-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2205-2208
doi:10.5923/j.ajmms.20261604.135
Received: Apr. 5, 2026; Accepted: Apr. 23, 2026; Published: Apr. 30, 2026

High and Ultra-High Anastomoses in Esophagogastric Junction Cancer with Extended Esophageal Involvement
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdikhakimov Abdulla Nusratullaevich1, Aliev Rafikzhan Alidzhanovich2, Aziziy Aziz Abdullaevich3, Mirzaev Hurshid Mirzaevich3, Mutalov Husan Ikramovich3, Ergashev Shohruh Kozimovich3
1Department of Thoracabdominal Surgery, Tashkent regional Branch of RSSPMCOR Uz, Tashkent, Uzbekistan
2Ezgu Niyat Private Medical Clinic, Uzbekistan
3Surgery, Department of Thoracabdominal, Tashkent regional Branch of RSSPMCOR Uz, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Cancer of the esophagogastric junction (GEJ) represents a significant clinical challenge in surgical oncology, accounting for approximately 10-15% of all esophageal and gastric cancers. Tumors involving the esophagogastric junction with extended esophageal involvement require extensive surgical resection to achieve adequate margins and improve oncological outcomes. The proximal location of these neoplasms and their longitudinal spread along the esophageal wall necessitate resection of significant portions of the intrathoracic esophagus, creating unique surgical and reconstructive challenges.
Keywords: Esophagogastric junction cancer, Esophageal cancer, High anastomosis, Ultra-high anastomosis, Extended esophageal involvement, Esophagectomy, Surgical technique, Reconstruction, Gastric conduit, Anastomotic complications, Swallowing function, Quality of life, Postoperative outcomes
Cite this paper: Abdikhakimov Abdulla Nusratullaevich, Aliev Rafikzhan Alidzhanovich, Aziziy Aziz Abdullaevich, Mirzaev Hurshid Mirzaevich, Mutalov Husan Ikramovich, Ergashev Shohruh Kozimovich, High and Ultra-High Anastomoses in Esophagogastric Junction Cancer with Extended Esophageal Involvement, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2205-2208. doi: 10.5923/j.ajmms.20261604.135.
1. Introduction
- High and ultra-high anastomoses are feasible and oncologically justified in GEJ cancer with proximal esophageal extension. Accurate intraoperative determination of the proximal invasion zone, individualized choice of approach, and refinement of anastomotic techniques significantly influence early and long-term outcomes [1]. Gastroesophageal junction (GEJ) cancer surgery is one of the most complex and prognostically unpredictable interventions in the upper gastrointestinal tract, involving manipulations in both the abdominal and pleural cavities, and sometimes in the neck. Such work on "two-..." and sometimes on three floors undoubtedly requires a lot of surgical experience and knowledge [2].Optimal surgical tactics are determined by the degree of tumor invasion of the esophagus, its type according to the Siewert classification, histological structure, stage of the disease and the general somatic status of the patient [6]. Current trends in cardioesophageal cancer surgery are aimed at improving the safety of interventions through the improvement of surgical instruments, the widespread introduction of minimally invasive technologies, the use of intraoperative fluorescence imaging and the introduction of navigation systems for the accurate identification of lymphatic drainage pathways. However, in locally advanced forms of GEJ cancer, the benefits of minimally invasive techniques remain limited. This is due to the strict requirements for oncological ablasticity and the limited range of movements of laparoscopic instruments, especially when there is tumor growth into surrounding structures [3].In order to improve the surgical treatment of CEJ cancer, we attempted to divide patients with a high transition of tumor infiltration into the esophagus according to the level of the applied anastomosis into 3 floors or levels [8].• Low esophageal anastomoses are defined as those constructed at the level of the abdominal and diaphragmatic segments of the esophagus [7];• High anastomoses are those created at the level of the retropericardial segment of the esophagus;• Ultra-high anastomoses are constructed at the level of the subbronchial segment and above [4]. To clarify the exact localization of the pathological process in the esophagus and from a practical point of view, we applied the classification according to Brombard (1956), modified by S.A. Gashelin (1988), recommended by the school of Academician M.I. Davydov, which best meets the requirements of modern oncosurgery (see Fig. 1). Taking into account this classification, the esophagus is divided into 9 segments [5].
