-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1719-1723
doi:10.5923/j.ajmms.20261604.36
Received: Mar. 2, 2026; Accepted: Mar. 22, 2026; Published: Apr. 9, 2026

Clinical and Syndromological Features of Anxiety and Depressive Disorders in Subclinical and Overt Hypothyroidism
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBotirbek Vosikov, Shakhnoza Magzumova
Department of Psychiatry and Narcology, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Botirbek Vosikov, Department of Psychiatry and Narcology, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The present study aimed to identify and analyze the clinical and syndromological characteristics of anxiety and depressive disorders in patients with subclinical and overt hypothyroidism. Statistically significant between-group differences were found, with a consistent increase in symptom severity along the gradient: euthyroidism - subclinical hypothyroidism - overt hypothyroidism. Cluster analysis demonstrated the predominance of neurovegetative-somatic components of anxiety and depression in the overt form of the disease, whereas cognitive-affective components prevailed in the control group. Patients with subclinical hypothyroidism occupied an intermediate position in both quantitative measures and symptom structure. Thyroid status exerts a significant influence on the severity and syndromological structure of anxiety-depressive disorders. These findings highlight the need for comprehensive psychopathological assessment of patients with different forms of hypothyroidism to improve diagnostic accuracy and optimize clinical management.
Keywords: Hypothyroidism, Subclinical hypothyroidism, Depression, Anxiety, Affective disorders, Syndromological structure
Cite this paper: Botirbek Vosikov, Shakhnoza Magzumova, Clinical and Syndromological Features of Anxiety and Depressive Disorders in Subclinical and Overt Hypothyroidism, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1719-1723. doi: 10.5923/j.ajmms.20261604.36.
1. Introduction
- Affective disorders remain one of the leading causes of reduced quality of life and social maladaptation among the working-age population, as emphasized in contemporary epidemiological studies and World Health Organization reports [1], [2], [3]. Over recent decades, increasing attention has been paid to their comorbidity with somatic pathology, particularly thyroid diseases, which have a substantial impact on mental functioning [4], [5], [6]. Hypothyroidism, both overt and subclinical, is associated with alterations in emotional regulation, cognition, and behavioral activity, as reflected in modern reviews and clinical-epidemiological studies [7], [8].The pathogenetic link between thyroid dysfunction and anxiety-depressive symptomatology is mediated by the effects of thyroid hormones on brain neurotransmitter systems – primarily serotonergic and noradrenergic pathways – as well as on central regulatory mechanisms of the hypothalamic-pituitary-thyroid axis [9], [10], [11]. Neuroimmune and inflammatory mechanisms may also contribute to the development of depressive symptoms in the context of somatic comorbidity [12], [13], [14]. The interaction between depression and chronic somatic diseases is conceptualized within the biopsychosocial model, which is reflected in integrative approaches to the management of patients with comorbid conditions and in collaborative care frameworks [15], [16], [17].Subclinical hypothyroidism poses challenges, as hormonal changes are modest and are often regarded as a laboratory finding without clear clinical significance [18], [19]. Nevertheless, the European Thyroid Association guidelines emphasize the need for clinical assessment of symptoms even when thyroid function parameters are borderline [20]. Contemporary evidence also points to heterogeneity of clinical manifestations and difficulties in interpreting symptoms in subclinical hypothyroidism, including depressive features reported in population-based and meta-analytic studies [21], [22], [23], [24]. This creates a risk of underdiagnosis of affective disorders or their misattribution to primary psychiatric illness, including the potential influence of diagnostic “labeling” and symptom perception biases [25], [26].Despite the growing body of research on the comorbidity of hypothyroidism and depression, the clinical and syndromological differences in anxiety-depressive disorders between subclinical and overt forms of the disease remain insufficiently studied; the literature is dominated by reviews and meta-analyses lacking detailed syndromic typology [22], [23], [24], [27] Clarifying the clinical and syndromological characteristics of anxiety-depressive disorders across different forms of hypothyroidism is essential for early detection, differential evaluation, and the development of stratified management approaches, including the debated role of replacement therapy and expert consensus recommendations in subclinical hypothyroidism [20], [28], [29].Against this background, this study aimed to identify and analyze the clinical and syndromological characteristics of anxiety and depressive disorders in patients with subclinical and overt hypothyroidism.
