-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1690-1695
doi:10.5923/j.ajmms.20261604.30
Received: Mar. 3, 2026; Accepted: Mar. 25, 2026; Published: Apr. 8, 2026

Synergistic Effect of Metroplasty and Autologous Platelet-Rich Plasma in the Treatment of Post-Cesarean Uterine Scar Defects
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLGafurov Jakhongir Mumindjanovich1, Saidjalilova Dilnoza Djavdatovna2
1PhD, Republican Perinatal Center, Head of the Department of Gynecology, Uzbekistan
2Doctor of Medical Sciences, Professor, Tashkent State Medical University, Uzbekistan
Correspondence to: Gafurov Jakhongir Mumindjanovich, PhD, Republican Perinatal Center, Head of the Department of Gynecology, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Over recent decades, the global rate of caesarean section has more than doubled, reaching approximately 24% in Uzbekistan. This rise is largely attributable to tertiary obstetric hospitals and perinatal centers, where high-risk pregnancies are concentrated, including women with severe obstetric and somatic pathology, prior uterine surgery, pregnancies following IVF, and cases complicated by severe preeclampsia. Research objective: To assess the effectiveness of combined metroplasty performed during preconception period in patients with uterine scar dehiscence following caesarean section. Materials and methods: This prospective study included 107 women with a uterine scar after cesarean section who were observed at the Gynecology Department of the Republican Perinatal Center during 2023-2024. Among them, 72 patients were diagnosed with uterine scar dehiscence and underwent metroplasty: 34 with the use of platelet-rich plasma (PRP) and 38 without PRP application. These patients were compared with a control group of 35 women who had a sonographically and clinically competent uterine scar. Results: Combined metroplasty with PRP improved uterine scar healing after caesarean section and was associated with favorable pregnancy outcomes, indicating adequate tissue repair. Conclusion: Preconception assessment of the uterine scar after caesarean section is essential, and when scar defects are identified, metroplasty combined with PRP therapy followed by individualized monitoring and delivery planning improves reproductive outcomes.
Keywords: Uterine scar dehiscence, Caesarean section, PRP therapy, Metroplasty
Cite this paper: Gafurov Jakhongir Mumindjanovich, Saidjalilova Dilnoza Djavdatovna, Synergistic Effect of Metroplasty and Autologous Platelet-Rich Plasma in the Treatment of Post-Cesarean Uterine Scar Defects, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1690-1695. doi: 10.5923/j.ajmms.20261604.30.
Article Outline
1. Introduction
- Caesarean section is one of the most common obstetric operations. Over the past few decades, the frequency of caesarean sections worldwide has more than doubled, and in Uzbekistan it averages about 24% [2,8,9,11,12]. The increase in cesarean section rates is primarily associated with large obstetric hospitals and perinatal centers, which manage a high concentration of patients with severe obstetric pathologies, elevated maternal and perinatal risks, as well as specific groups of pregnant women—those after the procedure in vitro fertilization (IVF), uterine scars from previous cesarean sections or myomectomy, severe somatic diseases, and cases of severe preeclampsia.The presence of scar tissue on the uterus is often an ‘automatic’ indication for repeat caesarean section, during which the frequency of complications increases 3-4 times compared to natural childbirth [1,4,11]. This is why the quality of uterine scar repair after a caesarean section is becoming an increasingly important issue.One of the urgent problems in modern obstetrics is uterine scar failure after cesarean section (CS), the incidence of which has reached an average of 26.4% worldwide over the past 10–15 years [3,5,9]. While cesarean section is undoubtedly a life-saving procedure for certain categories of pregnant women, it is also associated with additional risk factors for postpartum complications. As a result, the subsequent reparative processes in the uterine wall occur under conditions of pronounced tissue ischemia [6,7]. Uterine scar rupture during pregnancy is the most dangerous complication for both the mother and the fetus, and its incidence does not tend to decrease [2].In recent decades, there has been growing research interest in the long-term complications associated with cesarean section, particularly those related to the presence of a uterine scar (such as placenta accreta, cesarean scar pregnancy, uterine rupture, prolonged spotting, dysmenorrhea, chronic pelvic pain, infertility, and others) [4,8,12].Back in 1961, L. Poidevin, using hysterosalpingography (HSG), was the first to identify a wedge-shaped defect in the scar area of the uterus after CS in a non-pregnant woman, which, according to the author, was formed in the process of tissue repair disruption in the postoperative period [10]. Currently, recommendations for the diagnosis and description of the condition of uterine scars without pregnancy are still being developed [6,13,14].The morphological characteristics of the myometrium in non- pregnant condition were assessed in patients with uterine scar after CS. It was found that the scar tissue of patients with local thinning of the myometrium in the scar area on the uterus after CS significantly differs from the scar tissue of patients without local thinning, not only in terms of scar thickness, but also in terms of morphological structure and degree of vascularisation. It has been found that the morphological basis of the uterine scar in patients with local thinning of the myometrium is 55% connective tissue, in the structure of which disorganized muscle fibers are observed [10].The diagnosis of uterine scar dehiscence is always complex and ambiguous, particularly at the stage of pregnancy planning. Usually, neither patients nor clinicians are ready to accept the diagnosis based on just one ultrasound examination. Verification of the diagnosis is carried out in all cases during a consultative examination, using hydrosonography and hysteroscopy [5,14]. Ultrasonography serves as an important method for assessing reparative processes and the integrity of the scar on the operated uterus. Absolute signs of uterine scar dehiscence include: visualization of a complete myometrial defect in the area of the scar in the form of a niche extending from the uterine cavity to the bladder wall or to the serosal surface of the uterus; visualization of an incomplete myometrial defect in the scar area in the form of a niche from the uterine cavity with thinning of the lower uterine segment to 2 mm or less; deformation of the myometrium with retraction from the serosal surface and a niche from the uterine cavity, with thinning of the unaltered myometrium to 2 mm or less. Signs of partial uterine scar dehiscence include visualization of niches and deformations in the scar projection area with myometrial thinning to 4–5 mm or less. Very often, such defects have an irregular slit-like shape and are located both centrally and eccentrically. In some cases, niches and defects may extend into the parametrium. The absence of convincing vascularization in the myometrium on power Doppler imaging may also suggest partial scar dehiscence. In cases of suspected partial scar dehiscence, office hysteroscopy and/or hydrosonography are recommended [10,14]. When these features are identified, surgical treatment—metroplasty—is advised.The incidence of postoperative uterine scar defects can reach up to 63% [8]. Over the past decade, uterine scar repair (metroplasty) following cesarean section has become a widely practiced reconstructive procedure. However, data on methods for modulating reparative activity and promoting the formation of a fully functional scar remain limited in the literature [5,6,7,9]. Studies of the wound repair process in the uterus have made it possible to expand existing knowledge about the course of the wound process and continue the search for technologies to activate full tissue repair [4,12,13].In this regard, during the pregnancy planning stage, patients with a history of cesarean section should undergo ultrasound evaluation of the uterine scar. If a significant defect in the scar area is detected, metroplasty is indicated; the surgical approach may be either laparotomic or laparoscopic. The implementation of modern diagnostic techniques for uterine scar dehiscence, echographic criteria for myometrial healing following various metroplasty techniques, and advanced surgical methods of metroplasty will contribute to improved reproductive outcomes in patients with a history of cesarean section. This can be achieved by reducing pregnancy-related complications (such as miscarriage at various gestational stages and uterine rupture) and increasing the rate of full-term deliveries.
