-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1710-1714
doi:10.5923/j.ajmms.20261604.34
Received: Feb. 11, 2026; Accepted: Mar. 7, 2026; Published: Apr. 9, 2026

PRP Therapy of Hypertrophic Gingivitis in Pregnant Women with Pregnancy Pathology: A Case Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdilova Aziza Shuxrat qizi
Tashkent State Medical University, Uzbekistan
Correspondence to: Adilova Aziza Shuxrat qizi, Tashkent State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study evaluated the clinical effectiveness of platelet-rich plasma (PRP) therapy as an adjunct to conventional periodontal treatment in pregnant women with pregnancy-associated hypertrophic gingivitis (PHG). A controlled clinical pilot study was conducted in 52 pregnant women diagnosed with PHG, who were divided into two comparable groups: a main group receiving conventional periodontal therapy plus PRP injections and a control group receiving conventional treatment alone. Clinical effectiveness was assessed using the Papillary-Marginal-Alveolar (PMA) index, the Simplified Oral Hygiene Index (OHI-S), and gingival bleeding severity before and after therapy. In the main group, a significantly greater reduction in inflammatory indices was observed compared with the control group. The PMA index decreased from 56.0 ± 8.4% to 24.3 ± 6.1% in the main group and from 55.1 ± 7.9% to 37.8 ± 7.0% in the control group (p < 0.05). OHI-S values improved from 2.9 ± 0.4 to 1.5 ± 0.3 and from 2.8 ± 0.5 to 2.1 ± 0.4, respectively (p < 0.05). These findings suggest that PRP therapy may enhance the effectiveness of conventional treatment in PHG by reducing inflammation and improving periodontal status. PRP administration in the presented clinical case was performed postpartum, whereas in the broader study protocol PRP was administered during the second trimester in selected patients and again 30 days after delivery when clinically indicated.
Keywords: Platelet-rich plasma (PRP), PRP therapy, Pregnancy-associated hypertrophic gingivitis (PHG), Autologous platelet-rich plasma (APRP), Periodontal inflammation, Oral hygiene index (OHI-S)
Cite this paper: Adilova Aziza Shuxrat qizi, PRP Therapy of Hypertrophic Gingivitis in Pregnant Women with Pregnancy Pathology: A Case Study, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1710-1714. doi: 10.5923/j.ajmms.20261604.34.
Article Outline
1. Introduction
- Pregnancy-associated hypertrophic gingivitis (PHG) is a common inflammatory condition of the gingival tissues that develops or worsens during gestation under the influence of hormonal, microbial, and local hygienic factors [3,4,14]. Gingival inflammation during pregnancy has been reported in a substantial proportion of pregnant women, although prevalence estimates vary widely across studies depending on diagnostic criteria, population characteristics, oral hygiene status, and study design [3,4]. Because PHG may impair quality of life, complicate oral hygiene, and aggravate pre-existing periodontal pathology, effective and safe therapeutic approaches are needed [4,10,14].Conventional treatment of pregnancy-associated gingival inflammation includes professional oral hygiene, elimination of local irritants, individualized hygiene instruction, and anti-inflammatory supportive care [4,14]. However, in moderate and severe forms of PHG, clinical improvement may be slow, incomplete, or unstable, especially in women with pregnancy-related somatic or obstetric complications [4,10].Platelet-rich plasma (PRP) is an autologous biological product enriched with platelets and growth factors that may promote tissue repair, angiogenesis, collagen synthesis, and modulation of inflammation [6,7,9,11,12]. PRP has been widely used in oral surgery, regenerative dentistry, and periodontology [6–9,17–20]. Nevertheless, its role in the treatment of pregnancy-associated hypertrophic gingivitis remains insufficiently studied. The available literature includes only limited evidence directly focused on pregnant patients, although preliminary findings suggest a beneficial effect of PRP on gingival health and inflammatory status in this population [2,15,16].Periodontal inflammation in pregnancy is also of broader clinical relevance because periodontal disease has been discussed as a possible contributing factor in adverse pregnancy outcomes, including placental dysfunction, preeclampsia, and preterm birth [4,10]. This increases the importance of identifying local treatment approaches that are both effective and biologically safe.The aim of this study was to evaluate the clinical effectiveness of PRP therapy as an adjunct to conventional periodontal treatment in patients with pregnancy-associated hypertrophic gingivitis. The study hypothesis was that adjunctive PRP therapy would result in significantly greater clinical improvement in periodontal inflammatory indices than conventional treatment alone.
2. Materials and Methods
- Study design. This investigation was designed as a controlled clinical pilot study with parallel comparison of two treatment groups. In addition, one representative severe clinical case was analyzed descriptively to illustrate the practical application of PRP therapy [15,16].Study setting. The study was conducted at the pathology department of the maternity clinic affiliated with Tashkent State Medical University.Participants. A total of 52 pregnant women diagnosed with pregnancy-associated hypertrophic gingivitis were included in the study. After clinical screening and application of eligibility criteria, the participants were divided into two comparable groups: the main group (n = 26), which received conventional periodontal treatment plus PRP therapy, and the control group (n = 26), which received conventional periodontal treatment only. The groups were comparable at baseline in terms of age, gestational period, severity of gingival inflammation, gingival bleeding, PMA index, and oral hygiene status.Eligibility criteria. Inclusion criteria comprised confirmed pregnancy, diagnosis of pregnancy-associated hypertrophic gingivitis, informed voluntary consent to participate, and ability to attend clinical follow-up. Exclusion criteria included HIV infection, COVID-19 or other acute viral infection, viral hepatitis, malignant neoplasms, multiple pregnancy, severe obstetric complications requiring urgent non-dental management, severe iron-deficiency anemia (hemoglobin < 90 g/L), arterial hypotension (systolic blood pressure < 100 mmHg), acute or chronic inflammatory disease associated with body temperature > 37.2°C, and severe psychiatric disorders.Clinical examination. All participants underwent standardized dental and periodontal examination. The following parameters were assessed before and after treatment: gingival enlargement and visual signs of inflammation, gingival bleeding, gingival tenderness, the Papillary-Marginal-Alveolar (PMA) index, and the Simplified Oral Hygiene Index (OHI-S) [14–16]. OHI-S values were interpreted as follows: 0.0–1.2, good oral hygiene; 1.3–3.0, satisfactory oral hygiene; and 3.1–6.0, unsatisfactory oral hygiene.Treatment protocol. All patients received conventional periodontal therapy, including professional oral hygiene, removal of plaque-retentive factors, individualized oral hygiene instruction, and local anti-inflammatory periodontal care. Patients in the main group additionally received local PRP injections into affected gingival tissues.PRP preparation. PRP was prepared from 17 mL of autologous venous blood collected from the cubital vein under sterile conditions. The blood was distributed into two 8.5 mL tubes: a vacuum tube containing sodium heparin and a specialized PRP tube containing separation gel and highly purified sodium heparin. The protocol was based on established principles of autologous platelet concentrate preparation and Plasmolifting™ technology described in the literature [11–13].
3. Research Results
- A detailed analysis was performed for a clinical case of severe PHG. Patient U.M.M., born in 2002, presented with severe gingival inflammation during her fourth pregnancy at 38 weeks of gestation. The patient reported that her first pregnancy occurred at the age of 19 years. A concomitant disease of grade I iron-deficiency anemia was diagnosed.
 | Photo 1. Caries indicator staining |
 | Photo 2. after professional cleaning |
|