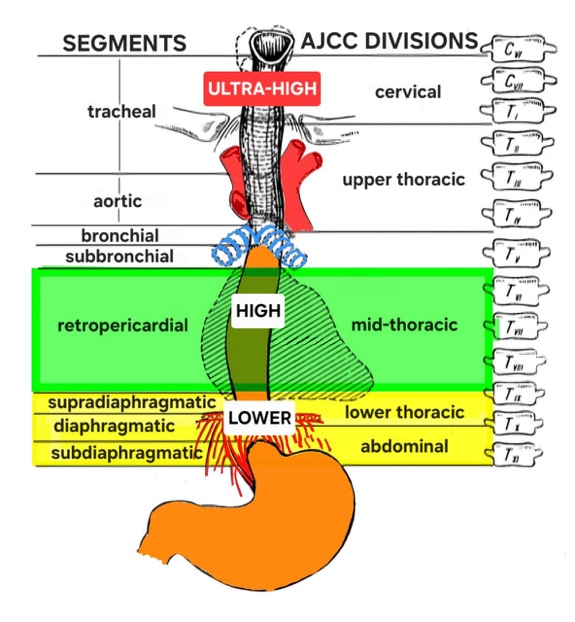 | Figure 1. Classification according to Brombard (1956) as modified by S.A.Gashelin (1988) |
2. Material and Methods
- The basis of the clinical material was the analysis of the results of surgical treatment of 76 patients with GEJ cancer who underwent surgery at the Thoracoabdominal Oncosurgery clinic of the Tashkent Regional Branch of the Russian National Cancer Research Center from 2014 to 2023, that is, over a ten-year period. During the study in these 76 patients, it was found that the C16 (stomach cancer) code, according to ICD-10, was assigned to 45 patients (59.2%), while the C15 (esophageal cancer) code was assigned to 31 patients (40.8%).All patients underwent radical surgery. There were 26 (34.2%) women and 50 (65.8%) men among the patients. The age of the patients ranged from 30 to 73 years (average age 62.4 years).In our study, there were no patients with stage I of the disease. In stage II, only one patient (1.3%) was operated on. The vast majority of patients — 58 cases (76.3%) — underwent surgery at stage III, which reflects the tendency of late detection and locally advanced course of the disease characteristic of GEJ cancer. A special group consisted of patients with stage IV — 17 cases (22.4%). Surgical interventions in this category were performed in a cytoreductive volume with reasonable prerequisites for achieving R0 resection, despite the presence of separate distant metastatic deposits. These situations included limited perigastric or paraesophageal dissemination, potentially subject to removal as part of a single surgical stage. Among them, 8 patients (10%) had distant metastases, whereas in 9 patients (11.8%), stage IV was established based on the local prevalence of the process without confirmed distant deposits. It should be emphasized that in the TNM classification, esophageal cancer can be classified as stage IV not only in the presence of M1, but also in the case of a locally widespread pT4a/bN2 process, which is essential in interpreting clinical data.
3. Results
- Surgery with the formation of an anastomosis exclusively through the abdominal cavity were not considered in the framework of this study due to their fundamental unacceptability in high tumor locations. When analyzing the types of surgical interventions performed in patients with GEJ cancer, the following distribution was found:
|

|
4. Conclusions
- Surgical management of esophagogastric junction cancer is entering a phase of sustained advancement, with a clear trajectory toward improved clinical and oncological outcomes. This progress is underpinned by continuous innovations in surgical technique, increasingly precise radiologic and endoscopic staging, and the integration of multimodal treatment strategies. Centralization of care in high-volume centers, combined with the development of dedicated multidisciplinary teams, has emerged as a critical determinant of outcomes, enabling both technical excellence and optimal perioperative management in this complex patient population.In this context, refined intrathoracic reconstructive approaches, meticulous assessment of conduit perfusion, and adherence to oncologic principles collectively contribute to improved safety and radicality of surgical treatment. Taken together, these advances position modern esophagogastric surgery not only as a technically feasible intervention but as a highly effective cornerstone of curative treatment, capable of achieving meaningful reductions in postoperative morbidity and durable improvements in long-term survival.