-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1724-1727
doi:10.5923/j.ajmms.20261604.37
Received: Mar. 5, 2026; Accepted: Mar. 23, 2026; Published: Apr. 9, 2026

Prosthodontic Rehabilitation with Removable Partial Dentures in Patients after Bariatric Surgery: A Clinical Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLT. F. Salavatova, A. N. Akbarov
Department of Prosthetic Dentistry, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: T. F. Salavatova, Department of Prosthetic Dentistry, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The increasing prevalence of bariatric surgery has led to a growing number of patients requiring prosthodontic rehabilitation under altered metabolic and microcirculatory conditions. The objective of this study was to optimize removable partial denture treatment in patients with a history of bariatric surgery. The study included 90 individuals, 60 of whom had undergone bariatric procedures. The main group (n=30) received comprehensive treatment including removable partial acrylic dentures with a soft silicone liner and microcirculatory support, while the comparison group (n=30) underwent conventional prosthodontic management. The control group consisted of 30 systemically healthy individuals. Clinical evaluation included mucosal hyperemia, number of traumatic pressure areas, pain intensity (VAS), and epithelial resistance. Follow-up lasted 12 months. Significant reduction in hyperemia and pressure areas was observed in the comprehensive group after 3 months (p<0.001). After 12 months, clinical indicators approached control values. The combined mechanical and endothelial-support approach demonstrated improved adaptive outcomes in post-bariatric patients.
Keywords: Removable partial denture, Bariatric surgery, Oral mucosa, Soft liner, Endothelial dysfunction
Cite this paper: T. F. Salavatova, A. N. Akbarov, Prosthodontic Rehabilitation with Removable Partial Dentures in Patients after Bariatric Surgery: A Clinical Study, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1724-1727. doi: 10.5923/j.ajmms.20261604.37.
Article Outline
1. Introduction
- Bariatric surgery is currently considered one of the most effective treatments for morbid obesity and metabolic syndrome [4,11,12]. Long-term results of mini-gastric bypass demonstrate sustained weight loss and carbohydrate metabolism compensation [3,9], but are accompanied by systemic metabolic changes, including changes in nutritional status [8].According to current data, patients undergoing bariatric surgery may experience vascular and neurological complications [2,6], as well as changes in somatic and functional status, affecting quality of life [7,10].Metabolic and vascular disorders can affect the condition of peripheral tissues, including the oral mucosa. The literature emphasizes the need for a comprehensive, interdisciplinary approach to patient care after bariatric surgery [8].
2. Methods
- The study was a prospective comparative observational study. The follow-up period was 12 months. Ninety patients (45.3±4.6 years) were included in the study. No gender differences were found between the groups (p>0.05).The study was conducted at the clinical site of the Department of Orthopedic Dentistry at Tashkent State Medical University. All patients signed voluntary informed consent to participate in the study and the processing of their personal data.The patients were divided into three groups of 30 each: Group I (main) - patients after bariatric surgery (gastric bypass), prosthetics using a soft silicone liner; Group II (comparison) - patients after bariatric surgery, standard prosthetics; the control group - generally healthy patients with no history of bariatric surgery.The average body mass index (BMI) at study inclusion was 34.4±1.8 kg/m² in Group I and 34.2±1.6 kg/m² in Group II.Inclusion and exclusion criteria were based on clinical guidelines [4,11].Prosthodontic treatment method. All cases utilized removable partial dentures with an acrylic base, manufactured using standard laboratory technology. In Group I, an elastic silicone liner 1.5-2.0 mm thick was applied to the inner surface of the base (temporary relining method) for a period of 3-6 months. Patients in Group I additionally received L-arginine hydrochloride to correct endothelial dysfunction and enhance microcirculatory regulation. The medication was administered parenterally in a standard therapeutic dose according to the manufacturer's protocol for 10-14 days, with repeat courses prescribed when clinically indicated. Patients were monitored monthly during the first year of follow-up.Clinical and functional assessment. The condition of the mucous membrane was assessed upon initial prosthesis placement and after 3, 6, and 12 months.Mucosa hyperemia was assessed visually under standard dental lighting. A four-point scale (0-4 points) was used: 0 - no hyperemia; 1 - mild diffuse hyperemia; 2 - moderate hyperemia; 3 - severe hyperemia; 4 - hyperemia with erosive-macerative changes. The assessment was performed by a single, pre-calibrated examiner.A functional test with pressure-indicating paste was used to identify areas of excessive load. The denture was inserted into the oral cavity after applying the indicator layer. The patient performed functional movements (chewing, articulation). After removing the denture, areas of thinning of the indicator layer, reflecting areas of increased pressure, were recorded. The number of such zones was recorded numerically.Pain intensity was assessed using a visual analog scale (VAS) from 0 to 10 points. The patient indicated the degree of discomfort during functional load in the area of the denture bed. The resistance of the epithelium to mechanical stress was assessed by graduated palpation of the mucosa with a blunt instrument applying uniform pressure, using a rating scale: 0 - no reaction; 1 - mild hyperemia without pain; 2 - hyperemia with moderate discomfort; 3 - severe hyperemia and pain; 4 - superficial erosive changes.All patients received oral hygiene instructions. Follow-up visits were conducted at regular intervals. All patients signed voluntary informed consent to participate in the study. The study was conducted in accordance with bioethical principles and current legislation.Statistical analysis was performed after checking for normal distribution (Shapiro-Wilk test). Paired and unpaired t-tests were used. Differences were considered significant at p < 0.05.