|

|

4. Discussion
- The clinical results obtained in the present study demonstrated a positive therapeutic effect of platelet-rich plasma (PRP) therapy in patients with pregnancy-associated hypertrophic gingivitis. The dynamics of periodontal indices before and after treatment in the main group are presented in Graph 1, which illustrates a significant reduction in inflammatory manifestations following PRP therapy.
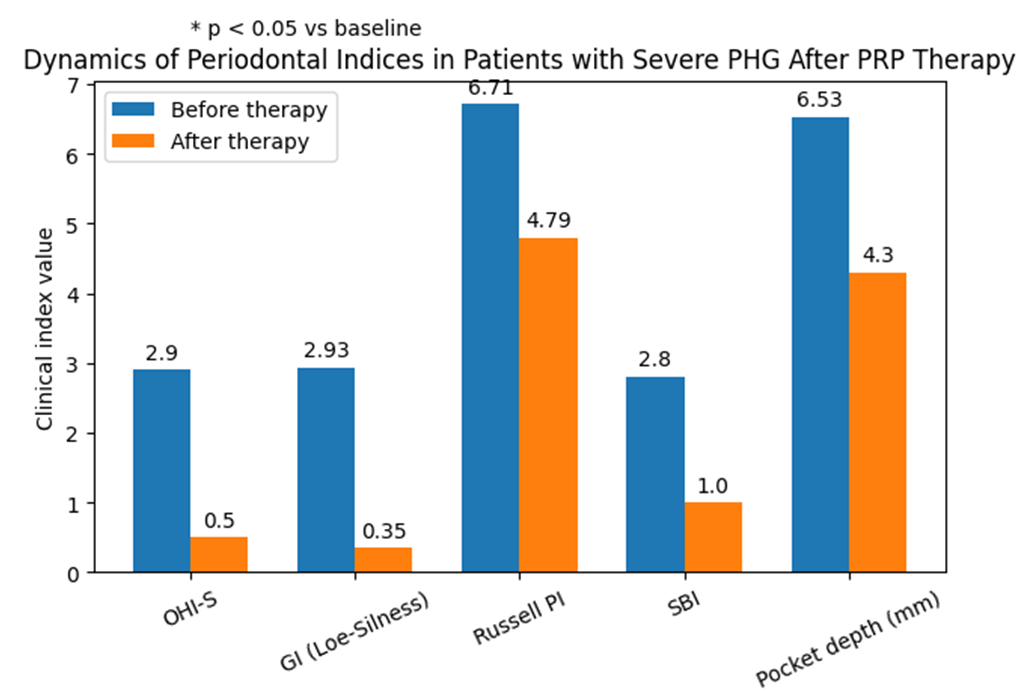 | Graph 1 |
5. Conclusions
- Adjunctive platelet-rich plasma therapy demonstrated superior clinical effectiveness compared with conventional periodontal treatment alone in patients with pregnancy-associated hypertrophic gingivitis. The use of PRP was associated with greater reductions in PMA index, gingival bleeding, and OHI-S values, indicating a more pronounced resolution of gingival inflammation and improved oral hygiene status.The study supports the potential role of PRP as a safe and promising adjunctive method in the management of moderate and severe PHG. In the overall study, PRP was administered during the second trimester and, when indicated, again 30 days postpartum; in the presented severe clinical case, PRP was administered postpartum only. Despite the encouraging clinical results, larger controlled studies are needed before firm clinical recommendations can be established.