-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1705-1709
doi:10.5923/j.ajmms.20261604.33
Received: Mar. 11, 2026; Accepted: Mar. 29, 2026; Published: Apr. 8, 2026

Selection of an Alternative Endoscopic Treatment Method for Primary High-Grade Vesicoureteral Reflux in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRaxmatullayev Akmal Abadbekovich, Ergashev Muhammadjon Tursunovich
Department of Pediatric Surgery, Urology, Pediatric Urology, Anesthesiology and Resuscitation, Pediatric Anesthesiology and Resuscitation, Tashkent State Medical University, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective. To improve the effectiveness of endoscopic correction in children with primary high-grade vesicoureteral reflux. Materials and Methods. The study included 107 patients diagnosed with primary high-grade vesicoureteral reflux. Based on the criteria identified during diagnostic cystoscopic examination, indications for specific endoscopic injection techniques were selected. Results. The STING, HIT-1, and HIT-2 techniques were used for endoscopic correction. In this study, the HIT-1 and HIT-2 techniques demonstrated high efficacy rates of 84.3% and 97.3%, respectively. Conclusion. Endoscopic correction methods allow achieving high treatment efficacy in children with primary high-grade vesicoureteral reflux.
Keywords: Primary vesicoureteral reflux
Cite this paper: Raxmatullayev Akmal Abadbekovich, Ergashev Muhammadjon Tursunovich, Selection of an Alternative Endoscopic Treatment Method for Primary High-Grade Vesicoureteral Reflux in Children, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1705-1709. doi: 10.5923/j.ajmms.20261604.33.
Article Outline
1. Introduction
- Primary vesicoureteral reflux (VUR) in children accounts for up to 30% of congenital anomalies of the urinary tract. This pathology is characterized by delayed diagnosis, the need for complex treatment approaches, and a relatively high incidence of postoperative complications [1,3,17].Studies have demonstrated a direct association between VUR in children and recurrent urinary tract infections (UTIs), as well as renal parenchymal scarring. According to research findings, when infection ascends and spreads to the renal pelvicalyceal system, the development of reflux nephropathy is frequently observed. Prolonged or recurrent UTIs lead to inflammatory and fibrotic processes in the renal tissue, ultimately resulting in renal parenchymal scarring and the development of chronic kidney disease [2,4,14].In recent years, endoscopic correction methods have been increasingly used in the treatment of high-grade VUR. The main advantages of this approach include its minimally invasive nature, short rehabilitation period, and low level of surgical trauma. However, in certain cases, endoscopic treatment does not completely eliminate VUR, and open surgical intervention becomes necessary. Nevertheless, fibrotic changes in the tissues of the urinary system observed after endoscopic correction do not complicate subsequent open surgical procedures and do not increase the risk of postoperative complications such as ureteral stricture or obstruction [5,7,15].These factors highlight the importance of early diagnosis, individualized selection of treatment strategies, and improvement of surgical outcomes. Therefore, the development of scientifically grounded approaches for the timely diagnosis and effective management of primary high-grade vesicoureteral reflux in children remains a highly relevant clinical issue [6,8,9].Despite ongoing scientific debate regarding VUR and its consequences, several important aspects have gained consensus among specialists. In particular, bladder dysfunction has been shown to significantly influence VUR outcomes; in some cases, reflux may resolve spontaneously, and not all children require active surgical or pharmacological treatment [10,11,16].In recent years, special attention has been given to risk stratification and patient grouping based on factors such as urinary tract infection, patient age, reflux grade, and bladder function [12,13,18].
2. Study Objective
- To improve the effectiveness of endoscopic correction methods in children with primary high-grade vesicoureteral reflux (VUR).