2. Materials and Methods
- The study included 159 patients aged 18-60 years with affective disorders who were examined in 2023-2025. Patients were divided into three groups: 41 patients with overt hypothyroidism, 68 with subclinical hypothyroidism, and 50 with euthyroid status (control group). Thyroid dysfunction was diagnosed based on serum thyroid-stimulating hormone (TSH) and free thyroxine (fT4) levels. The severity of affective symptoms was assessed using the HADS, HARS, HDRS-17, and CGI-S scales. Comparative analysis of quantitative indicators and a cluster analysis of the structure of anxiety and depressive symptomatology were performed. Statistical analysis included parametric and non-parametric methods; differences were considered significant at p < 0.05.For structural analysis of anxiety and depressive symptomatology, a cluster (domain-based) approach was used with a priori identification of two components: (1) neurovegetative-somatic and (2) cognitive-affective. Cluster scores were calculated as the mean (or sum) of points for the corresponding items of the HARS and HDRS-17 scales. For the HARS, the neurovegetative-somatic cluster included items reflecting somatovegetative manifestations of anxiety (cardiovascular, respiratory, gastrointestinal, urogenital, autonomic symptoms, etc.), whereas the cognitive-affective cluster included items related to psychic anxiety, tension, fears, and associated cognitive phenomena. For the HDRS-17, the neurovegetative-somatic cluster included sleep disturbances, somatic symptoms, psychomotor retardation/agitation, and reduced activity, while the cognitive–affective cluster included depressed mood, feelings of guilt, suicidal thoughts, and others.
3. Results
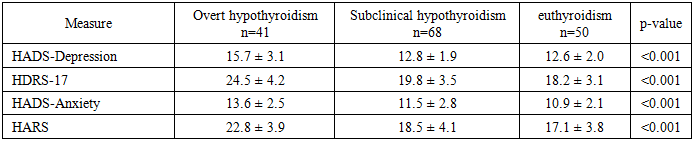
- Comparative analysis of anxiety–depressive symptom severity across the study groups revealed statistically significant differences on all applied scales (p < 0.001). A consistent trend toward increasing severity of affective disturbances was observed along the gradient: control group < subclinical hypothyroidism < overt hypothyroidism.In the overt hypothyroidism group, mean scores were 15.7 ± 3.1 on the HADS-Depression subscale, 24.5 ± 4.2 on the HDRS-17, 13.6 ± 2.5 on the HADS-Anxiety subscale, and 22.8 ± 3.9 on the HARS. The median CGI-S score was 5.0 [5.0; 6.0], indicating a predominance of moderately severe affective disorders.In the subclinical hypothyroidism group, the scores were lower: HADS-Depression 12.8 ± 1.9; HDRS-17 19.8 ± 3.5; HADS-Anxiety 11.5 ± 2.8; and HARS 18.5 ± 4.1. In the control group, the corresponding values were 12.6 ± 2.0; 18.2 ± 3.1; 10.9 ± 2.1; and 17.1 ± 3.8. Between-group differences were statistically significant (p < 0.001).Cluster (domain-based) analysis of anxiety symptoms (HARS) demonstrated significant differences in symptom structure. In the overt hypothyroidism group, the neurovegetative–somatic cluster (2.6 ± 0.4) exceeded the cognitive–affective cluster (1.9 ± 0.5). In the control group, the opposite pattern was observed: the somatic component was 1.7 ± 0.5, whereas the cognitive–affective component was 2.3 ± 0.6. The subclinical hypothyroidism group occupied an intermediate position (2.0 ± 0.5 and 2.1 ± 0.5, respectively). The differences were statistically significant (p < 0.001 for the somatic cluster and p < 0.01 for the cognitive–affective cluster).A similar analysis using the HDRS-17 showed that, in overt hypothyroidism, the neurovegetative–somatic cluster of depression (2.8 ± 0.5) exceeded the cognitive–affective cluster (1.9 ± 0.7). In the control group, by contrast, the cognitive–affective component (2.2 ± 0.6) was more pronounced than the somatic component (1.8 ± 0.5). In subclinical hypothyroidism, the indicators were intermediate (2.1 ± 0.6 and 1.8 ± 0.6, respectively). The differences were statistically significant (p < 0.001 and p < 0.01).Thus, both the quantitative indices and the structural profile of affective disturbances differed depending on patients’ thyroid status.