3. Results
3.1. Baseline
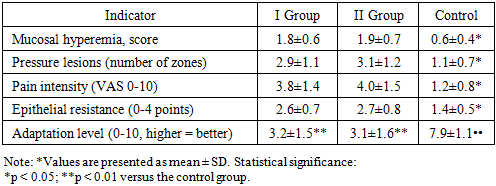
- During the initial examination, patients with a history of bariatric surgery showed pronounced signs of functional failure of the mucous membrane of the prosthetic bed. The average hyperemia score was 1.8 ± 0.6 points in Group I and 1.9 ± 0.7 points in Group II, which significantly exceeded the values in the control group (0.6 ± 0.4; p < 0.001). The number of local pressure zones reached 2.9 ± 1.1 and 3.1 ± 1.2, respectively, versus 1.1 ± 0.7 in the control. The pain intensity according to the VAS scale was 3.8 ± 1.4 and 4.0 ± 1.5 points, which is more than three times higher than the control values (1.2 ± 0.8; p < 0.001). Epithelial resistance to mechanical stress was also reduced (2.6±0.7 and 2.7±0.8 versus 1.4±0.5; p<0.001), indicating increased tissue reactivity and decreased barrier function of the oral mucosa. Pain intensity was more than three times higher (Table 1).
|
3.2. After 3 Months
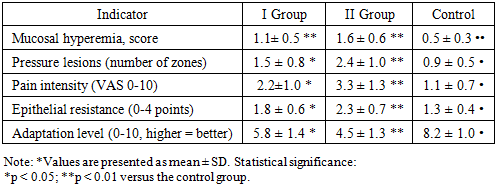
- After 3 months of observation, positive dynamics were noted in all groups; however, the degree of reduction in the severity of pathological manifestations varied significantly. In the complex management group, hyperemia decreased to 1.1±0.5 points, while in the standard management group it remained at 1.6±0.6 (p<0.001). The number of pressure zones decreased to 1.5±0.8 in Group I (a decrease of more than 48% from baseline) and to 2.4±1.0 in Group II (a decrease of approximately 23%). Pain decreased to 2.2±1.0 versus 3.3±1.3 (p<0.05) (Table 2).
|
3.3. After 6 Months
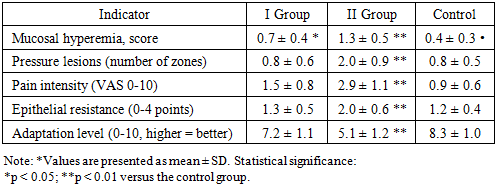
- By the sixth month of observation, the differences between the groups became more pronounced. In Group I, hyperemia decreased to 0.7±0.4 points, indicating restoration of mucosal trophism. In Group II, this indicator remained significantly higher (1.3±0.5; p<0.001). The number of pressure zones in Group I decreased to 0.8±0.6, while in Group II it remained at 2.0±0.9 (Table 3).
|
3.4. After 12 Months
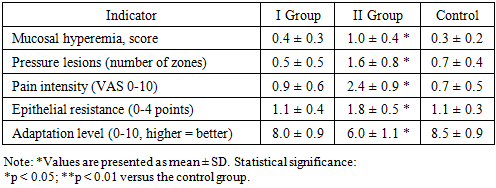
- After 12 months of orthopedic rehabilitation, the comprehensive management group demonstrated almost complete clinical stabilization of the denture bed. Mucosal hyperemia decreased to 0.4±0.3 points, the number of pressure zones to 0.5±0.5, and pain intensity to 0.9±0.6. These parameters did not differ statistically significantly from those in the control group (Table 4).
|
4. Discussion
- The obtained data are consistent with previously published studies demonstrating systemic metabolic changes after bariatric surgery [11,12]. Impaired nutritional status and microvascular regulation [8] can reduce the mucosal resistance to mechanical stress.The risk of postoperative complications and systemic reactions [1,2,14] justifies the need for long-term observation. The impact of bariatric surgery on quality of life [7,10] emphasizes the importance of adaptive processes.The use of a soft silicone pad reduces peak pressure values and attenuates the severity of the inflammatory response early on. The study has several limitations, including a relatively small sample size and a single-center design.
5. Conclusions
- Patients after bariatric surgery are characterized by reduced mucosal tolerance to functional stress. The use of a soft silicone pad provides a statistically significant reduction in hyperemia, the number of local pressure zones, and pain. After 12 months, mucosal condition indicators in the study group did not differ from the control values. A comprehensive approach to prosthodontic rehabilitation in post-bariatric patients should include multidisciplinary monitoring and individualized prevention of mucosal overload [5,13].