3. Materials and Methods
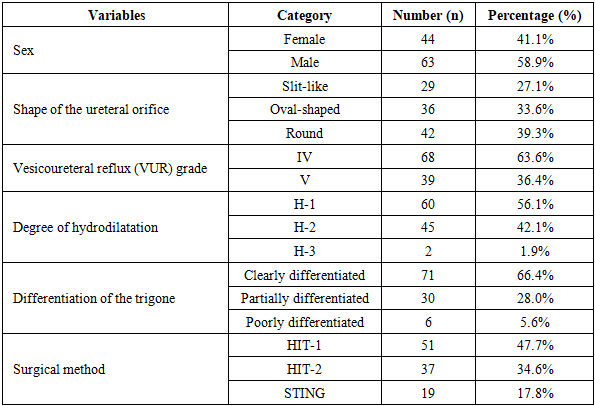
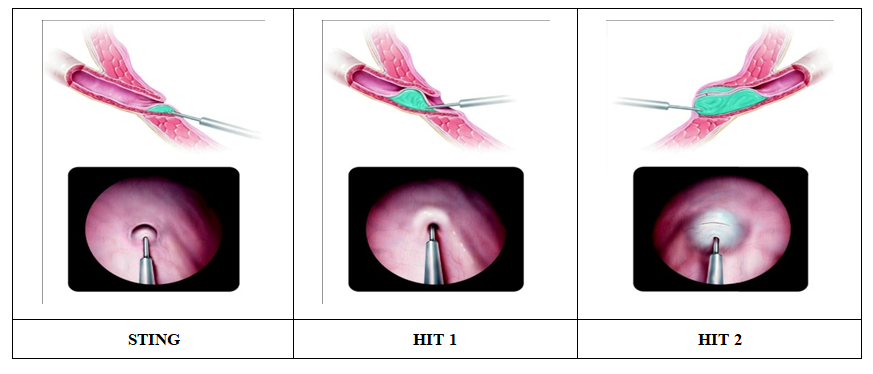
- The study included 107 patients treated for high-grade vesicoureteral reflux at the Department of Urology of the Multidisciplinary Pediatric Clinic of Tashkent State Medical University between 2019 and 2025.Analysis of the reasons for hospital admission among children with primary high-grade VUR showed that the most common presenting complaints were recurrent urinary tract infections and symptoms of pyelonephritis accompanied by fever. To establish a differential diagnosis of the observed clinical manifestations, a set of laboratory and instrumental diagnostic methods was applied.The primary objective of the study was to determine the severity and functional changes associated with primary high-grade vesicoureteral reflux in children and to establish comprehensive diagnostic criteria for selecting the optimal surgical treatment strategy.During cystoscopic examination, the condition of the bladder mucosa (hyperemic, bullous, or trabeculated), the shape of the ureteral orifice (slit-like, oval, or round), and the degree of contraction of the ureteral orifice were evaluated. In cases of high-grade reflux, the ureteral orifice was typically round or funnel-shaped, often accompanied by insufficient contraction and hyperemia of the mucosa.The appearance of the trigone (Lieutaud's triangle) was also found to be directly related to the severity of reflux. In mild reflux, the trigone was clearly delineated, whereas in moderate and severe reflux its borders appeared indistinct or completely undifferentiated, indicating disruption of the normal anatomical structure of the trigone.In patients with high-grade VUR who demonstrated relatively preserved cystoscopic findings—intact trigonal structure, minimal mucosal changes, and mild hydrodilatation—endoscopic treatment methods (HIT-1 or HIT-2) were considered effective. However, in patients with deformation of the ureteral orifice, disrupted trigonal boundaries, and pronounced hydrodilatation insufficiency, pneumovesicoscopic or exploratory ureteral reimplantation procedures were selected (Table 1).