2. Research Objective
- To evaluate the effectiveness of combined metroplasty in the preconception period in patients with uterine scar dehiscence after CS surgery.
3. Materials and Methods
- The study was conducted in several stages. At the first stage of this prospective study, 107 women with a uterine scar after CS who were observed at the Gynecology Department of the Republican Perinatal Center during 2023–2024 were enrolled and evaluated. The main group included 72 women diagnosed with uterine scar dehiscence following CS, while the comparison group consisted of 35 women with a competent uterine scar after CS. Within the main group, patients were further divided into two subgroups based on the treatment approach: Group 1A included 34 women who received platelet-rich autologous plasma (PRP) during surgery. Group 1B included 38 women who underwent metroplasty without the use of PRP. Prior to surgery, written informed consent was obtained from all patients. Transvaginal ultrasound was performed using a Voluson 730 Expert system (General Electric, USA), along with contrast-enhanced magnetic resonance imaging (MRI) of the pelvic organs for vascular assessment. In the absence of sonographic signs of uterine scar dehiscence, but in the presence of symptoms such as menstrual cycle disorders, secondary infertility, or recurrent pregnancy loss, hysteroscopy was performed. If no “niche” was detected during hysteroscopy, the diagnosis of uterine scar dehiscence was not confirmed. All patients with a confirmed diagnosis of uterine scar dehiscence underwent laparoscopic metroplasty combined with PRP therapy during the first phase of the menstrual cycle. In the postoperative period, all patients underwent ultrasound monitoring of the uterine scar on postoperative days 6–7 and after 6 months. The following criteria were used to assess uterine scar integrity in the early postoperative period (days 6–7): absence of deformations, niches, or retraction zones on both the serosal surface and within the uterine cavity; myometrial thickness at the site of the postoperative scar equal to that of the intact surrounding myometrium; absence of hematomas within the scar structure, connective tissue inclusions, or fluid collections; clear visualization of well-structured sutures within the myometrium; adequate blood flow; thickness of the vesico-uterine peritoneal fold less than 5 mm; and absence of hematomas or fluid accumulation beneath this fold [10,11].Assessment of uterine scar integrity six months after metroplasty included the following criteria: absence of deformations, niches, or retraction zones on both the serosal surface and within the uterine cavity; myometrial thickness in the lower uterine segment equal to that of the anterior uterine wall; absence of organized hematomas within the scar structure and connective tissue inclusions; adequate vascularization; normal appearance of the vesico-uterine fold, the Douglas space, and the parametria (without edema, hematomas, or free fluid) [10]. In some cases, hysteroscopy was used to confirm the diagnosis.The exclusion criteria were: uterine myoma, adenomyosis, inflammatory diseases of the female reproductive organs, acute infections of extragenital localization. The examination of women included in the study was conducted in accordance with the National Standard.To obtain platelet-rich plasma (PRP) prior to surgery, 15 ml of venous blood was collected and centrifuged for five minutes at 1500 rpm. The resulting volume of PRP was approximately 12 ml. Following uterine incision repair, tissue infiltration with PRP was performed along the entire length of the incision at both the upper and lower edges. The condition of the uterine scar was evaluated using transvaginal ultrasound (TVUS) on postoperative days 6–7 and after 6 months, using the same parameters assessed preoperatively. At the second stage, if the results of the 6-month follow-up were satisfactory, patients were allowed to proceed with pregnancy planning. The final evaluation of the effectiveness of the combined metroplasty technique was based on the course and outcome of the subsequent pregnancy.Statistical analysis of the results included calculation of the arithmetic mean (M), standard deviation (σ), and standard error of the mean (m) for quantitative variables. To assess the significance of differences in the distribution of qualitative variables, the χ² (chi-square) test and confidence intervals (p-values) were used.
