clinical effectiveness, current evidence does not clearly demonstrate superiority of one protection strategy over another [19].
3.6. Advances in Stent Design
- Modern carotid stents are typically constructed from self-expanding nitinol alloys, which provide optimal radial force and flexibility necessary for maintaining vessel patency.Three principal types of stents are commonly used in carotid artery stenting:• open-cell stents• closed-cell stents• dual-layer micromesh stentsOpen-cell stents provide greater flexibility and conformability to tortuous vessels, whereas closed-cell stents offer improved plaque coverage and potentially lower embolic risk [9].Recent studies have focused on dual-layer micromesh stents, which are designed to reduce plaque protrusion through the stent struts and thereby minimize embolic complications. Early clinical trials have demonstrated promising results with these devices, showing reduced rates of microembolization and improved procedural safety [21,30].
4. Discussion
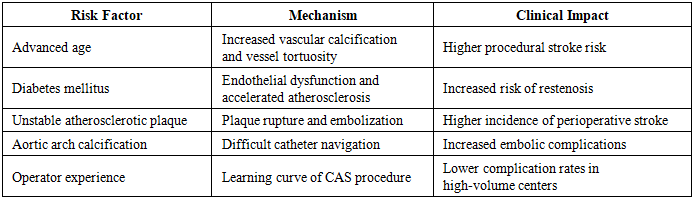
- The management of carotid artery stenosis remains one of the most important challenges in modern vascular medicine due to its direct association with ischemic stroke and chronic cerebral ischemia. The present review demonstrates that carotid artery stenting has evolved into an effective minimally invasive alternative to carotid endarterectomy in selected patients with significant carotid artery stenosis.Large randomized clinical trials have confirmed that both carotid artery stenting and carotid endarterectomy provide comparable long-term protection against ischemic stroke [11,23]. However, differences in perioperative complications have been consistently observed. While carotid artery stenting is associated with a slightly increased risk of periprocedural stroke, carotid endarterectomy demonstrates a higher incidence of myocardial infarction in the early postoperative period [14,23]. These findings emphasize the importance of individualized treatment strategies based on patient characteristics and risk profiles.One of the key factors influencing the outcomes of carotid artery stenting is patient selection. Numerous studies have demonstrated that advanced age significantly increases the risk of procedural complications, particularly due to extensive atherosclerotic calcification of the aortic arch and carotid arteries [26,27]. Elderly patients frequently present with complex vascular anatomy, including tortuous vessels and calcified plaques, which increase the risk of embolization during catheter manipulation. Consequently, careful preoperative imaging and patient stratification remain essential components of successful endovascular treatment.Another important consideration is the presence of comorbid conditions, particularly diabetes mellitus. Chronic hyperglycemia contributes to endothelial dysfunction, vascular inflammation, and accelerated progression of atherosclerosis, which may increase the risk of restenosis and perioperative complications following carotid artery stenting [10]. These findings highlight the need for comprehensive management of cardiovascular risk factors in patients undergoing carotid revascularization.Multiple clinical and anatomical factors may influence the safety and effectiveness of carotid artery stenting. The most important risk factors associated with procedural complications are presented in Table 2.
|
5. Conclusions
- Carotid artery stenosis remains one of the most significant risk factors for ischemic stroke and chronic cerebral ischemia. Early identification and appropriate management of this condition are essential components of modern strategies aimed at reducing cerebrovascular morbidity and mortality. The analysis of contemporary scientific literature demonstrates that carotid artery stenting has become an important minimally invasive alternative to carotid endarterectomy for the treatment of patients with significant carotid artery stenosis.Evidence from large randomized clinical trials and meta-analyses indicates that carotid artery stenting provides comparable long-term outcomes in stroke prevention when compared with surgical revascularization. However, differences in perioperative complications emphasize the need for careful patient selection and individualized treatment planning.Several factors significantly influence the safety and effectiveness of carotid artery stenting. These include patient-related characteristics such as advanced age and comorbidities, anatomical features of the aortic arch and carotid arteries, as well as procedural factors including operator experience and the use of embolic protection systems. Modern technological advancements, particularly in the development of embolic protection devices and improved stent designs, have contributed to a significant reduction in procedural complications.At the same time, ongoing improvements in imaging techniques and risk stratification strategies are expected to further optimize the selection of patients for carotid revascularization. Future research should focus on the development of advanced endovascular technologies, refinement of procedural techniques, and integration of personalized approaches to the management of carotid artery disease.In conclusion, carotid artery stenting represents a safe and effective treatment modality for selected patients with carotid artery stenosis. Continued technological progress, improved patient selection, and increasing operator experience are expected to further enhance the clinical outcomes of this procedure and contribute to more effective prevention of ischemic stroke.