|
|

|

4. Discussion
- Affective disorders frequently accompany thyroid dysfunction and may modify the clinical presentation of hypothyroidism, complicating diagnosis and the choice of therapeutic strategy [5], [30]. The present findings demonstrate statistically significant differences in the severity and structure of anxiety–depressive disorders in patients with different forms of hypothyroidism. The observed gradient of affective symptom severity (overt hypothyroidism > subclinical hypothyroidism > euthyroidism) is consistent with evidence from systematic reviews and meta-analyses linking thyroid dysfunction to depressive symptoms [22], [23], [24], [27], as well as with population-based observations in individuals with high-normal/elevated TSH levels [31].It is well established that thyroxine (T4) and triiodothyronine (T3) exert modulatory effects on serotonergic transmission and central regulatory mechanisms, which underlies their role in the pathogenesis of depressive disorders [9], [10], [32]. Reduced thyroid function is associated with affective symptoms of varying severity, as supported by population-based and clinical studies in overt hypothyroidism and subclinical forms [6], [33], [34].Attention should be given to the identified structure of anxiety symptomatology. The predominance of neurovegetative-somatic components of anxiety in overt hypothyroidism may align with reports of neuropsychiatric involvement and somatization in thyroid insufficiency, including descriptions of “brain fog” and neurocognitive complaints [7], [8], [35]. This pattern may reflect different mechanisms underlying anxiety states: in thyroid insufficiency, anxiety may be mediated predominantly through somatovegetative manifestations, whereas in the absence of endocrine dysfunction it may have a more psychogenic character [5], [36].Analysis of depressive symptoms using the HDRS-17 revealed a similar trend: in overt hypothyroidism, neurovegetative-somatic components predominated, while in the control group cognitive-affective features were more pronounced. Comparable phenomenological observations have been reported in clinical and population-based studies examining depressive symptoms in hypothyroidism and subclinical dysfunction [6], [33], [37]. This finding is indirectly consistent with biologically determined models of depression in the context of marked somatic (endocrine) insufficiency, including discussions of interactions between the thyroid and stress axes [38], [39], as well as data on functional brain changes associated with hypothyroidism [40].In subclinical hypothyroidism, by contrast, the structure of disorders was intermediate and less differentiated, which may reflect a combination of biological and contextual mechanisms; this is consistent with the heterogeneity of findings on subclinical dysfunction in the literature [21], [23], [24]. Subclinical hypothyroidism remains a matter of debate regarding the clinical significance of affective disturbances and the appropriateness of early intervention, as reflected both in guidelines and in critical commentaries [18], [19], [20].The present data confirm that even in the absence of overt hormonal deficiency, clinically significant anxiety-depressive symptoms may develop and differ from those observed in euthyroidism, which corresponds to conclusions from meta-analyses and population-based studies [22], [24], [37]. From a practical standpoint, this is important given the mixed evidence regarding the effects of levothyroxine on depressive symptoms and quality of life in subclinical hypothyroidism [28], [41], [42].Overall, the identified clinical and syndromological differences suggest that affective disorders in overt hypothyroidism can be conceptualized as predominantly somatized forms of depression and anxiety with a marked neurovegetative component, whereas subclinical hypothyroidism is characterized by a more heterogeneous structure with moderately expressed symptoms [7], [27], [35]. These features should be considered in diagnostic evaluation and the development of individualized treatment strategies, including multidisciplinary models for managing patients with psychosomatic comorbidity [15], [16], [17], [43].
5. Conclusions
- The present study demonstrated significant quantitative and structural differences in anxiety and depressive disorders in patients with subclinical and overt hypothyroidism compared with individuals with euthyroid status. A statistically significant gradient in affective symptom severity was identified (p < 0.001), characterized by a progressive increase in severity along the continuum: euthyroidism < subclinical hypothyroidism < overt hypothyroidism.In overt hypothyroidism, affective disturbances were more intense and were characterized by a predominance of neurovegetative–somatic components in both the anxiety and depressive symptom profiles. In this group, the depressive syndrome was accompanied by marked psychomotor retardation, sleep disturbances, reduced activity, and prominent somatic symptoms, reflecting a biologically driven pattern of affective pathology in the context of pronounced thyroid hormone deficiency.In subclinical hypothyroidism, clinically significant anxiety–depressive symptomatology was observed, but the symptom structure was less differentiated and more heterogeneous. Quantitative indices occupied an intermediate position between overt hypothyroidism and the control group, and the balance between somatic and cognitive–affective components did not show a clear dominance of either cluster.In the euthyroid control group, cognitive–affective components of anxiety and depressive disorders predominated, consistent with the profile of primary affective disturbances without a substantial somatic contribution.Overall, thyroid status exerts a substantial influence not only on the severity but also on the syndromological structure of anxiety–depressive disorders. The identified clinical and syndromological differences are diagnostically relevant and may support more accurate differential assessment of affective states in patients with different forms of hypothyroidism.