4. Research Results
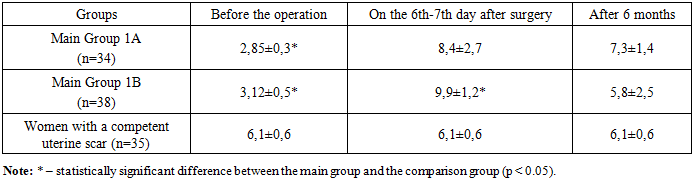
- After assessing the characteristic complaints of the women studied (menstrual cycle disorders (MCD), secondary infertility, miscarriage), an ultrasound examination of the pelvic organs was performed. During TVUS of the scar area on the uterus, in addition to determining its local thinning (‘niche’), the thickness of the scar along its entire length and its homogeneity were measured. Thus, the thickness of the scar on the uterus in the main group averaged 2.85±0.3 mm.In the comparison group, the average scar thickness was 6.1 ± 0.6 mm. The thickness of the myometrium outside the scar area did not differ significantly between the study groups. Among the 72 women with uterine scar dehiscence, 51 (70.8%) showed the presence of a "niche" on ultrasound (Fig. 1), while in the remaining cases, scar heterogeneity and adhesions were observed.
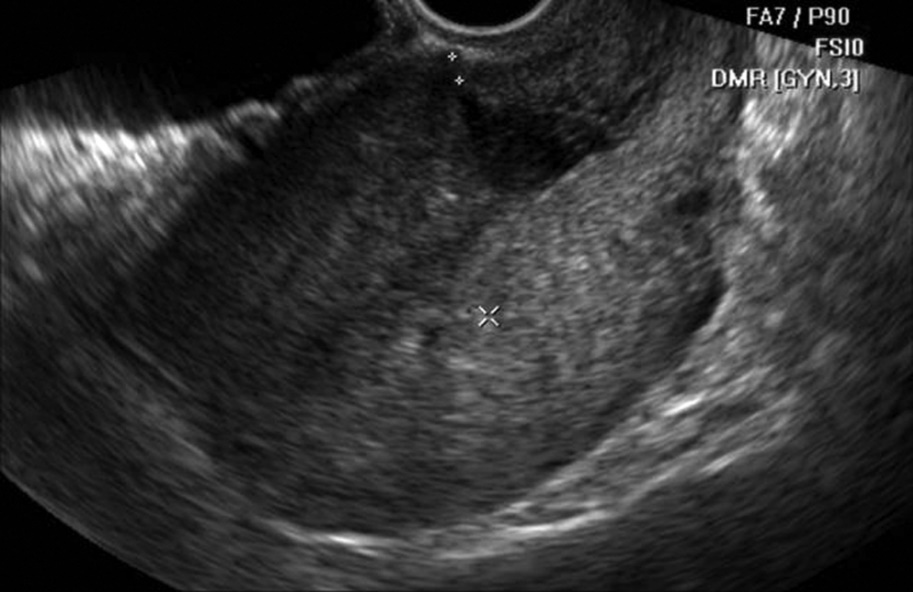 | Figure 1. Patient M., 27 years old, niche symptom (main group) |
|
 | Figure 2. Patient U., 27 years old, 6 days after metroplasty |
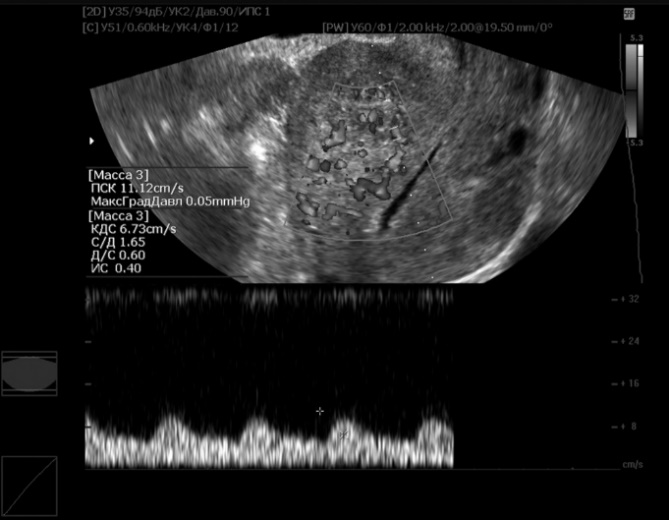 | Figure 3. Patient A., 25 years old, 6 months after metroplasty |
|
5. Discussion
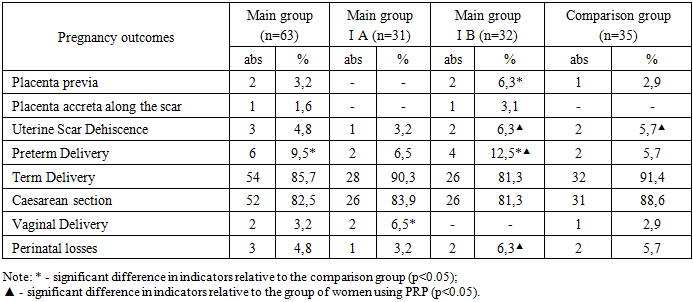
- The results of the study of the course and outcomes of pregnancy showed that the gestational course after metroplasty, in terms of complication rates, did not differ from that of the control group of women with a well-formed uterine scar after cesarean section. A severe complication such as placenta accreta along the scar was observed in only one woman who had undergone metroplasty without the use of PRP during the surgery.Histological analysis revealed notable differences in scar tissue remodeling between the groups. In women who underwent metroplasty with PRP therapy, the scar tissue was characterized by a well-developed smooth muscle component represented by hypertrophied muscle fibers, suggesting more favorable myometrial regeneration. In contrast, specimens from women who underwent metroplasty without PRP, as well as those with a conventionally formed uterine scar, demonstrated predominance of diffuse stromal fibrosis with thin connective tissue layers interspersed between smooth muscle fibers. Additionally, some cases in the non-PRP group exhibited focal subserosal fibrosis associated with adhesive changes, as well as mild perivascular inflammatory infiltration and occasional foreign body granulomas in deeper layers. Overall, these findings suggest that the use of PRP during metroplasty may contribute to improved structural remodeling of the uterine scar, promoting a more pronounced restoration of the muscular component of the myometrium.
6. Conclusions
- 1. During the pregnancy planning stage, patients with a history of cesarean section should undergo transvaginal ultrasound evaluation of the uterine scar. In the absence of ultrasonographic signs of scar insufficiency, but in the presence of clinical symptoms (menstrual cycle disorders (MCD), secondary infertility, or recurrent pregnancy loss), hysteroscopic examination is recommended.2. If a defect of the postoperative uterine scar is detected during the preconception period, metroplasty combined with PRP therapy is indicated. Follow-up evaluation at 6 months post-metroplasty should include pelvic ultrasound and MRI. If the results are satisfactory, pregnancy planning may be allowed.3. A personalized approach to the method of delivery is required for women who have undergone metroplasty. This approach should be based on the condition of the uterine scar, presence of comorbid somatic pathology, the course of the current pregnancy, fetal condition, and the age of the pregnant woman.
Conflict of Interest
- The authors declare no conflict of interest.
ACKNOWLEDGEMENTS
- The authors express their sincere gratitude to the medical staff of the Republican Perinatal Center, including the obstetric, gynecologic, anesthesiology, and neonatal teams, as well as the clinical support personnel, for their invaluable contribution to patient care and data collection.