|
 | Figure 1 |
4. Results
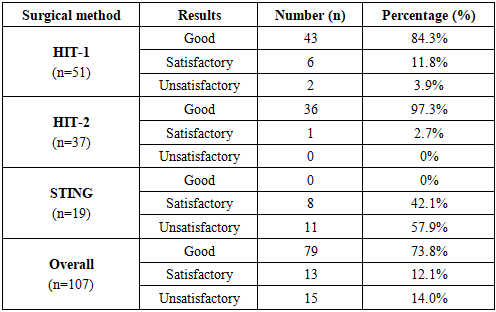
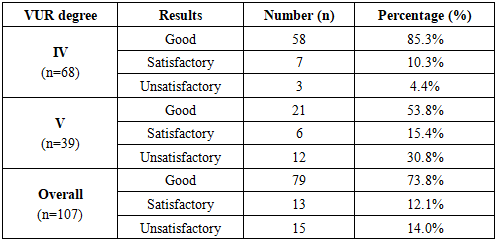
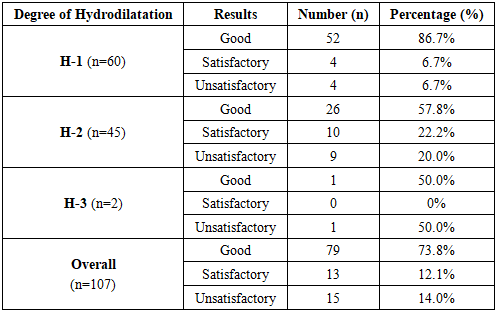
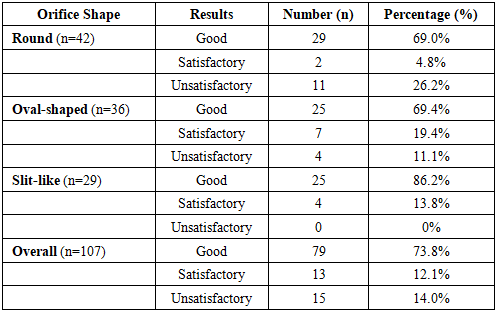
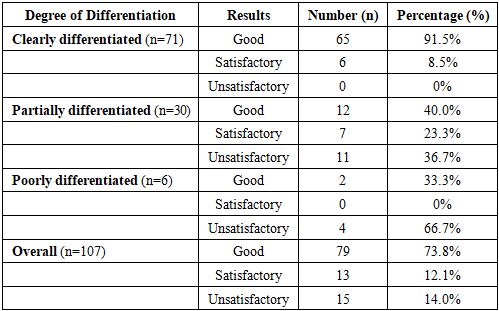
- The outcomes of endoscopic correction using the STING, HIT-1, and HIT-2 techniques were evaluated in all patients and categorized into three groups: good, satisfactory, and unsatisfactory results (Table 2).
|
|
|
|
|
5. Discussion
- The primary aim of this study was to improve the effectiveness of endoscopic correction in children with primary high-grade vesicoureteral reflux (VUR) by using cystoscopic criteria to select the optimal injection technique. The most valuable finding is that the HIT-2 technique achieved a 97.3% success rate, significantly outperforming STING (0% good results) in patients with grade IV–V reflux. Additionally, cystoscopic features such as round ureteral orifices and poorly differentiated trigones were identified as key predictors of treatment failure with less invasive techniques, highlighting the importance of tailoring the surgical approach to individual anatomy.Our findings align with previous studies reporting limited efficacy of STING in high-grade VUR, while the high success of HIT-2 is consistent with authors such as Yilmaz et al., who demonstrated that two-stage implantation better restores the antireflux mechanism. The main limitations of this study are the modest sample size and lack of long-term follow-up data. Future research should focus on larger, multicenter studies to develop a predictive scoring system that integrates both anatomical and functional factors for personalized treatment selection.
6. Conclusions
- In children with high-grade vesicoureteral reflux (VUR), endoscopic correction using polyacrylamide hydrogel (DAM+) was shown to be an effective method for restoring the antireflux mechanism. Accurate assessment of the disrupted antireflux mechanism is of critical importance in managing the disease. Although the STING technique is technically simple and can be performed quickly, the HIT-1 and HIT-2 techniques demonstrated higher efficacy. These methods allowed restoration of the intramural ureteral segment length, physiological reconstruction of the antireflux mechanism, and reduction of the risk of VUR recurrence. Therefore, for cases of high-grade VUR, the HIT-1 and HIT-2 techniques are considered preferable.